Impact of COVID 19 Pandemic in Hemodialysis Units in Mexico
*Corresponding Author(s):
Bueno-Hernández JFHemodialysis Unit, Renal Assistance Center, Estado De México ZC 53100, Mexico
Tel:+52 5530388877,
Email:francisco.bueno@hemocare.com.mx
Abstract
Since the World Health Organization (WHO) declared the pandemic associated with COVID 19, our hemodialysis center took up preventive measures based on the literature on this matter, and created an algorithm for restraining and avoiding further transmission of the virus.
Nevertheless, in México, there is not current information about the incidence and prevalence of this disease on patients taking hemodialysis treatment.
Given this lack of information, our unit considers necessary to carry out an observational, descriptive, cross-sectional and retrospective study, with the objective of knowing the prevalence and mortality, as well as the clinical and nutritional characteristics of patients infected with COVID 19.
Keywords
Chronic kidney disease; COVID-19; Hemodialysis; Renal disease
INTRODUCTION
On December 31, 2019, the WHO (World Health Organization) was informed by the Chinese authorities of 27 cases of pneumonia of unknown etiology in the city of Wuhan; identifying a new coronavirus as a possible etiological agent. The current outbreak declared by the WHO as a Public Health Emergency of International Importance (ESPII) was in fact, caused by this new agent, later named as COVID-19, abbreviation for "coronavirus disease 2019” [1].
Given the alarming levels of global spread; On March 11, 2020, the WHO officially declared the pandemic associated with COVID 19, with a record of 332,930 confirmed cases and 14,509 deaths [2]. The absence of specific treatments and the high degree of contagion called for the need to use public strategies aimed at reducing the rates of contacts in the population and the transmission of the virus. The governments' priority focused on keeping mortality as low as possible and avoiding the collapse of health systems, therefore extraordinary measures of isolation, quarantine and social distancing of communities were taken to contain the infection [3]. The Mexican government indicated the suspension of non-essential activities of the public, private and social sectors, as well as the extension of the National Day of Healthy Distance [4].
However, these measures cannot be carried out by all the population, being the case of hemodialysis patients [5,6]. There have been reports of patients in need of this treatment around the world (China [7,8], Italy [9] and Spain [10]) that report a lower prevalence and mortality than expected in this subgroup; since by attending treatment centers have a higher risk of exposure and transmission of the virus, both to their family members and to others patients, medical staff, facility workers, and everyone in contact.
Mexico has been one of the most affected countries in the world by the COVID 19 infection, proved by statistics showing that in November 26 there were already 1,078,594 confirmed cases and 104,242 deaths, with one of the highest fatality rates (9.8%) [11], both in general population and in health personnel [12]. In our hemodialysis center, preventive measures were carried out based on what is described in the international literature to help contain and avoid the transmission of the virus [13]. However, in México there is no current information related to the incidence and prevalence of this disease in hemodialysis patients. Given this lack of information in our unit, we consider it necessary to carry out an observational, descriptive, cross-sectional and retrospective study, in order to know the prevalence and mortality, as well as the clinical and nutritional characteristics of patients infected with COVID 19 (Figure 1).
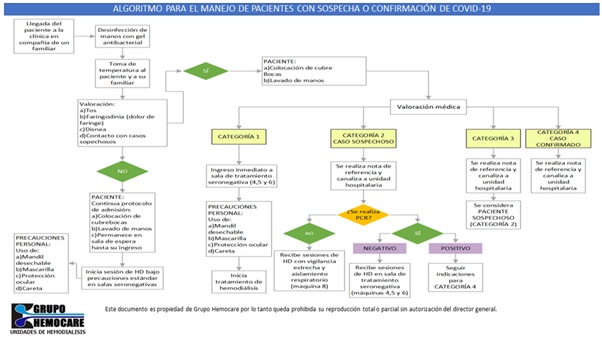
Figure 1: Algorithm of the “Follow-up and action protocol for suspected cases of SARS infection-CoV-2 of the renal assistance center "CARE".
MATERIAL AND METHODS
From the month of March to September 2020, 1308 patients who received their hemodialysis treatment in the outpatient clinics of the CARE Renal Assistance Center were monitored, and those with a diagnosis of COVID 19 by a positive PCR test, who were older than 18 years old, with laboratory results and nutritional evaluations, were included.
Once the patients were recognized, the demographic characteristics, causal diagnosis of CKD, length of stay on hemodialysis, and presence of previous comorbidities; biochemical, nutritional indicators and symptoms of COVID-19 infection were reviewed. The outcome of the disease was sought by grouping them into survivors and deaths.
The results were reported in measures of central tendency and dispersion according to the variable distribution; variables with normal distribution such as age and biochemical indicators were reported in means ± standard deviation and non-parametric distributions such as months on hemodialysis and gender in medians and interquartile range. Nominal variables such as diagnosis of Chronic Kidney Disease or comorbidities were reported in percentages. The Chi-square test was used to demonstrate differences between the outcome groups.
A p<0.05 was considered significant, in order to perform the statistical tests, the SPSS version 22 statistical package was used.
The study protocol was evaluated and approved by the research ethics committee of the Renal Assistance Center (CARE) in accordance with the provisions of the General Health Law of Mexico, and based on the declaration of Helsinki for the collection, storage and use of data contained in medical records.
RESULTS
Of our total population of 1308 patients, 63 (4.8%) were confirmed to have COVID-19 infection.
The baseline characteristics of the studied population show that most cases are male, with a causal diagnosis of Chronic Kidney Disease due to diabetic nephropathy and a high prevalence of associated comorbidities such as diabetes and hypertension, the patients were young with a median of 48 years of age, and more than 30 months in hemodialysis replacement therapy. No significant differences were found between groups except for the presence of cardiovascular disease, which was more frequent in the group of patients with COVID-19 (Table 1).
|
Variable |
General population No.1245 ± D.E. (%); Median (I.I.C) |
COVID-19 cases No.63 ± D.E. (%); Median (I.I.C) |
p |
|
Age (years) |
48.26 (34-62) |
48.97±14.94 |
0.869 |
|
Gender |
|||
|
Men |
705 (56.6%) |
43 (68.3%) |
0.095 |
|
Months in HD |
28 (9-63) |
32 (14-78) |
0.54 |
|
Causal Diagnosis |
|||
|
DM2 |
450 (36.1%) |
25 (39.7%) |
|
|
Unknown |
281 (22.6%) |
18 (28.5%) |
0.525 |
|
GMN |
162 (13.0%) |
10 (15.9%) |
|
|
Other |
352 (28.3%) |
10 (15.9%) |
|
|
Comorbidities |
|||
|
DM2 |
453 (40.6%) |
29 (46%) |
0.323 |
|
HAS |
863 (76.7%) |
59 (93.7%) |
0.099 |
|
>60 ã |
375 (30.1%) |
17 (27%) |
0.609 |
|
Cardiovascular Disease |
14 (1.1%) |
7 (11.1%) |
0.034 |
|
Respiratory Disease |
15 (1.2%) |
1 (1.6%) |
0.558 |
|
Other |
290 (24.7%) |
10 (30.2%) |
0.088 |
|
Outcome |
|||
|
Deceased |
201 (20.1 %)a |
26 (41.3%)b |
0.168 |
|
(a) Other causes |
|||
|
(b) COVID 19 |
Table 1: Demographic characteristics of the general population vs. cases COVID-19.
When analyzing the confirmed cases grouped by survivors and deceased, we can observe similar age ranges. Visually, the patients who died were older compared to the survivors, however this difference was not statistically significant [14].
Regarding the comorbidities presented, we found that 65.4% of the deceased patients had diabetes mellitus 2 compared to 32.4% of the patients who survived, this difference being statistically significant. No other statistical differences were found between groups (Table 2).
|
Variable |
Survivors No.37 ± D.E. (%); Median (I.I.C) |
Deceased No.26 ± D.E. (%); Median (I.I.C) |
P |
|
Age (years) |
47.3±14.29 |
51.35±15.8 |
0.303 |
|
Gender |
|
|
|
|
Men |
24 (64.9%) |
19 (73.1%) |
|
|
Months in HD |
32 (11-86) |
29 (18.5-64.25) |
0.68 |
|
Comorbidities |
|||
|
DM2 |
12 (32.4%) |
17 (65.4%) |
0.01 |
|
HAS |
34 (91.9%) |
25 (96.2%) |
0.495 |
|
>60 ã |
8 (21.6%) |
9 (34.6%) |
0.253 |
|
Cardiovascular Disease |
4 (10.8%) |
3 (11.5%) |
0.928 |
|
Respiratory Disease |
1 (2.7%) |
0 (0%) |
0.398 |
|
Other |
11 (29.7%) |
8 (30.8%) |
0.929 |
|
Hemoglobin (g/dL) |
10.09±2.74 |
9.36±2.51 |
0.272 |
|
Platelets (thousands/L) |
208.8±79.2 |
238.2±102.6 |
0.226 |
|
Neutrophils (%) |
62.03±9.91 |
57.89±11.05 |
0.133 |
|
Leukocytes (thousands/L) |
5.58±1.5 |
5.99±1.96 |
0.369 |
|
Lymphocytes (%) |
29.25±8.71 |
32.5(23.3-39) |
0.525 |
|
CTL |
1645.9±609.9 |
1826.3±583.9 |
0.241 |
|
Transferrin (mg/L) |
203.54±70.25 |
205.5 (155.5-257.3) |
0.418 |
|
Ferritin (mg/dL) |
269 (41-1121) |
159.5 (28-419.5) |
0.211 |
|
Glucose (mg/dL) |
109 (92-127) |
135.9±63.51 |
0.39 |
|
BUN (mg/dL) |
60 (47-71.5) |
62.19±15.52 |
0.557 |
|
Sodium (meq/L) |
136.4±3.6 |
134.73±3.48 |
0.073 |
|
Potassium (meq/L) |
4.91±0.89 |
5.24±0.80 |
0.138 |
|
Calcium (mg/dL) |
8.44±0.89 |
8.55 (7.85-9.2) |
0.6 |
|
Phosphorus (mg/dL) |
5.4 (4.2-6.8) |
5.4±1.53 |
0.989 |
|
Total protein (g/dL) |
6.71±0.62 |
6.89±0.64 |
0.239 |
|
Albumin (g/dL) |
3.7 (3.35-3.95) |
3.79±0.38 |
0.313 |
|
Kt/V |
1.74±0.34 |
1.78±0.36 |
0.597 |
Table 2: Demographic and biochemical characteristics of patients with COVID-19 survivors vs. deceased.
Nutritional status was analyzed by different screening tools, observing that more than 50% of the patients in both populations were well nourished. Visually, a higher percentage of severe malnutrition is observed in confirmed deceased patients using the following tools: Subjective Global Assessment and Bilbrey Index. Nonetheless, these differences were not statistically significant (Table 3).
|
Variable |
Survivors No. 37 ± D.E; (%); Median (I.I.C) |
Deceased No. 26 ± D.E; (%); Median (I.I.C) |
|
|
BMI |
|||
|
Low weight |
2 (5.4%) |
2 (7.7%) |
|
|
Normal |
16 (43.2%) |
12 (46.2%) |
0.756 |
|
Overweight |
12 (32.4%) |
10 (38.5%) |
|
|
Obesity |
7 (18.9%) |
2 (7.7%) |
|
|
Subjective Global Assessment (EGS) |
|||
|
Normal |
27 (73%) |
14 (53.8%) |
0.067 |
|
Mild/Moderate |
10 (27%) |
9 (34.6%) |
|
|
Serious |
- |
3 (11.5%) |
|
|
Bilbray Index (BI) |
|||
|
Normal |
19 (51.4%) |
11 (42.3%) |
|
|
Slight |
12 (32.4%) |
8 (30.8%) |
0.534 |
|
Moderate |
5 (13.5%) |
4 (15.4%) |
|
|
Serious |
1 (2.7%) |
3 (11.5%) |
Table 3: Nutritional status in patients with COVID-19 survivors vs. deceased.
The clinical symptoms reported by both groups were similar, except for the presence of nausea and vomiting in the deceased patients, showing a statistically significant difference in the presentation of both symptoms (Table 4).
|
Variable |
Survivors No. 37 ± D.E; (%); Median (I.I.C) |
Deceased No. 26 ± D.E; (%); Median (I.I.C) |
p |
|
Fever |
28 (75.7%) |
19 (73.1%) |
0.816 |
|
Cough |
28 (75.7%) |
14 (53.8%) |
0.07 |
|
Dyspnea |
18 (48.6%) |
15 (57.7%) |
0.479 |
|
Asthenia |
11 (29.7%) |
6 (23.1%) |
0.558 |
|
Adynamic |
11 (29.7%) |
6 (23.1%) |
0.558 |
|
Arthralgias |
10 (27%) |
6 (23.1%) |
0.723 |
|
Myalgias |
10 (27%) |
5 (19.2%) |
0.474 |
|
Odynophagia |
4 (10.8%) |
0 (0%) |
0.083 |
|
Diarrhea |
6 (16.2%) |
6 (23.1%) |
0.495 |
|
Headache |
3 (8.1%) |
5 (19.2%) |
0.192 |
|
Chest pain |
1 (2.7%) |
1 (3.8%) |
0.799 |
|
O2 Requirement |
5 (13.5%) |
2 (7.7%) |
0.469 |
|
Conjunctivitis |
2 (5.4%) |
0 (0%) |
0.228 |
|
Nausea |
0 (0%) |
3 (11.5%) |
0.034 |
|
Vomiting |
0 (0%) |
3 (11.5%) |
0.034 |
|
General Discomfort |
10 (27%) |
7 (26.9%) |
0.993 |
|
Shudder |
4 (10.8%) |
3 (11.5%) |
0.928 |
Table 4: Clinical symptoms in patients with COVID-19, surviving patients vs. deceased.
DISCUSSION
Hemodialysis services in the State of Mexico cover a population of approximately 16.19 million inhabitants. Our Center provides care for more than 1,300 patients, of which 281 are concentrated in the main unit located in the municipality of Naucalpan, and in two peripheral units; one with 354 patients located in Ixtapaluca and the largest with 635 patients located in Ecatepec, all in the State of Mexico. It should be noted that this last municipality has been the highest in incidence of COVID-19 infection in our country, being a district area with overpopulation, high unemployment rates, poverty and low education index, which favors the transmission of the disease by COVID-19.
In our country, access to public health has been affected by the pandemic, with care being limited for any other illness and in the specific case of COVID-19 infection. Hospitals treating this condition have been overwhelmed by the demand for attention, which favors the probability of not diagnosing the carrier and in the case of our population, the patient on hemodialysis continues to attend their sessions, breaking the confinement at home and thus increasing the risk of contagion.
As we could see in the results, the mean age of our general population was 48 years old; however, the deceased patients had a tendency to be older (51.35 years old) compared to the survivors (47.3 years old). Different from what was previously reported in the literature; In Italy, the average age reported was 75 years for deceased patients and 69 years for COVID-19 survivors, according to the study by Goicoechea y cols. , similar to the data found by Yiqiong y cols. in Wuhan, China where the age of the patients was 71 years. It is important to recognize that the mean age in the Mexican population is 29.2 years compared to the mean age of Italy, which is around 45.7 years or that of China, which is 36 years, which would explain why Mexican patients are younger.
Diabetes mellitus was higher in the group of deceased by 64.5% compared to 32.4% of the survivors (p=0.010), which to date is a known risk factor for severity of COVID-19 worldwide.
The percentage of patients in our hemodialysis center confirmed with COVID-19 was 4.8%, which is lower than what was reported in other countries such as China, Spain and Italy (18.23, 12.77 and 6.5% respectively), although this could be a result of an under diagnosis due to the lack of carrying out confirmatory tests by PCR in our country, since currently, according to the OECD, Mexico ranks last in the application of diagnostic tests for COVID-19.
When analyzing the percentage of mortality, it is observed that 41% of the patients with COVID-19 died, compared with the 5.65% mortality reported by Yiqiong et al. in China, which is a reflection of the national situation, since Mexico has one of the highest fatality rates in the world. Currently in our country the fatality rate for COVID 19 is 9.8% which reached its maximum peak in July 2020 with 12.4%.
In our population, the mortality rate during the studied pandemic months was 13.98%, in 2019 during the same period it was 9.18%.
As expected, the impact of the pandemic has been reflected in the increase of mortality in patients, since many, due to the fear of contagion, omitted their medical consultations, delaying the care of conditions independent of COVID-19.
No differences were found in nutritional status or biochemical indicators between both groups. It should be noted that our patients have been on hemodialysis for several years and have stable biochemical concentrations, and most of them have a good nutritional status. Regarding the symptoms of COVID-19, more than 70% presented fever, more than 50% cough and more than 40% dyspnea. Patients who died had a higher percentage of gastrointestinal symptoms (diarrhea 23.1% died, vs. 16.2% recovered; nausea 11.5% vs. 0% and vomiting 11.5% vs. 0% respectively) compared to the survivors where the symptoms were mainly respiratory, for what is required of studies with a larger sample to determine if this could be a factor of severity in the patient with chronic kidney failure and COVID-19.
In the population of clinic employees, the percentage of COVID-19 infection was 6.9% (19 out of 274) compared to the 12.12% reported by Yiqiong Ma et al. in China, being the operational areas in direct contact with patients, those who were most affected.
CONCLUSION
The impact that COVID-19 pandemic has left in Mexico has been devastating. Being the fourth country with the highest number of deaths from COVID-19 according to the UN, as of November 2020 with more than 100,000 deaths and more than one million of confirmed cases. Hemodialysis units are not the exception to this tragedy, so this study's main objective is to show the country and the world the measures that were carried out to try to prevent infections and describe the behavior of the COVID-19 pandemic in our hemodialysis patients population.
Among the limitations of the study is the number of patients confirmed by a positive PCR test, since in many of the cases, despite the clinical suspicion, this confirmation was not available.
In our hemodialysis centers, the measures recommended by international and national organizations were carried out; however, despite this, the lethality of COVID-19 in our population was high.
Our intention is to contribute as a national and international reference on how the COVID-19 pandemic has affected hemodialysis units in Mexico, in order to improve preventive guidelines, avoid infections, as well as complications and deaths associated with this condition.
REFERENCES
- Patiño-Lugo DF, Vélez M, Salazar PV, Vera-Giraldo CY, Velez V, et al. (2020) Non-pharmacological interventions for the containment, mitigation and suppression of COVID-19 infection. Colomb Med 51: 4266.
- World Health Organization (2020) Coronavirus disease 2019 (COVID-19): Situation report-63.
- Evidence and Deliberation Unit for Decision Making (UNED) (2020) Quick synthesis. Non-pharmacological interventions for the containment, mitigation and suppression of COVID-19 infection.
- Secretary of Health (SSA) Statement begins phase 3 by Covid-19.
- International Society of Nephrology (2020) Recommendations for the prevention and treatment of COVID-19.
- Kliger AS, Cozzolino M, Jha V, Harbert G, Ikizler TA (2020) Managing the COVID-19 pandemic: International comparisons in dialysis patients. Kidney Int 98: 12-16
- Ma Y, Diao B, Lv X, Liang W, Zhu J, et al. (2020) COVID-19 in hemodialysis (HD) patients: Report from one HD center in Wuhan, China.
- Wang R, Liao C, He H, Hu C, Wei Z, et al. (2020) COVID-19 in hemodialysis patients: A report of 5 cases. American Journal of Kidney Diseases 76.
- Esposito P, Russo R, Conyti N, Falqui V, Massarino F, et al. (2020) Management of COVID-19 in hemodialysis patients: The Genoa experience. Hemodial Int 24: 423-427.
- Goicoechea M, Cámara LAS, Macías N, de Morales AM, Rojas ÁG, et al. (2020) COVID-19: Clinical course and outcomes of 36 hemodialysis patients in Spain. Kidney Int 98: 27-34.
- Informe Técnico Diario COVID-19 MÉXICO.
- Agren D (2020) Understanding Mexican health worker COVID-19 deaths. Lancet 396: 807.
- Vega-Vega O, Arvizu-Hernández M, Domínguez-Cherit JG, Sierra-Madero J, Correa-Rotter R (2020) Prevention and control of SARS-CoV-2 (Covid-19) coronavirus infection in hemodialysis units. Salud Publica Mex 62: 341-347.
- Unit of Evidence and Deliberation for Decision Making (UNED) (2020) Quick synthesis. Non-pharmacological interventions for the containment, mitigation and suppression of COVID-19 infection.
Citation: Bueno-Hernández JF, Islas-Olvera C, Arceo-Venegas E, Morales-Salgado A, Edgar RES (2021) Impact of COVID 19 Pandemic in Hemodialysis Units in Mexico. J Nephrol Renal Ther 7: 048.
Copyright: © 2021 Elías Arceo-Venegas, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.