Homoeopathic Management of Severe Haemophilia in Pediatric age group: Twin Case Study
*Corresponding Author(s):
Kundu TapasPI-Homoeopathy In Haemophilia, Homeopathic Medical College And Hospital, Nashik, Maharashtra, India
Tel:+91 9373908112,
Email:drkundu2002@gmail.com
Abstract
Haemophilia being a rare disorder its management is costly. In pediatric age group haemophiliacs giving factor infusion during the bleeding phase is a tedious job as there is lack of cooperation along with fear of injection in the patients. As the patient are in growing phase they are prone to multiple injuries and giving factor infusions multiple times may cause development of inhibitors. In this case study both the patient started with homoeopathic treatment in early age which proved to be helpful as many of their bleeding episodes were managed with homoeopathic medicines alone. Out of those 2 patients, 1 patient did not require any factor infusion and the other one required factor concentrate in five episode of bleeding whereas all other acute emergencies were managed with homoeopathic medicines. Both the patients were relieved of their other complaints with homoeopathy.
Keywords
Acute bleeds; Blood Non-coagulable; Haemophilia; Homoeopathy; Pediatric
Introduction
Haemophilia is an X-linked [1] inherited immunogenetic [2] rare bleeding disorder resulting from deficiency of clotting Factor VIII (Haemophilia A) or Factor IX (Haemophilia B). Haemophilia is a high cost disease. Clotting products constitute more than 90 percent of the total cost of haemophilia care. In Resource limited nations (RLN) very little amount is spent on health issues [3]. In Modern medicine, though the Factor concentrates are available for free at Government Hospitals still patients find it difficult to avail because of time constraint & immobility of patients during acute bleeds. Additionally if the frequency of factor infusions are more it can cause development of inhibitors [4,5]. Homoeopathy has proved to be helpful in haemophilic patients as it probably creates a bypass for the normal clotting mechanism & thereby the bleeding stops. Homoeopathic medicines when given on symptom totality have always given results. In India where the availability of factor is a major issue, Homoeopathy has proved out to be a boon for haemophiliacs as an add-on therapy & / complementary therapy.
Methods and Materials
In this case study, two cases / patients of pediatric age group from Homoeopathy In Haemophilia (HIH), Mumbai Centre located at Haemophilia Society, Parel, Mumbai are presented which shows how the acute emergencies of bleeds were managed with Homoeopathic medicines. Case Report Format [6] of HIH Protocol is followed. Various Scales are used for assessment such as Wong Baker faces Pain rating scale [7], Adaptive Maladaptive Behavioral scale [8]. HIH treatment protocol is followed- Step 1- Managing with Hammamelis virginiana Q (Mother tincture). Step 2- Acute medicine is given considering patients reaction during bleeding episodes (change in behavior), Pain score & type of injury. Step 3- Constitutional medicine is given considering the Genetic history, Miasmatic trait, Frequency of bleeds, Affection of joints etc. The patients are given Hammamelis Q (Mother Tincture) & Emergency Kit of Homoeopathic Thrombostatic medicines. Homoeopathic software RADAR-10.5 [9] was used for Repertorization. Consent was taken from both the patient’s Parent / Guardian. Patient’s parent were asked to maintain a bleeding diary which gave the details of the number of bleeding episodes in a month, type of injuries, how were the episodes managed, behavior of the patient during acute bleeds as well as during non-bleeding phase& also complaints other than Haemophilia.
Cases
Case No- 1 (HIH Mumbai Centre-343)
History of the patient: A 7 month old baby boy diagnosed as haemophilia A severe (Factor VIII-<1%) was brought by his parents with complaint of recurrent bruises. Bruise-Mostly intramuscular bruises-on abdomen, left iliac region, on legs, bluish to blackish in color, hard to touch, 5-6 bruises in 15 days. He also had recurrent episodes of cold and coryza with cough. Patient was infused factor for the first time at the age of 6 months which resulted in severe thrombophlebitis, post infusion.
Family History - Maternal Grandmother’s Sister Son- Haemophilia (Type not known). On detailed case taking during follow ups and (checking the bleeding diary), parent revealed that the patient- Physical Generals- Desires - sweets. Perspiration is profuse esp. over nape of neck at night. Bowel habit was regular. Thirst & Appetite - adequate. Sleep - sound. Thermal - Chilly patient. Mental Generals-Restlessness with desire to roam outside the house. Construct - Constitution is lean & thin.
Assessment with scales:
- Pain score during bleed-8-10.
- Adaptive and Maladaptive Behavior scales-
- Activity level: Very active- score-6
- Cooperation: Cooperative- score-6
- Communication skills: shy but warms up quickly- score-4
3. Joint affection-no joint bleeds, mobility normal.
Miasmatic trait [10]- Tubercular Miasm- changing symptoms, restlessness, haemorrhagic diathesis, tendency of recurrent respiratory infections, constitution is thin & lean.
First Prescription was – Phosphorus [11] 30 C/3Doses/24 hourly & PL 30 C/1 dram, 2 pills twice per day.
After regular follow ups & treatment - the frequency of bruises reduced to 1-2 in 15 days. Also the tendency of recurrent cold coryza with cough had reduced. Patient had many episodes of acute bleedings which were managed (at HIH Mumbai Centre & sos Tele-consultation) only with Homoeopathic medicines & Hammamelis Q along with RICE method. Now the Patient is 6 years old plus & has not required any Factor VIII Infusion from the time he is on Homoeopathic medicines (i.e. since the age of 7 months till 6 years of age) (Figure 1 & Table 1).
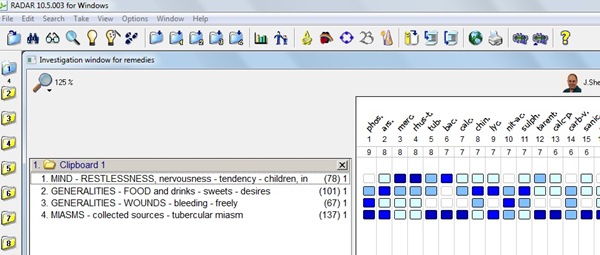 Figure 1: Repertorisation chart.
Figure 1: Repertorisation chart.
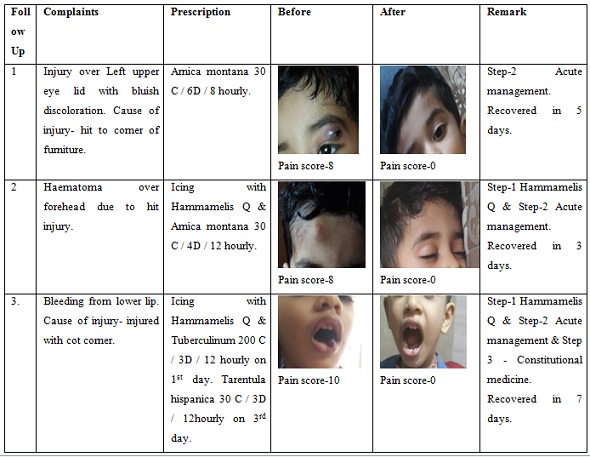 Table 1: Few of the Acute Bleeds & its management.
Table 1: Few of the Acute Bleeds & its management.
Discussion of bleeding episodes
Episode-1- Patient had injury over Left upper eye lid with bluish discoloration and was not allowing touching or examining. Cause of injury- hit to corner of furniture. Pain score was 8. Prescribed - Arnica montana 30 C / 6 Doses / 8 hourly. Pain score was 0 later. The patient recovered completely in 5 days.
Episode-2- Patient had Haematoma over forehead due to hit injury. Pain score was 8. Prescribed - Icing with Hammamelis Q & Arnica montana 30 C / 4 Doses / 12 hourly. Pain score was 0 later. The patient recovered completely in 3 days.
Episode-3- Patient had acute bleeding-bright red blood from lower lip. Cause of injury- injured with cot corner. Pain score was 10. Prescribed - Icing with Hammamelis Q which helped in stopping the bleeding but bleeding would start again on slightest touch & So Tuberculinum [12] 200 C / 3 Doses / 12 hourly was given on 1st day. The bleeding did not stop completely, clot was forming but the patient was touching the clot with tongue & thereby it would start bleeding again. So the Constitutional medicine (derived from regular follow ups of patient) - Tarentula hispanica 30 C / 3 Doses / 12hourly was given on 3rd day which helped to heal completely. Pain score was 0 later. The patient recovered completely in 7 days (Table 2).
|
|
Scale Used |
Episode 1 |
Episode 2 |
Episode 3 |
|||
|
|
|
Before |
After |
Before |
After |
Before |
After |
|
1 |
Adaptive / maladaptive (modified) behavioral scale- |
|
|
|
|
|
|
|
|
Activity level- score |
2 |
6 |
4 |
8 |
2 |
6 |
|
|
Co-operation- score |
4 |
8 |
4 |
8 |
0 |
6 |
|
|
Communication Skill- score |
4 |
6 |
6 |
8 |
2 |
6 |
|
2 |
Wong baker pain rating scale |
8 |
0 |
8 |
0 |
10 |
0 |
Table 2: Assessment of Scale.
Case No-2 (HIH Mumbai Centre-361)
History of the patient: A 1year old male patient with haemophilia A severe (Factor VIII-- <1%) was brought by his parent with complaint of recurrent bruises. Bruise - intramuscular, over hands, legs and abdomen, hard to touch, bluish in color, 7-8 in a month. Eczematous patch on both legs below knee, both hands below elbow. Eruption-red with itching, < Night, dryness. Recurrent episodes of cold, coryza and cough.
Family History- Maternal Grandfather & Maternal Grandfather’s Brother-Haemophilia a Severe. On detailed case taking during follow ups and (checking the bleeding diary), parent revealed that the patient Physical Generals– Desires - sweets. Sleep - sound. Urine - NAD. Bowels -constipated. Thermals - Hot patient. Mental Generals- Restless cannot keep still, Activity desires, Likes Music & Dancing. Bangs head in anger. Construct - Constitution is lean & thin.
Assessment with scales
- Pain score during bleed -10
- Adaptive and Maladaptive Behaviour scales
- Activity level: Very active- score-6
- Cooperation: Mild Cooperative- score-4
- Communication skills: shy but warms up slowly- score-2
- Joint affection-no joint bleeds, mobility normal
Miasmatic trait - Tubercular Miasm- restlessness, hemorrhagic diathesis, tendency of recurrent respiratory infections, skin infection, constitution is thin & lean.
First Prescription was - Tarentula hispanica 200 C / 3 Doses / 24 hourly & PL 30 C / 2 dram, 2 pills three times per day.
After regular follow ups & treatment - the frequency of bruises reduced markedly. Frequency of episodes of cold, coryza & cough had reduced. Itching over eczema patch area reduced. His restlessness reduced &he stopped banging head in anger. Now the patient is 5 years old & required factor infusion five times in between from the time he is on homoeopathic medicines (i.e. since the age of 1 year till 5 years of age) (Figure 2 & Table 3).
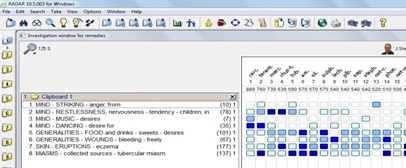 Figure 2: Repertorisation chart.
Figure 2: Repertorisation chart.
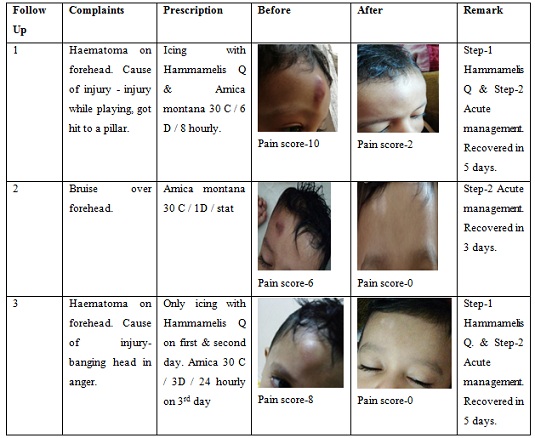 Table 3: Few of the Acute Bleeds & its management.
Table 3: Few of the Acute Bleeds & its management.
Discussion of Bleeding Episodes
Episode-1- Patient had haematoma on forehead with reddish, bluish discoloration. Cause of injury- injury while playing, got hit to a pillar. Patient was crying with pain. Pain score was10 Prescribed- Icing with Hammamelis Q & Arnica montana 30 C / 6 Doses / 8 hourly. Pain score was 2 later. The patient recovered completely in 5 days.
Episode-2- Patient had bruise over forehead. Pain score was 6. Prescribed- Arnica montana 30/1Dose/stat. Pain score was 0 later. The patient recovered completely in 3 days.
Episode-3- Patient had haematoma on forehead. Cause of injury- banging head in anger. Pain score was 8. Prescribed- Only icing with Hammamelis Q on first & second day-as it was an acute bleed/haematoma. Arnica montana 30 C / 3 Doses / 24 hourly on 3rd day after the haematoma reduced and bluish discoloration was seen. Pain score was 0 later. The patient recovered completely in 5 days (Table 4).
|
|
Scale Used |
Episode 1 |
Episode 2 |
Episode 3 |
|||
|
|
|
Before |
After |
Before |
After |
Before |
After |
|
1 |
Adaptive / maladaptive (modified) behavioral scale- |
|
|
|
|
|
|
|
|
Activity level- score |
2 |
8 |
4 |
6 |
4 |
8 |
|
|
Co-operation- score |
2 |
8 |
6 |
8 |
4 |
8 |
|
|
Communication Skill- score |
4 |
6 |
6 |
8 |
2 |
8 |
|
2 |
Wong baker pain rating scale |
10 |
2 |
6 |
0 |
8 |
0 |
Table 4: Assessment of Scale.
In addition the outcomes of the patient was also assessed on Modified Naranjo Criteria in Homeopathy (MONARCH) This tool helped in mapping the outcomes achieved in patients on 10 domains as listed below (Table 5):
|
Domains |
Yes |
No |
Not Sure or N/A |
|
|
1 |
Was there an improvement in the main symptom or condition for which the homeopathic medicine was prescribed? |
+2/+2 |
- |
- |
|
2 |
Did the clinical improvement occur within a plausible timeframe relative to the drug intake? |
+1/+1 |
- |
- |
|
3 |
Was there an initial aggravation of symptoms? |
0/0 |
+1/+1 |
- |
|
4 |
Did the effect encompass more than the main symptom or condition (i.e., were other symptoms ultimately improved or changed)? |
+1/+1 |
- |
- |
|
5 |
Did overall well-being improve? (suggest using validated scale) |
+1/+1 |
- |
- |
|
6A |
Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? |
0 |
- |
- |
|
6B |
Direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms: –from organs of more importance to those of less importance? –from deeper to more superficial aspects of the individual? –from the top downwards? |
0 |
- |
- |
|
7 |
Did “old symptoms” (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? |
0/0 |
- |
- |
|
8 |
Are there alternate causes (other than the medicine) that—with a high probability—could have caused the improvement? (Consider known course of disease, other forms of treatment, and other clinically relevant interventions) |
+1/+1 |
- |
- |
|
9 |
Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation, etc.) |
+2/+1 |
- |
- |
|
10 |
Did repeat dosing, if conducted, create similar clinical improvement? |
+1/+1 |
- |
- |
|
|
Total score |
10/9 |
|
|
|
Note: Maximum score=13, minimum score = -6 |
||||
Table 5: Patient outcome assessment on Modified Naranjo Criteria in Homeopathy (MONARCH) Assessment of both patient are separated by a / (H-343/H-361).
Discussion
Both the patients were diagnosed case of severe haemophilia A. One patient had a strong genetic history while the other didn’t. Both the patients started homoeopathic treatment at an early age. As the children were growing they were facing the difficulties faced by haemophilics [13]. There were many episodes of bleeds, mostly managed with Hammamelis Q, acute medicines, medicines from emergency kits (in acute emergency at any time in the day via teleconsultation) & constitutional medicines. H-343 has not required any factor infusion after starting with homoeopathic medicines (i.e. since the age of 7 months till 6 years of age). H-361 required factor infusion five times in between after starting with homoeopathic medicines (i.e. since the age of 1 year till 5 years of age). Patient outcome assessment score on Modified Naranjo Criteria in Homeopathy (MONARCH) was 10 & 9 respectively (Table 5).
Results
From the time patient started with homoeopathic treatment- Out of the 2 patient, 1 patient did not required any factor infusion and the other patient required factor concentrate in five episodes of bleeding whereas all other acute emergencies were managed with homoeopathic medicines.
Conclusion
Homoeopathic medicine helps in managing acute bleeding episodes in haemophilia patients of pediatric age group and acts as a good adjunct.
Acknowledgment
The authors show sincere gratitude to Prof. (Dr.) Kanjaksha Ghosh, Former Director, National Institute of Immunohaematology, KEM Hospital, Parel, Mumbai for his whole hearted guidance and scientific support to all the projects of Homoeopathy In Haemophilia.
Conflicts of Interest
Authors declare no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Jorde LB, Carey JC, Bamshad MJ (2003) Medical Genetics. Elsevier, Amsterdam, Netherlands.
- National Organization for Rare Disorders (2021) List of Rare Disease Information- NORD. National Organization for Rare Disorders, USA.
- Ghosh K, Ghosh K (2021) Overcoming the challenges of treating haemophilia in resource-limited nations: a focus on medication access and adherence. Expert Review of Hematology 14: 721-730.
- Hiral S, Tapas K, Afroz S (2020) Homoeopathic Management of a case of Severe Haemophilia Type A with Inhibitor Positive: Case report. Homoeopathic Links 33: 302-308.
- Centers for Disease Control and Prevention (2021) Inhibitors and Hemophilia. Centers for Disease Control and Prevention, USA.
- Sakha The Centre of Research and Charity's - Homoeopathy in Haemophilia (2021) Homoeopathy in Haemophilia. Sakha The Centre of Research and Charity's - Homoeopathy in Haemophilia, India.
- Wong DL, Eaton MH, Wilson D, Winkelstein ML, Schwartz P (2001) Wong’s essentials of pediatric nursing. St. Louis, USA.
- Duijn GV, Dijkxhoorn Y, Noens I, Scholte E, Onnes IB (2009) Vineland Screener0-12 years research version (NL). Constructing a screening instrument to assess adaptive behaviour. Int J Meth Psychiatr Res 18: 110-117.
- RADAR (2021) 10.5-open the homeopathic software. Jain publishers, India.
- MIASMS (2021) A New Perspective on the Hereditary Factor. MIASMS, India.
- Boericke W (1980) Pocket Manual of Homoeopathic Materia Medica and Repertory. B Jain Publishers Pvt Ltd, India.
- Allen HC (1998) The Materia Medica of the Nosodes with Provings of the X-Ray. B Jain Publishers Pvt Ltd, India.
- Lee CA, Berntop EE, Hoots WK (2010) Text book of hemophilia. Wiley Blackwell, USA.
Citation: Hiral B, Tapas K, Afroz S, Omkar K (2021) Homoeopathic Management of Severe Haemophilia in Pediatric age group: Twin Case Study. J Altern Complement Integr Med 7: 214.
Copyright: © 2021 Bothra Hiral, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.