Historical Review of Endoscopic Spinal Decompression
*Corresponding Author(s):
Akira DezawaDepartment Of Orthopedic Surgery, Head Dezawa Spine PED Center, Visiting Professor, Teikyo University, Tokyo, Japan
Tel:+81 448443333,
Email:adezawajp@gmail.com
Abstract
Improvements in imaging techniques, along with advancements in optomechanical devices such as 2-mm-thin endoscope, electronic scope, and CCD cameras, and development of new devices such as the high speed drill greatly affected the techniques of minimally invasive endoscopic surgery. In behind the birth of these groundbreaking medical techniques there were engineers who have supported from the beginning. Thus, it is also the history of medical-and-engineering ties between doctors and optical engineers, and past experience becomes a beam of light that shed upon the future.
Primum nil nocere (minimize the invasion) was a concept since the days of Hippocrates, and it has been an everlasting theme for surgeons. Then, a paradigm shift occurred, from the times of microscopes to the times of video endoscope where operators can share the live image with others. With these advancements, surgeons were able to understand the anatomical structures and relative positional relationship of each organs through the endoscope and developed their depth perception through two-dimensional video images. Endoscopic spinal decompression that uses high-definition endoscopic images and can treat a wide range of the spinal column enabled to decrease numbers of complications and faster rehabilitation.
Keywords
Endoscopic spinal decompression; Full endoscopic spine surgery; Minimally invasive spine surgery; Rigid endoscope; Stenosis
INTRODUCTION
Trying to see inside a human body with an instrument was a theme that went in tandem with the development of lenses and image capturing. By looking back at the history, we can foresight the future of minimally invasive endoscopic techniques. History of endoscopy goes way back to 100AD, in which medical instruments that can examine inside the body were discovered in the ruins of Pompei [1,2]. The first time a tube was used to examine the inside of an organism was done in 1805 by Philipp Bozzini. He inserted a tube inside the body, and by using a candle as the light source, he became the first person to examine inside the body. He also tried to examine the inside of the ear, urethra, rectum, and a woman’s bladder by using a 13zoll (35cm) by 5.9 cm sized box-like device called a Lichtleiter (light guide) [3]. Antoine Jean Desormeaux was a French urologist who worked at the Necker Hospital, a hospital still presents in Paris and in 1853, he examined the urethra, bladder, and the rectum using an autoscope. He is the first person to create the phrase endoscope, a device to look inside the body. Known as the father of endoscopy, Desormeaux committed to popularize endoscopy. The light source was made by burning mixture of alcohol and turpentine and reflecting the light into a lens tube. Until the invention of incandescent light bulb by Edison, light source was made by using candles, gas, and turpentine. In 1879, with Edison inventing the incandescent light bulb, the development of endoscopy also found a new light. In 1970, George Smith (1930-) and Willard Boyle (1924-2011) invented the Charged Coupled Device (CCD), which converts light into electrical signals. With this device, images were converted into electrical signals, which then were displayed onto a monitor for everyone to see.
HISTORY OF ENDOSCOPY
Rigid endoscope – semi-flexible endoscope period (1868-1957) (Table 1)
|
Basic principle of the arc lamp discovered, 1802. |
|
1805 Philipp Bozzini: Used a candle |
|
Image fixation on asphalt by Niepce, 1822 |
|
1826 Segalas: Autoscope and candle |
|
silver-coated plates 1837, |
|
1853 Antoine Jean Desormeaux: Endoscope developed |
|
1868 Kussmaul: Esophagogastroscope developed |
|
Luminescent platinum wire 1870, |
|
Dry plates, Maddox, 1871 |
|
1879 Nitze and Leiter: Cystoscope developed |
|
1881 Mikulicz: Rigid gastroscope developed |
|
Electric lighting entered general use in USA, 1883 |
|
Discovery of X-rays, 1895 |
|
Diode vacuum tube, 1904 |
|
1911 H.C. Jacobaeus: Abdominothoracoscope developed |
|
Tetrode vacuum tube, 1912 |
|
1918 Kenji Takagi: Examination inside a cadaver knee joint using the cystoscope Charrier 22 |
|
1920 Zollikofer (in Switzerland): Meteorismusperitonealis achieved using carbon dioxide gas |
|
1921 Eugen Bircher: Report of 18 cases of arthroscopy |
|
1929 Kalk: Abdominoscope developed |
|
Cool-ray lamp with transmission by glassibers, Heinrich Lamm, 1930 |
|
1931 Burman: Arthroscope published in Journal of Bone and Joint Surgery |
|
1932 Schindler (in Germany): Flexible gastroscope developed |
|
UK television broadcast, 1936 |
|
1937 Presentation of Takagi’s endoscopes at the Paris Exposition, 1937 |
|
Invention of silicon transistor, 1947 |
|
Theoretical publication about fiber optics in Nature, Hopkins, 1954 |
Table1: Era of rigid endoscopes (1805 to 1957).
The first person to look inside the stomach of a live person using anesophago-gastroscope was a German doctor by the name of Adorf Kussmaul (1822-1902) in 1868. Using a metal tube with a length of 47cm and a width of 13mm, the process was extremely painful for the patient. The tip was shaped into an oval, but as it was a rigid endoscope, it was not able to bend at all during examination [1]. In 1887, Nitze and an Austrian technician by the name of Josef Leiter developed an urethro-cystoscope that used a molten platinum glow wire as a light source [4,5] (Figure 1).
In 1881, Josef Leiter collaborated with Mikulicz to develop the first widely-used rigid gastroscope [1,5,6]. Afterwards in 1911, Jacobaeus invented the laparo-thoracoscope, enabling the endoscope to reach most of the body’s tube-shaped organs and cavity [7].
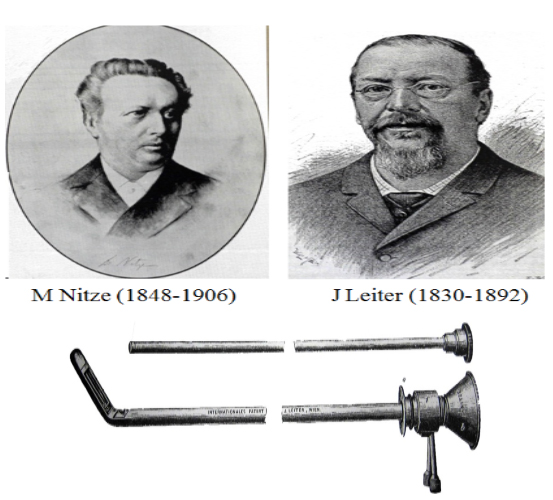 Figure 1: Dr. Nitze and an Austrian engineer, Josef Leiter developed an urethro-cystoscope, J. Leiter received the first international patent for an endoscope.
Figure 1: Dr. Nitze and an Austrian engineer, Josef Leiter developed an urethro-cystoscope, J. Leiter received the first international patent for an endoscope.
The new age of endoscopy arrived in 1932 when Rudolf Schindler invented a flexible gastroscope that had a flexible optic axis, with the help of an optical engineer by the name of Georg Wolf [8]. In 1959, after countless trials, Masaki Watanabe and Tsunekichi Fukuyo invented the the 21st Watanabe Arthroscope, which enabled not only examinations but also surgery and filming inside the joint [9] (Figure 2).
 Figure 2: Dr. Masaki Watanabe and an engineer, TsunekichiFukuyo invented the the “21st Watanabe Arthroscope”.
Figure 2: Dr. Masaki Watanabe and an engineer, TsunekichiFukuyo invented the the “21st Watanabe Arthroscope”.
Cold light source video endoscopy period (1952-now) (Table 2)
|
Fiberscope developed by Hirscowitz, 1957 |
|
Optical fibers developed by Narinder SinghKapany, 1958 |
|
1962 Watanabe: Success in the world’s first arthroscopic meniscectomy,using the Model-21 arthroscope |
|
Integrated-circuit calculator developed, 1964 |
|
1966 Kurt Semm: Automatic pneumoperitoneum device developed |
|
Charged-coupled device developed, 1970 |
|
Computed tomography developed, 1971 |
|
1974 International Arthroscopy Association established. |
|
1975S.Hijikata: Percutaneous nuclectomy developed |
|
Optical communication, 1977 |
|
1983Semm: Abdominoscopic appendectomy carried out |
|
1985 Erich Muhe (in Germany): Abdominoscopic Cholecystectomy carried out |
|
Miniature charged-coupled device developed1986 |
|
1987 Philippe Mouret: Abdominoscopic cholecystectomy |
|
Carried out in Lyons, France. |
|
1994 A robotic arm developed. |
|
1996 Robotic telesurgery carried out using the Internet. |
Table 2: Era of cool-ray lamps and videoendoscopy (1957 to present).
Fourestier developed the cold light fiberglass in 1952 [10]. The technical advancement of the endoscopy accelerated with the development of the quartz rod lens by Hopkins [11], a lens still used today. This incorporates a new theoretical concept of light transmission called the total internal reflection, and this made it possible for the light to be transmitted inside the endoscopy lens without lowering the luminosity. Hopkins’ “Rod Lens” and the flexible light fiber scope enabled the image to be brighter and clearer [12]. In 1970, by using CCD camera that converts light into electrical signals, operations were done by multiple surgeons using TV monitor displays, and the development of the CCD camera accelerated the development and the popularization of the endoscope. Even now, small-sized CCD camera and robots are continued to be in development to miniaturize video endoscopy with clearer resolution.
HISTORY OF ENDOSCOPIC SPINAL DECOMPRESSION TECHNIQUES
Each type of endoscopeis categorized depending on the thinness (Table 3)
|
Classification from endoscopy |
|
Fullendoscopy |
|
Tubular surgery with endoscopy |
|
Laparoscopy |
|
Retroperitoneoscopy |
|
Thoracoscopy |
|
Epiduroscopy |
|
Classification of the method to maintain a space |
|
constant saline irrigation |
|
pneumoperitoneumwith CO2gas |
|
natural cavity |
|
Decompression classification from an approach |
|
Inter laminal |
|
Uniportal bilateral decompression |
|
Biportal bilateral |
|
Trans spinous process [13] |
|
Translaminar [14-18] |
|
Transpedicular [19] |
|
Transforaminal [20,21] |
|
Transiliac [22] |
|
Transsacral [23] |
|
Decompression classification from pathological condition |
|
Central stenosis |
|
Lateral recess stenosis |
|
Foraminal stenosis |
|
Extraforaminal stenosis |
Table 3: Classification of endoscopes used in decompression techniques.
PELD (Percutaneous Endoscopic Lumbar Discectomy) is an optical technique innovation expanded from the PN (Percutaneous Nucleotomy) method, and a rigid-type endoscopy called Full endoscopy is used for the spine. It is also used in uniportal bilateral decompression of the thoracic spine OYL resection, and biportal bilateral decompression is also in consideration.
Although tubular surgery with assistant of endoscopy (an approach similar to when using the miscroscope) expanded into a technique suitable for the posterior region [24-26], as it is a natural cavity, a suction tube becomes necessary, and there is a limit to the size of the working channel. For the anterior region, both anterior lumbar discectomy and fusion during laparoscopy of aeroperitoneum and retroperitoneoscopy uses endoscope as a support for lateral approach. Also, this technique is used in VATS and applied during the decompression andcorrection of thoracic and thoracolumbar transitional vertebrae.
Methods to sustain the cavity are categorized into full endoscopy (sustains by flowing saline into the cavity [27]). Laparoscopy (uses CO2 gas to sustain the cavity [28]), VATS: Video-Assisted Thoracic Surgery (uses a small natural cavity instead of saline to sustain the cavity [29,30]), tubular surgery (METRx tube [31,32]), and abdominal wall lifting [33].
Full Endoscopic Spine Surgery
In 1975, Hijikata used a contrast needle to enlarge the surrounding cavity and set up a standard cannula (inner diameter 3.0m, outer diameter 3.5mm, 2.6mm) under fluoroscopic guidance [34,35]. This led to the devisal of PN method (Percutaneous Nucleotomy), a method to extract the nucleus pulposus of the intervertebral disc post-laterally. Kambin used a 4mm Craig cannula. In 1988, Pravis Kambin suggested that a triangular area surrounded by the exiting root, traversing nerve root, and the end plate of the lower vertebral body is safe for endoscopic spine surgery [36-38]. Currently, technique that fully utilizes this triangle by conducting until the pedicle is popularized (Figure 3) [27]. Onik resected the intervertebral disc using a mechanical suction tube in which the outer diameter was 2.5mm [39]. Foraminoscope (Field Lens of 6 degrees) designed by Hans-Jorg Leu was utilized for 21 years until 2012 [40]. YESS system created by Tony Yeung consists of a 2.5mm surgical instrument, washing channel, multi channel used for rod lens, and an egg-shaped endoscopy. In particular, the inside-out concept suggested by him was safe and easy to perform even for beginners, as decompression and extraction of the spinal cord herniation is done gradually by going into the avascular area of the intervertebral disc [41,42]. Contrary to this, the outside-in method proposed by Hoogland is complicated and needs much practice to control hemorrhage, as this method directly decompresses the intervertebral disc herniation by resecting parts of the pedicle and the zygapophysial joint transforaminal [43]. The strong endoscopic technique performed by Rutten et al. enabled decompression to be done even to the lateral canal and the hidden zone of MacNab [44-47]. Now, decompression techniques using endoscopy for wide areas of the spine, from the cervical to the lumbar area and from the anterior to the posterior area, is being popularized. Furthermore, it is started to be applied in decompression techniques of the anterior/posterior areas of the cervical spine and yellow ligament resection of the thoracic spine [48].
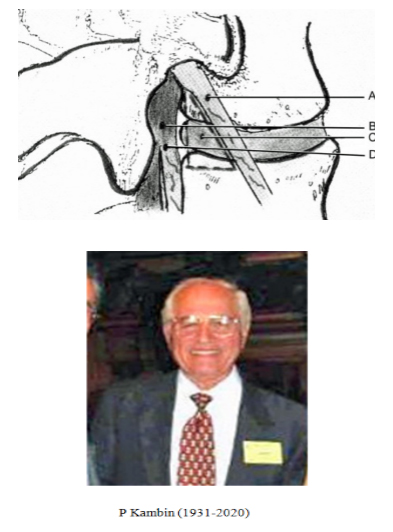 Figure 3: Illustration showing the boundaries of the Kambin triangular working zone: A: Exiting root, B: Dural sac C: Intervertebral disc, D: Traversing root.
Figure 3: Illustration showing the boundaries of the Kambin triangular working zone: A: Exiting root, B: Dural sac C: Intervertebral disc, D: Traversing root.
Pravis Kambin suggested that a triangular area surrounded by the exiting root, traversing nerve root, and the end plate of the lower vertebral body is safe for endoscopic spine surgery. Currently, technique that fully utilizes this triangle by conducting until the pedicle is popularized.
Tubular surgery with assistant of endoscopy
In 1997, Forely and Smith performed a surgery where they extracted a herniation in the intervertebral disc by inserting an 18mm diameter microendoscopy (MED) [31,32]. Furthermore, vertebral arch resection was done by using a technique called the Destando syste [49] and Easy GO.
Laparoscopic (retroperitoneoscopic) lumbar decompression surgery technique
Decompression and fixation under pneumoperitoneum started in 1991 [28]. Furthermore, retroperitoneoscopy by lifting was performed. It became possible to decompress by dividing or moving the psoas major muscle anteriorly [33]. Also, at one point, operation performed anteriorly was done actively for thoracic spine herniation and degenerative diseases [29].
SUMMARY
Future direction
Until now, popularization and advancements of the endoscopic spinal surgery was affected by the ability of the operator to understand the anatomical structure and the relative positional relationship of each organs under endoscopy, and the ability to see the depth perception from a 2-dimentional video monitor. Also, acquiring hand-eye coordination under magnified images and organ sensation such as bone, ligament, and nerves, and leading technology such as the AI Navigation robotics will become the gold standard for endoscopic spinal decompression. In particular, decompression techniques such as the full endoscopic technique will likely be developed through meta-analyses and randomized clinical trials more in the future for lesions where the diameter is small and microscope cannot be used [50].
Improvements of the endoscopy in recent times are mesmerizing, decreasing the chance of approach-induced disabilities by making and sustaining a cavity using a dilator and using a high-resolution VTR image endoscope. Evolving from the traditional intervertebral disc resection surgery using a microscope, the current method can reach the lesion precisely by substantially thinning the working channel and still have a similar performance as the traditional method.
The goal is utilizing the limited cavity as much as possible and obtain a clear visionary field to complete the surgery as fast and safe as possible. With the education system being standardized, minimally invasive techniques will provide a safe and nice treatment method for the people in the 21st century.
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.
FUNDING STATEMENT
The authors declare that their article was not funded and financially supported by anybody or any corporation.
REFERENCES
- Reuter MA, Reuter HJ, Engel RM (1999) History of : an illustrated documentation : Vol. I – IV. Kohlhammer, Stuttgart, Germany.
- McHenry LC (1969) Garison’s History of neurology. Charles C Thomas, Springerfield, USA.
- Bozzini P (1806) Light conductor, an invention for viewing internal parts and diseases, together with illustrations. J Pract Med Surg 24: 107-124.
- Nitze M (1879) Uebereineneue Beleuchtungsmethode derHohlen des menschlichen Korpers. Weiner med 26: 851-858.
- Leiter J (1880) Elektro-endoskopische Instrumente. Beschreibung und Instruction zur. W. Braumüller & Sohn, Wien, Paris.
- Mickulcz J (1883) Uebereinengeheilten Fall von Magenresektionnebst Bemerkungen uber emn Gastroskopisches Symptomes des Magencarcinomas. Wienermed 33: 705-708.
- Jacobaeus HC (1910) Possibility of the use of the cystoscope for investigations of serious cavities. Munich Med Wochenshrift 57: 2090-2092.
- Schindler R (1966) Gastroscopy: The Endoscopic Study of Gastric Pathology (2nd). Hafner, New York, USA.
- Watanbe W, Takeda S, Ikeuch H (1957) Atlas of Arthroscopy, Igakushoin Ltd, Tokyo, Japan.
- Fourestier M, Ennuyer A, Chamouard J (1964) Endoscopic Exploration of the Rhinopharynx by the so-called double light guide Pharyngo-laryngoscope”Sem Hop 8: 2296-2299.
- Hopkins HH, Kapany NS (1954) A Flexible Fibrescope using Static Scanning. Nature 173: 39-41.
- Hirschowitz BI (1958) Demonstration of a new gastroscope, the fiberscope. Gastroenterology 35: 50-53.
- Mayer HM, Brock M (1993) Percutaneous endoscopic discectomy:surgical technique and preliminary results compared to microsurgical discectomy. J Neurosurg 78: 216-225.
- Shibuya I, Dezawa A, Urayama S, Nakamura S (2018) Surgical treatment of a lumbar aneurysmal bone cyst using percutaneous endoscopic lumbar discectomy. Eur Spine J 27: 368-374.
- Sairyo K, Sakai T, Higashino K, Inoue M, Yasui N, et al. (2010) Complications of endoscopic lumbar decompression surgery. Minim Invasive Neurosurg 53: 175-178.
- Dezawa A, Mikami H, Sairyo K (2012) Percutaneous endoscopic translaminar approach for herniated nucleus pulposus in the hidden zone of the lumbar spine. Asian J Endosc Surg 5: 200-203.
- De Antoni DJ, Claro ML, Poehling GG, Hughes SS (1996) Translaminar lumbar epidural endoscopy: anatomy, technique, and indications. Arthroscopy 12: 330-334.
- Oertel JM, Burkhardt BW (2019) Endoscopic Translaminar Approach for Resection of Migrated Lumbar Disc Herniation. World Neurosurgery 128: 365-368.
- Ringer AJ, Bhamidipaty SV (2013) Percutaneous access to the vertebral bodies: a video and fluoroscopic overview of access techniques for trans-, extra-, and infrapedicular approaches. World Neurosurg 80: 428-435.
- Kim HS, Sharma SB, Raorane HD (2019) How I Do It? Transforaminal Endoscopic Decompression of Intraspinal Facet Cyst. Acta Neurochir 161: 1895-1900.
- Mikami Y, Nagae M, Ikeda T, Tonomura H, Fujiwara H, et al. (2013) Tubular surgery with the assistance of endoscopic surgery via midline approach for lumbar spinal canal stenosis: a technical note. Eur Spine J 22: 2105-2112.
- Choi G, Kim JS, Lokhande P, Lee SH (2009) Percutaneous endoscopic lumbar discectomy by transiliac approach: a case report. Spine 34: 443-446.
- Gillespie G, MacKenzie P (2004) Epiduroscopy--a review. Scott Med J 49: 79-81.
- Mixter WJ, Barr JS (1934) Rupture of the intervertebral disc with involvement of the spinal canal. The New England Journal of Medicine 211: 210-214.
- Love JG (1939) Removal of the protruded interlaminar discs without laminectomy. Mayo Clinic Proceedings 14: 800.
- Yasargil MG (1977) Microsurgical Operation of Herniated Lumbar Disc. Lumbar disc adult hydrocephalus. Springer, Heidelberg, Germany.
- Kambin P, Nixon J, Chait A, Schaffer J (1988) Annular protrusion: pathophysiology and roentgenographic appearance. The Spine Journal 13: 671-675.
- Obenchain TG (1991) Laparoscopic lumbar discectomy: case report. J Laparoendosc Surg 3: 145-149.
- Mack MJ, Regan JJ, Bobechko WP, Acuff TE (1993) Application of thoracoscopy for disease of the spine. Ann Thorac Surg 56: 736-738.
- Ebara S, Kamimura M, Itoh H, Kinoshita T, Takahashi J, et al. (2000) A new system for the anterior restoration and fixation of thoracic spinal deformities using an endoscopic approach. Spine 25: 876-883.
- Foley KT, Smith MM. Microendoscopic discectomy. Techniques Neurosurg1997; 3: 301-307.
- Perez-Cruet MJ, Foley KT, Isaacs RE, Rice-Wyllie L, Wellington R, et al. (2002) Microendoscopic lumbar discectomy: technical note. Neurosurgery 51: 129-136.
- Dezawa A, Yamane T, Mikami H, Miki H (2000) Retroperitoneal laparoscopic lateral approach to the lumbar spine: a new approach, technique, and clinical trial. J Spinal Disord 13: 138-143.
- Hijikata S (1975) A method of percutaneous nuclear extraction. Journal of Toden Hospital 5: 39-42.
- Hijikata S (1989) Percutaneous nucleotomy. A new concept technique and 12 years' experience. Clin Orthop Relat Res 238: 9-23.
- Kambin P, Sampson S (1986) Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin Orthop Relat Res 207: 37-43.
- Kambin P, Bracer MD (1987) Percutaneous posterolateral discectomy. Anatomy and mechanism. Clin Orthop Relat Res 223: 145-154.
- Kambin P, Schaffer JL (1989) Percutaneous lumbar discectomy. Review of 100 patients and current practice. Clin Orthop Relat Res 238: 24-34.
- Onik G, Shang YL, Maroon JC (1990) Automated percutaneous biopsy in postoperative diskitis: a new method. AJNR Am J Neuroradiol 11: 391-393.
- Leu HJ, Hauser R (1996) Die perkutan posterolaterale Foraminoskopie : Prinzip, Technik und Erfahrungen seit 1991. Arthroskopie 9: 26-31.
- Tsou PM, Yeung AT (2002) Transforaminal endoscopic decompression for radiculopathy secondary to intracanal noncontained lumbar disc herniations: outcome and technique. The Spine Journal 2: 41-48.
- Yeung AT, Yeung CA (2003) Advances in endoscopic disc and spine surgery: foraminal approach. Surgical Technology International 11: 255-263.
- Hoogland T, Schubert M, Miklitz B, Ramirez A (2006) Transforaminal posterolateral endoscopic discectomy with or without the combination of a low-dose chymopapain: a prospective randomized study in 280 consecutive cases. Spine 31: 890-897.
- Ruetten S, Komp M, Merk H, Godolias G (2009) Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: a prospective, randomized, controlled study. Journal of Neurosurg Spine 10: 476-485.
- Komp M, Hahn P, Merk H, Godolias G, Ruetten S (2011) Bilateral operation of lumbar degenerative central spinal stenosis in full-endoscopic interlaminar technique with unilateral approach: Prospective 2-year results of 74 patients. J Spinal Disord Tech 24: 281-287.
- Komp M, Hahn P, Ozdemir S, Merk H, Kasch R, et al. (2014) Operation of lumbar zygoapophyseal joint cysts using a full-endoscopic interlaminar and transforaminal approach: prospective 2-year results of 74 patients. Surg Innov 21: 605-614.
- Ruetten S, Hahn P, Oezdemir S, Baraliakos X, Merk H, et al. (2018) Full-endoscopic uniportal decompression in disc herniations and stenosis of the thoracic spine using the interlaminar, extraforaminal, or transthoracic retropleural approach. J Neurosurg Spine 29: 157-168.
- Ruetten S, Hahn P, Oezdemir S, Baraliakos X, Godolias G, et al. (2018) Operation of soft or calcified thoracic disc herniations in the full-endoscopic uniportal extraforaminal technique. Pain Physician 21: 331-340.
- Destandau J (1999) A special device for endoscopic surgery of lumbar disc herniation. Neurol Res 21: 39-42.
- Dowling Á, Lewandrowski KU, da Silva FHP, Parra JAA, Portillo DM, et al. (2020) Patient Selection Protocols for Endoscopic Transforaminal, Interlaminar, and Translaminar Decompression of Lumbar Spinal Stenosis. J Spine Surg 6: 120-132.
Citation: Dezawa A, Dezawa T (2020) Historical Review of Endoscopic Spinal Decompression. J Phys Med Rehabil Disabil 6: 055.
Copyright: © 2020 Akira Dezawa, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.