Journal of Alternative Complementary & Integrative Medicine Category: Medicine
Type: Case Report
Holographic Kinetics for Clinically Diagnosed Suicidal, Depressed, PTSD Military Veterans: Case Study
*Corresponding Author(s):
Antoine ChevalierUniversity Of Natural Health, IN And NIH, Bethesda, MD, USA; 21010 South Bank St, #5050, Sterling, VA 20165, United States
Tel:+1 3017688384,
Email:antoine@healedandhappy.net
Received Date: Nov 22, 2017
Accepted Date: Dec 23, 2017
Published Date: Dec 29, 2017
Abstract
Introduction: This case study offers a detailed analysis and a potential non invasive holistic sustainable solution to the current international mental health crisis of the military veterans.
Case: The patient is a 34 years old military veteran, who has been clinically diagnosed as both suicidal and depressed. The patient has been living with Post Traumatic Stress Disorder (PTSD) since 2006 following 27 months of active duty military service in Iraq. Since 2012, he has halted usage of all medications. He has tried almost all forms of allopathic and holistic medicines available. However, nothing has worked until he received a Holographic Kinetics (HK) treatment in September 7th, 2017. Since then, he is 100% better.
Results: The patient experienced more than 50% relief regarding the symptoms of both his depression and suicidal ideation, and less than 50% relief of his PTSD symptoms after only three days following a single 90 minute treatment. The treatment is known as “Holographic Kinetics”, a mental health Modality originated from Australia. Three weeks following the treatment, the patient was 100% symptom free. Almost 5 months after the session, he is symptom free.
Conclusion: This case study reflects a significant and sustainable improvement in both frequency and intensity of the symptoms of PTSD, depression and suicidal ideation. The results deserve attention and more research. We also need to assess different ways of scientifically measuring before and after treatments. The intent is to start a suicidal prevention military veterans research project.
Case: The patient is a 34 years old military veteran, who has been clinically diagnosed as both suicidal and depressed. The patient has been living with Post Traumatic Stress Disorder (PTSD) since 2006 following 27 months of active duty military service in Iraq. Since 2012, he has halted usage of all medications. He has tried almost all forms of allopathic and holistic medicines available. However, nothing has worked until he received a Holographic Kinetics (HK) treatment in September 7th, 2017. Since then, he is 100% better.
Results: The patient experienced more than 50% relief regarding the symptoms of both his depression and suicidal ideation, and less than 50% relief of his PTSD symptoms after only three days following a single 90 minute treatment. The treatment is known as “Holographic Kinetics”, a mental health Modality originated from Australia. Three weeks following the treatment, the patient was 100% symptom free. Almost 5 months after the session, he is symptom free.
Conclusion: This case study reflects a significant and sustainable improvement in both frequency and intensity of the symptoms of PTSD, depression and suicidal ideation. The results deserve attention and more research. We also need to assess different ways of scientifically measuring before and after treatments. The intent is to start a suicidal prevention military veterans research project.
Keywords
Depression; Functional MRI; Holographic Kinetics; Mental health; Military veterans; Post Traumatic Stress Disorder (PTSD); SPECT imaging; Suicide
INTRODUCTION
THE MILITARY VETERAN MENTAL HEALTH CRISIS
Of all countries in the world, the United States is the most concerned by this issue. The US has become a country that is constantly at war. This situation has created a crisis amongst our veterans. The main issue being the lack of access to critical mental health services which may lead to suicidal behavior, especially among young military veterans who have completed multiple deployments to Afghanistan and Iraq [1]. Recent data on suicide rates among Army veterans, reported by the Department Of Defense (DOD), showed an increase of more than 18% from 2011 to 2014 [2]. The Department of Veteran Affairs (DVA) is now struggling to find solutions to this national crisis for our veterans. Veterans experience mental health issues such as PTSD, depression and suicidal ideations at a higher percentage than the general public. Despite treatments, the afflictions do not seem to be decreasing. Based on data collected in 2012, VA estimated that there are roughly 22 suicides committed per day by veterans only further proving how large of an issue this is [3].
Other publications indicate that in 2014, an average of 20 Veterans a day died from suicide. In 2016, this number varied between 20-22. In comparison to civilian adults, the data represents a 21 percent statistically significant higher risk of suicide for veterans [4]. From 2001 to 2014, the civilian suicide rate rose about 23.3 percent, yet the rate of suicide among veterans was greater than 32 percent. Female veterans are even more at risk with their suicide rates rising by more than 85 percent over that time period in comparison to approximately about 40 percent for civilian women [4,5].
We are all proud of our veterans and what they do for us, however we are not reciprocating our responsibilities to them, for we are clearly failing them. This is due to the fact that mental health is a difficult issue to tackle simply because it is more complicated than treating physical ailments.
More and more research further proves that the current methods of treatment for mental health issues such as PTSD, depression and suicidal ideations are ineffective. This lack of treatment largely contributes to the astounding average of 22 veteran suicides per day [4,6-10]. The goal of this publication is to illustrate and highlight that there are multiple ways to treat and measure these. Nevertheless, the treatments and assessments of these illnesses are not as effective as they should be.
Per the Nebraska Department of Veterans Affairs, 7.8% of all Americans will suffer from PTSD at some point in their lives. In comparison, 30% of all veterans will experience PTSD [11]. Veterans are more prone to acquiring PTSD symptoms due to the disturbing nature of being in a war zone. Per the US Department of Veterans Affairs, there are two types of measures used for PTSD evaluations [11]. The first is a structured interview known as the Clinician-Administered Scale (CAPS), and the second is known as the structured clinical interview for DSM [12]. There is a severity rating from 0, which means PTSD symptoms are absent, and five, which means the symptoms are extreme. Also, “when choosing an instrument or structured clinical interview to assess depression or PTSD, attention to the instrument’s reliability and validity is essential. There are two primary domains of reliability (internal consistency and test-retest) and three primary domains of validity (construct, criterion and content) that are often tested and reported” [13]. Oftentimes, self-reported PTSD tests will be followed up by a clinician who can then further evaluate the veteran before and after treatment [5]. At this point in time, trauma-focused psychotherapy and antidepressants are the main ways to treat PTSD. Antidepressants are able to alleviate most PTSD symptoms [14]. Pharmaceuticals help, but alternative treatment may be more effective in addressing root issues. It is becoming more and more important to prioritize researching other alternative treatments, such as Holographic Kinetics to actually help the patient overcome their issues.
Other publications indicate that in 2014, an average of 20 Veterans a day died from suicide. In 2016, this number varied between 20-22. In comparison to civilian adults, the data represents a 21 percent statistically significant higher risk of suicide for veterans [4]. From 2001 to 2014, the civilian suicide rate rose about 23.3 percent, yet the rate of suicide among veterans was greater than 32 percent. Female veterans are even more at risk with their suicide rates rising by more than 85 percent over that time period in comparison to approximately about 40 percent for civilian women [4,5].
We are all proud of our veterans and what they do for us, however we are not reciprocating our responsibilities to them, for we are clearly failing them. This is due to the fact that mental health is a difficult issue to tackle simply because it is more complicated than treating physical ailments.
More and more research further proves that the current methods of treatment for mental health issues such as PTSD, depression and suicidal ideations are ineffective. This lack of treatment largely contributes to the astounding average of 22 veteran suicides per day [4,6-10]. The goal of this publication is to illustrate and highlight that there are multiple ways to treat and measure these. Nevertheless, the treatments and assessments of these illnesses are not as effective as they should be.
Per the Nebraska Department of Veterans Affairs, 7.8% of all Americans will suffer from PTSD at some point in their lives. In comparison, 30% of all veterans will experience PTSD [11]. Veterans are more prone to acquiring PTSD symptoms due to the disturbing nature of being in a war zone. Per the US Department of Veterans Affairs, there are two types of measures used for PTSD evaluations [11]. The first is a structured interview known as the Clinician-Administered Scale (CAPS), and the second is known as the structured clinical interview for DSM [12]. There is a severity rating from 0, which means PTSD symptoms are absent, and five, which means the symptoms are extreme. Also, “when choosing an instrument or structured clinical interview to assess depression or PTSD, attention to the instrument’s reliability and validity is essential. There are two primary domains of reliability (internal consistency and test-retest) and three primary domains of validity (construct, criterion and content) that are often tested and reported” [13]. Oftentimes, self-reported PTSD tests will be followed up by a clinician who can then further evaluate the veteran before and after treatment [5]. At this point in time, trauma-focused psychotherapy and antidepressants are the main ways to treat PTSD. Antidepressants are able to alleviate most PTSD symptoms [14]. Pharmaceuticals help, but alternative treatment may be more effective in addressing root issues. It is becoming more and more important to prioritize researching other alternative treatments, such as Holographic Kinetics to actually help the patient overcome their issues.
HOLOGRAPHIC KINETICS
Holographic Kinetics (HK) is one of the most advanced and unique modality available today. It is based on the ancient Aboriginal knowledge of the laws of LORE and 50 years of research [15]. Steve Richards, the founder of holographic kinetic therapy technique is of aboriginal descendant. He was awarded the 2005 Life Award, Certificate of Commendation by Suicide Prevention Australia. Steve was nominated for the Human Rights Medal Award in 2005 and 2006. He was also nominated for Australian of the Year in 2007 as acknowledgement of the results for the outstanding achievements using the Holographic Kinetics Therapy Technique. HK is not in any way likened to other therapies. It is not hypnosis. It looks at the body as a whole, accessing cellular memory passed down from generations (including trauma) and the cause and effect of events. Thoughts and emotions set up in the past and present affect the cycles of the future. These events, thoughts and emotions are trapped in the body today, affecting our lives and causing us to continue repeating the cycles of life patterns within their own dimension of time, which we can become stuck in. The HK practitioner understands the power of the subtle bodies in the creation and removal of internal created realities which are considered the original causes of mental illnesses. The HK practitioner is able to correct imbalances in the energy field, mind and body of the patient.
Just as there is an above, there is a below-just as there is an internal invisible world, there is an external visible world-and there is always the point zero of the observer (man’s conscious choice) that is positioned between the two-all imbalances occur in the invisible mind of man first and transmute into the visible as an effect of the imbalance. Visible effects can include anxiety, depression, suicidal thoughts, PTSD, Bi Polar, ADD, ADHD, stress, fear, anger, guilt, sexual problems and self-punishment to name a few. Holographic Kinetics aims assist a patient in accessing the causes of these imbalances, so they are able to bring those imbalances back into balance to remain in a state of homeostasis permanently once they have been addressed properly.
Holographic Kinetics uses the natural law of causality in action-and-reaction sequences [16]. Causality is commonly defined as the relationship between causes and effects [17,18]. It is considered to be fundamental to all natural science, especially physics, philosophy, statistics and modern experimental psychology [16]. Based on Minkowski spacetime scientific work, causality means that an effect can occur from a cause which is in the back (past) light cone of an event.
Similarly, a cause can have an effect outside its front (future) light cone [19,22]. The action-reaction pendulum of cause and effect feeds an invisible dimension within the internal world of a humans energy field, creating a visible imbalance (anxiety, depression, etc.,) which needs to be brought back to null point zero vector observer within man’s awareness by waking up to his responsibility of the metaphysical consequences of his own creation upon its own separate dimension of time [21,22]. Only then, will man’s own imbalances be brought back to balance and the effect (mental illness) will finally cease to exist [15].
Kinetic energy is a free-flowing, constant energy, inside and around us, until captured by thoughts. Holographic Kinetics is not limited to this physical dimension, but has an awareness of multi-dimensions and sees man as a multi-dimensional being in a multi-dimensional world, consisting of multiple parts of the human form, in multiple dimensions that need to be cleared. This includes the Spirit and the Soul. Under “Royal commission in the bringing them home report” it states;
One of the fundamental aspect of a hologram is any part of the hologram contains the whole in the form of fractals of stored information. Consequently, a piece of a long-term memory is equally distributed over a dendritic arbor so that each part of the dendritic network contains all the information stored over the entire network of the genetic hereditary lines of the mother and father or beyond (epigenetics) and/or long term experience memories attached to the life force of the patient, coming through time [23-31].
A well trained and experienced Holographic Kinetic practitioner can assist the life force of the patient in accessing internal hyperspace within the patient, where all things become omnipresent, omnipotent and omniscient within their own separate dimension of reality. In Aboriginal culture this is known as the Spirit. (the internal life form, the spark of life) Different to the Psych or Soul, (the external experience) stored as memory, within the cells. Therefore, the practitioner can successfully assist the client to access and clear, their created reality by correcting in invisible the original cause of the visible effect, that is affecting the patient at themoment, within its own dimension of time, of the treatment. The difference between the other treatments and this modality is the permanent improvement and positive outcomes you achieve as a practitioner for the patient [15]. A Holographic Kinetics practitioner recognizes and addresses successfully the multi-dimensions of man.
You must deal with changing the self-destructive processes, these inner patterns that erode the self and mental well-being [34,35].
Just as there is an above, there is a below-just as there is an internal invisible world, there is an external visible world-and there is always the point zero of the observer (man’s conscious choice) that is positioned between the two-all imbalances occur in the invisible mind of man first and transmute into the visible as an effect of the imbalance. Visible effects can include anxiety, depression, suicidal thoughts, PTSD, Bi Polar, ADD, ADHD, stress, fear, anger, guilt, sexual problems and self-punishment to name a few. Holographic Kinetics aims assist a patient in accessing the causes of these imbalances, so they are able to bring those imbalances back into balance to remain in a state of homeostasis permanently once they have been addressed properly.
Holographic Kinetics uses the natural law of causality in action-and-reaction sequences [16]. Causality is commonly defined as the relationship between causes and effects [17,18]. It is considered to be fundamental to all natural science, especially physics, philosophy, statistics and modern experimental psychology [16]. Based on Minkowski spacetime scientific work, causality means that an effect can occur from a cause which is in the back (past) light cone of an event.
Similarly, a cause can have an effect outside its front (future) light cone [19,22]. The action-reaction pendulum of cause and effect feeds an invisible dimension within the internal world of a humans energy field, creating a visible imbalance (anxiety, depression, etc.,) which needs to be brought back to null point zero vector observer within man’s awareness by waking up to his responsibility of the metaphysical consequences of his own creation upon its own separate dimension of time [21,22]. Only then, will man’s own imbalances be brought back to balance and the effect (mental illness) will finally cease to exist [15].
Kinetic energy is a free-flowing, constant energy, inside and around us, until captured by thoughts. Holographic Kinetics is not limited to this physical dimension, but has an awareness of multi-dimensions and sees man as a multi-dimensional being in a multi-dimensional world, consisting of multiple parts of the human form, in multiple dimensions that need to be cleared. This includes the Spirit and the Soul. Under “Royal commission in the bringing them home report” it states;
- Bad health is not being connected to your Spiritual being, this indicates those important parts of your life are not connected, being damaged by different forces not of our control or doing.
- An aboriginal perception of Mental health is holistic; there is no need to compartmentalize…..Aboriginal mental health should not be viewed from a medical model of abnormality
- Aboriginal culture sees the health of the mind, the body, and the spirit as inextricable linked
- Witnesses to the inquiry emphasized the fact that disturbed people are often perceived as a normal reaction to Spiritual forces or a curse, such as being ‘Sung’, Rather than being physical ill, the person is considered to be spiritually ill
One of the fundamental aspect of a hologram is any part of the hologram contains the whole in the form of fractals of stored information. Consequently, a piece of a long-term memory is equally distributed over a dendritic arbor so that each part of the dendritic network contains all the information stored over the entire network of the genetic hereditary lines of the mother and father or beyond (epigenetics) and/or long term experience memories attached to the life force of the patient, coming through time [23-31].
A well trained and experienced Holographic Kinetic practitioner can assist the life force of the patient in accessing internal hyperspace within the patient, where all things become omnipresent, omnipotent and omniscient within their own separate dimension of reality. In Aboriginal culture this is known as the Spirit. (the internal life form, the spark of life) Different to the Psych or Soul, (the external experience) stored as memory, within the cells. Therefore, the practitioner can successfully assist the client to access and clear, their created reality by correcting in invisible the original cause of the visible effect, that is affecting the patient at themoment, within its own dimension of time, of the treatment. The difference between the other treatments and this modality is the permanent improvement and positive outcomes you achieve as a practitioner for the patient [15]. A Holographic Kinetics practitioner recognizes and addresses successfully the multi-dimensions of man.
You must deal with changing the self-destructive processes, these inner patterns that erode the self and mental well-being [34,35].
CASE STUDY: A MILITARY VETERAN CLINICALLY DIAGNOSED WITH SUICIDE, DEPRESSION AND PTSD
The initial patient for this study joined the army at the age of 18 and was deployed only 6 months after to Iraq towards the end of 2003. He stayed there in active duty for 27 months and upon his return was clinically diagnosed with PTSD, depression and suicidal thoughts. As previously mentioned, he tried all allopathic and holistic healing modalities available such as (among others):
Cognitive therapy: For suicidal people this was developed by Aaron Beck and Gregory Brown. Unlike other CBT treatments, this approach is not time limited. The third and last stage is “relapse prevention with a Twist”, which involves inducing a suicidal crisis for the client while they are in session. The theory behind this technique draws from the fact that people who are suicidal have trouble using newly acquired skills when in crisis. By evoking the crisis in session, the client is able to apply and test coping skills with the therapist’s help and support. Clients do not graduate from treatment until they demonstrate that they are ready to do this on their own.
Dialectical behavior therapy: Developed by Marsha M Linehan, is designed to treat emotion regulation difficulties and suicidal behavior. One element, the skill-building component of DBT, addresses the issues of distress tolerance and the development of healthy affect regulation strategies, both of which are essential for suicidal clients.
Mentalizing treatment: Developed by Jon Allen and Peter Fonagy, emphasizes emotional regulation and expressiveness. The techniques implemented assist clients in forming good affect regulation and tolerance through the process of developing the mentalizing capability to observe and understand their minds and the minds of others, accurately seeing the mind behind the behavior.
Transference-focused therapy: Developed by Kernberg, Clarkin and Yeomans, concentrates on the intermediate interaction between the client and therapist in session by focusing on the therapeutic relationship.
Voice therapy: Developed by Robert Firestone, is a cognitive-affective-behavioral therapeutic methodology that brings introjected hostile thoughts, with the accompanying negative affect, to consciousness, rendering them accessible for treatment?
Eye Movement Desensitization and Reprocessing (EMDR): A psychotherapy treatment that was originally designed to alleviate the distress associated with traumatic memories. Shapiro’s adaptive information processing model posits that EMDR therapy facilitates the accessing and processing of traumatic memories and other adverse life experience to bring these to an adaptive resolution.
Emotional Freedom Technique (EFT): An alternative therapy for fear, Thought Field Therapy (TFT), was developed by Roger Callahan. TFT is based on Traditional Chinese Medicine, claiming to access alleged meridians that carry the energy and well-being of animals, including humans. Callahan developed TFT while treating a patient for water phobia. The Emotional Freedom Technique (EFT), developed by Gary Craig, evolved from TFT. Craig claims that EFT takes TFT a step further by using a comprehensive procedure, thus eliminating the need for a complicated diagnosis.
Since none of these therapies helped, he opted for medications, which he decided to stop in 2012. He came to the conclusion that the drugs were more detrimental to his health than they were positive. Since then, he has been “managing” his illnesses by himself by struggling daily to stay alive and using all of his willpower to not commit suicide. On September 7th, 2017, he received a 90-minute Holographic Kinetics session. Three days after, he reported more than 50% improvement towards his suicidal and depression symptoms and a less than 50% improvement regarding his PTSD symptoms. Three weeks after the HK session, he became 100% free from all of his prior symptoms. Today, November 21st, 2017, he is still symptom free. The Holographic Kinetics protocol for treating suicidal patients is easily replicable once you have become an advanced and experienced HK practitioner. For military veterans, it is more complicated than normal and it requires advanced professional Holographic Kinetics.
The patient, before and after treatment (4 days after, 4 weeks after and almost 5 months after), answered these Holographic Kinetics questions:
Before a session;
I would remove as most is auto suggestion and dangerous and could have a worst effect on the patient.
Cognitive therapy: For suicidal people this was developed by Aaron Beck and Gregory Brown. Unlike other CBT treatments, this approach is not time limited. The third and last stage is “relapse prevention with a Twist”, which involves inducing a suicidal crisis for the client while they are in session. The theory behind this technique draws from the fact that people who are suicidal have trouble using newly acquired skills when in crisis. By evoking the crisis in session, the client is able to apply and test coping skills with the therapist’s help and support. Clients do not graduate from treatment until they demonstrate that they are ready to do this on their own.
Dialectical behavior therapy: Developed by Marsha M Linehan, is designed to treat emotion regulation difficulties and suicidal behavior. One element, the skill-building component of DBT, addresses the issues of distress tolerance and the development of healthy affect regulation strategies, both of which are essential for suicidal clients.
Mentalizing treatment: Developed by Jon Allen and Peter Fonagy, emphasizes emotional regulation and expressiveness. The techniques implemented assist clients in forming good affect regulation and tolerance through the process of developing the mentalizing capability to observe and understand their minds and the minds of others, accurately seeing the mind behind the behavior.
Transference-focused therapy: Developed by Kernberg, Clarkin and Yeomans, concentrates on the intermediate interaction between the client and therapist in session by focusing on the therapeutic relationship.
Voice therapy: Developed by Robert Firestone, is a cognitive-affective-behavioral therapeutic methodology that brings introjected hostile thoughts, with the accompanying negative affect, to consciousness, rendering them accessible for treatment?
Eye Movement Desensitization and Reprocessing (EMDR): A psychotherapy treatment that was originally designed to alleviate the distress associated with traumatic memories. Shapiro’s adaptive information processing model posits that EMDR therapy facilitates the accessing and processing of traumatic memories and other adverse life experience to bring these to an adaptive resolution.
Emotional Freedom Technique (EFT): An alternative therapy for fear, Thought Field Therapy (TFT), was developed by Roger Callahan. TFT is based on Traditional Chinese Medicine, claiming to access alleged meridians that carry the energy and well-being of animals, including humans. Callahan developed TFT while treating a patient for water phobia. The Emotional Freedom Technique (EFT), developed by Gary Craig, evolved from TFT. Craig claims that EFT takes TFT a step further by using a comprehensive procedure, thus eliminating the need for a complicated diagnosis.
Since none of these therapies helped, he opted for medications, which he decided to stop in 2012. He came to the conclusion that the drugs were more detrimental to his health than they were positive. Since then, he has been “managing” his illnesses by himself by struggling daily to stay alive and using all of his willpower to not commit suicide. On September 7th, 2017, he received a 90-minute Holographic Kinetics session. Three days after, he reported more than 50% improvement towards his suicidal and depression symptoms and a less than 50% improvement regarding his PTSD symptoms. Three weeks after the HK session, he became 100% free from all of his prior symptoms. Today, November 21st, 2017, he is still symptom free. The Holographic Kinetics protocol for treating suicidal patients is easily replicable once you have become an advanced and experienced HK practitioner. For military veterans, it is more complicated than normal and it requires advanced professional Holographic Kinetics.
The patient, before and after treatment (4 days after, 4 weeks after and almost 5 months after), answered these Holographic Kinetics questions:
Before a session;
- What is affecting you that you would like to look at?
- If you looked over your life what are the cycles that you see that are affecting you?
- What do you react to?
- Have you taken any drugs or drink excessively?
- What is the main issue that you would like to clear?
- Have you been in a war zone?
- Do you have voices in the head?
- Do you still have voices in the head?
- How do you feel since the session?
- Are you still on drugs or alcohol?
- How did the family find your attitude, before the session?
- What does your family find your attitude since the session?
- Is there anything else that is affecting you that you would like to look at?
I would remove as most is auto suggestion and dangerous and could have a worst effect on the patient.
DISCUSSION FOR FUTURE RESEARCH: METHODS OF SCIENTIFICALLY ASSESSING MENTAL ILLNESSES
Over a period of 7 years, 206,000 veterans who entered the VA health care system were assessed. 14% were diagnosed with depression. Even with this high number, depression is under-diagnosed in the veteran population [36]. Veterans with depression can be screened using the Beck Depression Inventory, (which is also mentioned below) or Patient Health Questionnaire-2 and Patient Health Questionnaire-9, which are both widely popular [6]. In this study, the researchers took care to measure all the other symptoms the veterans were experiencing, including but not limited to PTSD or comorbid alcohol use disorder. Thus, after treatment was over, it was more clear what symptoms were treated in the veterans because the researchers had multiple facets of information on the veterans mental health status [36]. This means there is a reliable system in place to diagnose and measure depression. However, “data shows that within the first year following a mental health diagnosis, two-thirds of patients receive very minimal or no psychiatric care” [36]. They are left to wallow in depression with no treatment, which can develop alongside other symptoms that may lead to suicide.
Depression also presents itself with suicidal behavior. Suicidal behavior is hard to measure in veterans because it often presents with other symptoms, such as psychological pain. A study found a “significant linear correlation between psychological pain and suicidal tendencies in the depressed patient cohort” [37]. The researchers applied these findings to a “diagnostically heterogeneous” population of 57 US veterans that were currently enrolled in a suicide prevention program. First, they used the Mee-Bunney Psychological Pain Assessment Scale. This is a 10-item self-rating inventory, where psychological pain is measured from none to unbearable and frequency is also measured [38]. The researchers also administered the Columbia Suicide Severity Rating Scale, the Beck Depression Inventory, the Beck Hopelessness Scale, and the Barratt Impulsiveness Scale. The researchers utilized multiple tests to determine which factors most affected the patient’s suicidal ideations. The results determined that impulsiveness and psychological pain accounted for the most shared variance of suicidal ideation in the 57 veterans that were tested before and after their enrollment in the suicide prevention program [37]. Again, the traditional view of medicine cannot effectively treat suicide as a holistic issue, which is why alternative treatments must be prioritized for treatment. With 22 veterans committing suicide every day, alternative models of treatment must be developed to mitigate this crisis for the people who serve our country.
Depression also presents itself with suicidal behavior. Suicidal behavior is hard to measure in veterans because it often presents with other symptoms, such as psychological pain. A study found a “significant linear correlation between psychological pain and suicidal tendencies in the depressed patient cohort” [37]. The researchers applied these findings to a “diagnostically heterogeneous” population of 57 US veterans that were currently enrolled in a suicide prevention program. First, they used the Mee-Bunney Psychological Pain Assessment Scale. This is a 10-item self-rating inventory, where psychological pain is measured from none to unbearable and frequency is also measured [38]. The researchers also administered the Columbia Suicide Severity Rating Scale, the Beck Depression Inventory, the Beck Hopelessness Scale, and the Barratt Impulsiveness Scale. The researchers utilized multiple tests to determine which factors most affected the patient’s suicidal ideations. The results determined that impulsiveness and psychological pain accounted for the most shared variance of suicidal ideation in the 57 veterans that were tested before and after their enrollment in the suicide prevention program [37]. Again, the traditional view of medicine cannot effectively treat suicide as a holistic issue, which is why alternative treatments must be prioritized for treatment. With 22 veterans committing suicide every day, alternative models of treatment must be developed to mitigate this crisis for the people who serve our country.
WHY THIS RESEARCH IS IMPORTANT?
Veterans are receiving ineffective mental treatment. For example, “a study of suicide among older male veterans in the general population and retrospective studies of veterans from previous conflicts failed to identify general increases in risk” [7]. Veterans often have multiple mental health afflictions, thus when measuring what kind of symptoms a veteran has; clinicians must administer multiple types of tests. Among 110,603 veterans who had depression, 92% of women and 91% of men had “depression along with other psychiatric comorbidities” [5]. Thus, it is important to test for multiple symptoms when evaluating a veteran to fully measure the psychological pain they are experiencing so that we can know how to give them the best assessment possible. Nevertheless, evaluating veterans is only part of the battle for better mental health.
PROPOSED METHOD OF ASSESSING SCIENTIFICALLY BEFORE AND AFTER HK TREATMENTS: NON INVASIVE FUNCTIONAL MRI AND/OR SPECT IMAGING
Functional MRI (fMRI) is a unique type of MRI that can image both brain structure and function. fMRI uses blood flow to measure increases in neuronal activity, called Blood Oxygen Level Dependent (BOLD) Imaging. BOLD can also be combined with Arterial Spin Labeling (ASL), Magnetic Resonance Spectroscopy (MRS), and Diffusion Tensor Imaging (DTI) with Fractional Anisotropy (FA), to determine additional functions of the brain related to blood flow, neural metabolite ratios and fiber tract integrity [39,41].
FMRI is largely used in research, but is beginning to make an appearance in outpatient clinical medicine. Therefore, fMRI may be possible in assisting physicians and researchers in helping in the diagnosis of many mental disorders such as anxiety, PTSD, depression, suicide and dementia, and more. FMRI may also be useful in detecting changes before and after various treatments to determine the changes in brain function and possible facilitation of treatment efficacy [41,42].
By evaluating neural networks, cerebral blood perfusion, neural metabolites and quantified integrity of fiber tracts in the brain, fMRI may provide insight into the visualization of mental illness and ultimately advancing the diagnostic capabilities of the brain and various treatments far beyond what is currently available [40,42,43].
For example, the patient Arterial Spin Labeling (ASL) measures blood perfusion in the brain. The frontal lobes, as indicated by the arrows in the picture, show an increase in brightness before and after, which is consistent with increased and normalized blood perfusion to the frontal lobe. These areas based on literature have been shown to play a major role in depression type of conditions and feelings. Increased blood flow to this region may indicate possible remission from depression related symptoms (Figure 1).
FMRI is largely used in research, but is beginning to make an appearance in outpatient clinical medicine. Therefore, fMRI may be possible in assisting physicians and researchers in helping in the diagnosis of many mental disorders such as anxiety, PTSD, depression, suicide and dementia, and more. FMRI may also be useful in detecting changes before and after various treatments to determine the changes in brain function and possible facilitation of treatment efficacy [41,42].
By evaluating neural networks, cerebral blood perfusion, neural metabolites and quantified integrity of fiber tracts in the brain, fMRI may provide insight into the visualization of mental illness and ultimately advancing the diagnostic capabilities of the brain and various treatments far beyond what is currently available [40,42,43].
For example, the patient Arterial Spin Labeling (ASL) measures blood perfusion in the brain. The frontal lobes, as indicated by the arrows in the picture, show an increase in brightness before and after, which is consistent with increased and normalized blood perfusion to the frontal lobe. These areas based on literature have been shown to play a major role in depression type of conditions and feelings. Increased blood flow to this region may indicate possible remission from depression related symptoms (Figure 1).
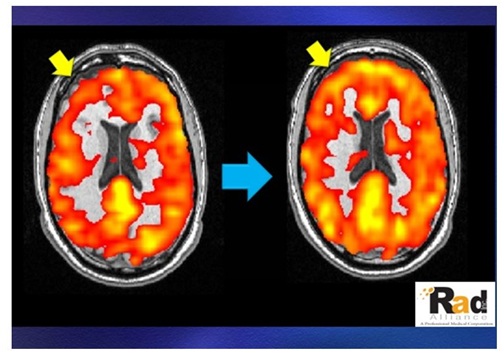 Figure 1: Arterial Spin Labeling (ASL) of the patient before and 4 weeks after the Holographic Kinetic session.
Figure 1: Arterial Spin Labeling (ASL) of the patient before and 4 weeks after the Holographic Kinetic session.The Blood Oxygen Level Dependent (BOLD) imaging measures the connectivity of the brain by evaluating which areas are working together, and the strength of that connectivity. The brightness and surface area of the activation on the left image in the frontal lobes may be consistent with over-rumination or uncontrolled thoughts or actions. The picture on the right has a reduction in both brightness and surface area in the frontal lobes, again consistent with the brain areas similar to that in the ASL findings (Figure 2). This reduction in activity may indicate a possible remission of symptoms pertaining to rumination and uncontrolled thoughts.
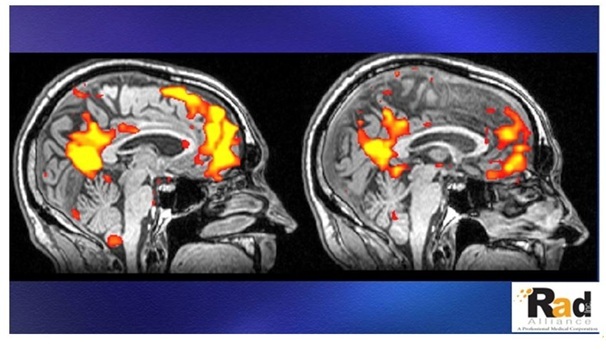
Figure 2: The Blood Oxygen Level Dependent (BOLD) of the patient before and 4 weeks after the Holographic Kinetics treatment.
SPECT Imaging could also be used. SPECT stands for single photon emission computed tomography. It is a nuclear medicine procedure that is widely used to study heart, liver, thyroid, bone and brain problems. Brain SPECT imaging gives you and your doctor information on the blood flow and activity patterns of your brain. Brain SPECT imaging is a proven and reliable measure of brain blood flow and activity; therefore, it is used as a tool in the evaluation and treatment process at Amen Clinics. SPECT imaging effectively shows us the patterns of activity in your brain. It allows our physicians to observe three things: areas of the brain that work well; areas of the brain that work too hard; and areas of the brain that don’t work hard enough. Science has repeatedly recognized the value of brain SPECT imaging for assessing brain function. There is a robust amount of scientific data that support the utility of SPECT for revealing the blood flow patterns underlying many different types of brain problems. Dr Daniel Amen has authored or co-authored more than 70 peer-reviewed published research studies on brain SPECT imaging. In addition, our website has a collection of more than 2,700 abstracts on brain SPECT from researchers around the world [44].
CONCLUSION
Per the White House Office of Management and Budget regarding Veterans Affairs, $7.4 billion dollars was spent on mental health services for veterans in 2017 and $133 million for suicide [45,46]. The description of the services provided does not mention any kind of preventative or holistic treatment. Although pharmaceuticals can cure ailments, when dealing with the complexities of mental health, alternative medical treatments can make a larger impact. The current model of medicine is inaccessible and ineffective for the multitude of mental health issues those veterans face, which is why alternative medical treatments should be utilized. More and more money is being thrown at issues faced by veterans with little to no overall improvement. Employing alternative medical treatments, such as Holographic Kinetics, as most depression can be cleared in a few sessions, with Holographic Kinetics, this, simply could give more options that are desperately needed to treat veterans affected by PTSD, depression and suicidal ideations. Further research is needed to scientifically measure the efficacy and effectiveness of this non invasive holistic mental health modality on a larger scale [47].
REFERENCES
- Ramchand R (2017) Epidemiologist RAND Corporation: Congressional testimony before the senate appropriations committee preventing veterans suicides. Epidemiologist RAND Corporation, California, USA.
- S. Department of Veterans Affairs (2016) Suicide among veterans and other Americans Office of Suicide Prevention. US Department of Veterans Affairs, Washington, USA.
- US Department of Veteran Affairs (2016) VA Conducts Nation’s Largest Analysis of Veteran Suicide. Office of Public and Intergovernmental Affairs, US Department of Veteran Affairs, USA.
- https://www.militarytimes.com/veterans/2016/07/07/new-va-study-finds-20-veterans-commit-suicide-each-day/
- Lam CA, Sherbourne C, Gelberg L, Lee ML, Huynh AK, et al. (2017) Differences in depression care for men and women among veterans with and without psychiatric comorbidities. Womens Health Issues 27: 206-213.
- Arroll B, Goodyear-Smith F, Crengle S, Gunn J, Kerse N, et al. (2010) Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med 8: 348-353.
- Bossarte RM, Knox KL, Piegari R, Altieri J, Kemp J, et al. (2012) Prevalence and characteristics of suicide ideation and attempts among active military and veteran participants in a national health survey. Am J Public Health 102: 38-40.
- https://www.va.gov/budget/docs/summary/fy2018VAbudgetInBrief.pdf
- National Alliance on Mental Illness (2017) Depression and veterans. National Alliance on Mental Illness, Virginia, USA.
- Department of Veterans Affairs (2016) Facts about veteran suicide. Department of Veterans Affairs, USA.
- http://www.ptsd.ne.gov/what-is-ptsd.html
- https://www.ptsd.va.gov/PTSD/public/assessment/ptsd-measured.asp
- Steel JL, Dunlavy AC, Stillman J, Pape HC (2011) Measuring depression and PTSD after trauma: Common scales and checklists. Injury 42: 288-300.
- https://www.ptsd.va.gov/public/treatment/therapy-med/treatment-ptsd.asp
- Chevalier A, Richards S (2017) Holographic kinetics for a child suffering from autism with extreme aggressive behavioral disorder. J Altern Complement Integr Med 3: 1-4.
- Schlottmann A, Ray ED, Surian L (2012) Emerging perception of causality in action-and-reaction sequences from 4 to 6 months of age: Is it domain-specific? J Exp Child Psychol 112: 208-230.
- Green C (2003) The Lost Cause: Causation and the Mind-Body Problem. Oxford Forum, Oxford, UK.
- Bunge M (1959) Causality: the place of the causal principle in modern science. Harvard University Press, Cambridge, Massachusetts, USA.
- Galison PL (1979) Minkowski’s Space-Time: From Visual Thinking to the Absolute World. University of California Press, Berkeley, California, USA.
- Walter SA (1999) Minkowski, mathematicians and the mathematical theory of relativity. In: Goenner, H, Renn J, Ritter J, Sauer T (eds.). The Expanding Worlds of General Relativity. Birkhäuser 45-86.
- Penrose R (2005) Minkowskian geometry. In: Penrose R (ed.). Road to Reality: A Complete Guide to the Laws of the Universe. Jonathan Cape, London, UK.
- Weinberg S (2013) The Quantum Theory of Fields. Cambridge University Press, England, UK.
- Forsdyke DR (2009) Samuel Butler and human long term memory: Is the cupboard bare? J Theor Biol 258: 156-164.
- Andrew AM (1997) The decade of the brain ? further thoughts. Kybernetes 26: 255-264.
- Pribram KH, Meade SD (1999) Conscious awareness: Processing in the synaptodendritic web. New Ideas in Psychology 17: 205-204.
- Pribram KH (1999) Quantum holography: Is it relevant to brain function? Information Sciences 115: 97-102.
- Vandervert LR (1995) Chaos theory and the evolution of consciousness and mind: A thermodynamic-holographic resolution to the mind-body problem. New Ideas in Psychology 13: 107-127.
- Berger DH, Pribram KH (1992) The relationship between the Gabor elementary function and a stochastic model of the inter-spike interval distribution in the responses of visual cortex neurons. Biol Cybern 67: 191-194.
- Pribram KH (2004) Consciousness Reassessed. Mind and Matter 2: 7-35.
- Gabor D (1972) Holography, 1948--1971. Science 177: 299-313.
- Borsellino A, Poggio T (1972) Holographic aspects of temporal memory and optomotor responses. Kybernetik 10: 58-60.
- Bókkon I (2005) Dreams and neuroholography: An interdisciplinary interpretation of development of homeotherm state in evolution. Sleep and Hypnosis 7: 61-76.
- Gabor D (1968) Holographic Model of Temporal Recall. Nature 217: 584.
- Mikulincer M Orbach I (1995) Attachment styles and repressive defensiveness: The accessibility and architecture of affective memories. J Pers Soc Psychol 68: 917-925.
- Apter A, Gothelf D, Orbach I, Weizman R, Ratzoni G, et al. (1995) Correlation of suicidal and violent behavior in different diagnostic categories in hospitalized adolescent patients. J Am Acad Child Adolesc Psychiatry 34: 912-918.
- Waltz TJ, Campbell DG, Kirchner JE, Lombardero A, Bolkan C, et al. (2014) Veterans with depression in primary care: provider preferences, matching, and care satisfaction. Fam Syst Health 32: 367-377.
- Reist C, Mee S, Fujimoto K, Rajani V, Bunney WE, et al. (2017) Assessment of psychological pain in suicidal veterans. PLoS One 12: 0177974.
- Tossani E (2013) The concept of mental pain. Psychother Psychosom 82: 67-73.
- Yi L, Wang J, Jia L, Zhao Z, Lu J, et al. (2012) Structural and Functional Changes in Subcortical Vascular Mild Cognitive Impairment: A Combined Voxel-Based Morphometry and Resting-State FMRI Study. PLoS One 7: 44758.
- Bellace M, Williams JM, Mohamed FB, Faro SH (2013) “An FMRI Study of the Activation of the Hippocampus by Emotional Memory. Int J Neurosci 123: 121-127.
- Fox M, Pascual-Leone A (2012) Intrinsic Functional Connectivity with the Subgenual Cingulate Predicts Clinical Efficacy of TMS Targets for Depression (P01.188). Neurology 78.
- Chiaravalloti ND (2014) Application of Functional Neuroimaging to Evaluating the Efficacy of Cognitive Rehabilitation in Neurological Populations. Imaging in Medicine 6: 9-11.
- Fayed N, Andrés E, Viguera L, Modrego PJ, Garcia-Campayo J (2014) Higher glutamate+glutamine and reduction of N-acetylaspartate in posterior cingulate according to age range in patients with cognitive impairment and/or pain. Acad Radiol 21: 1211-217.
- Amen DG, Prunella JR, Fallon JH, Amen B, Hanks C (2009) A comparative analysis of completed suicide using high resolution brain SPECT imaging. J Neuropsychiatry Clin Neurosci 21: 430-439.
- https://www.whitehouse.gov/sites/whitehouse.gov/files/omb/budget/fy2018/budget.pdf
- Reistad B (2015) New bill provides VA accountability. The American Legion, Indianapolis, Indiana, USA.
- Amen DG, Trujillo M, Newborn A, Willeumier K, Tarzwell R, et al. (2011) Brain SPECT Imaging in Complex Psychiatric Cases: An Evidence-Based, Underutilized Tool. Open Neuroimag J 5: 40-48.
Citation: Chevalier A, Richards S (2017) Holographic Kinetics for Clinically Diagnosed Suicidal, Depressed, PTSD Military Veterans: Case Study. J Altern Complement Integr Med 3: 044.
Copyright: © 2017 Antoine Chevalier, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!