Incidental Finding of A Fenestrated Vertebrobasilar Junction Aneurysm
*Corresponding Author(s):
Geraud AkpoDepartment Of Radiology And Medical Imaging, FANN Hospital, Dakar, Senegal
Tel:+221 775429470,
Email:geraudakpo@hotmail.com
Abstract
We report the case of a sacculara neurysm of the fenestrated vertebrobasilar junction in a 57-year-old woman, incidentally discovered. The diagnosis was made on CT brain angiography which found the an atomical variant and the aneurysm.
Vertebrobasilar junction aneurysms are uncommon but often associated with a fenestration of the basilar artery.
We detail the radiological features illustrating this association.
Keywords
Basilar artery fenestration; CT brain angiography; Vertebrobasilar aneurysm
Introduction
We report here a case of an incidental discovery of this association in a patient received for a suspected cerebral venous thrombosis.
Basilarartery fenestration is an anatomical variant consisting of a focal duplication located on any segment of the artery.
It results from an incomplete fusion of the two vertebral arteries during embryonic life. In order of frequency, it is the second most common location of vascular fenestrations after the anterior comminuted artery [1].
Aneurysms of the vertebrobasilar junction are rare, representing lessthan 0.5% of intracranial aneurysms, and are associated in 70% of cases with a fenestration of the basilar trunk [2].
We report here the case of an incidental discovery of this association in a patient received for a suspected cerebral venous thrombosis.
Observation
The patient was a 57-year-old woman with a history of pulmonary embolism who was referred to our department for a cerebral CT angiography for a suspected cerebral venous thrombosis.
CT revealed a large saccular aneurysm of 13 x 16 mm, with a wide neck (05 mm), implanted on an asymmetric fenestration of the vertebrobasilar junction, without any sign of complication (Figures 1-3).
No other vascular abnormalities were noted, and the dural venous sinuses in particular were permeable.
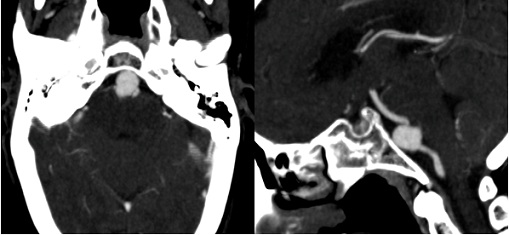 Figure 1: Cerebral CT angiography. A) Oblique axial section and sagittal reconstruction; B) Show a large unruptured saccular aneurysm (blue arrows) on the proximal portion of the basilar trunk (red arrow).
Figure 1: Cerebral CT angiography. A) Oblique axial section and sagittal reconstruction; B) Show a large unruptured saccular aneurysm (blue arrows) on the proximal portion of the basilar trunk (red arrow).
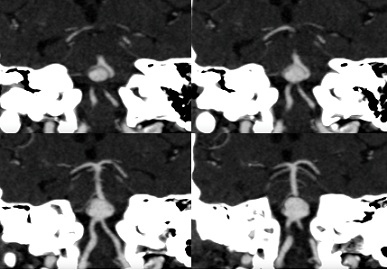 Figure 2: Oblique coronal reconstructions with MIP (Maximum Intensity Projection) allow visualization of the asymmetric fenestration of the basilar artery at its origin, with a right branch (blue arrow) and a dominant left branch (green arrow), surrounding the aneurysmal sac (red arrows).
Figure 2: Oblique coronal reconstructions with MIP (Maximum Intensity Projection) allow visualization of the asymmetric fenestration of the basilar artery at its origin, with a right branch (blue arrow) and a dominant left branch (green arrow), surrounding the aneurysmal sac (red arrows).
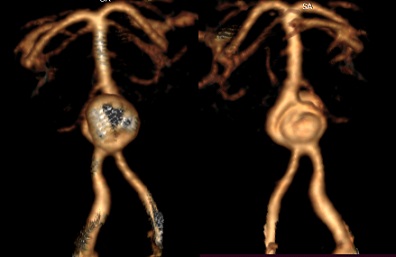 Figure 3: 3D VRT (Volume Rendering Technique) reconstructions: anterior (A) and posterior (B) views showing the aneurysm developed on the fenestration of the vertebrobasilar junction.
Figure 3: 3D VRT (Volume Rendering Technique) reconstructions: anterior (A) and posterior (B) views showing the aneurysm developed on the fenestration of the vertebrobasilar junction.
Discussion
The first case of this rare entity was described in 1979 by Hoffman, et al. [3]. Embryologically, the basilar trunk is formed by the union of the two vertebral arteries around the 7th week of amenorrhea. Any fusion anomaly may result in a focal duplication of the basilar artery [4].
This can occur over the entire height of the artery but predominates in the proximal segment [5]. A classification based on the relationship between the fenestration and the origin of the Anterior Inferior Cerebell Ararteries (AICA) distinguishes 04 types (Figure 4) [6,7]:
- Type I: the fenestration is located up stream of the origin of the AICA (this is the case of our patient);
- Type II: the two AICA s are born symmetrically on the fenestration;
- Type III: emergence of a single AICA on the fenestration;
- Type IV: the fenestration is located down stream from the origin of the AICA.
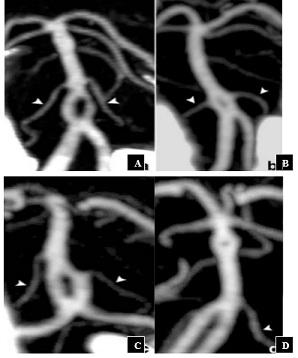 Figure 4 : Classification of basilarartery fenestrations. According to Gao, et al. [7] ; Type I (A): Fenestration before the emergence of the AICAs, Type II (B): Emergence of the two AICAs on fenestration, Type III (C): Emergence of a single AICA on fenestration, Type IV (D): Fenestration down stream from the origin of the AICAs.
Figure 4 : Classification of basilarartery fenestrations. According to Gao, et al. [7] ; Type I (A): Fenestration before the emergence of the AICAs, Type II (B): Emergence of the two AICAs on fenestration, Type III (C): Emergence of a single AICA on fenestration, Type IV (D): Fenestration down stream from the origin of the AICAs.
Although rare, aneurysms of the vertebrobasilar junction are associated in 70% with a fenestration of the basilar trunk [2].
The occurrence of this association is explained by the presence of parietal abnormalities related to these anatomical variants: locally absent media, discontinuity of the elastin, and locally thinned subendothelium. This parietal fragility, added to the turbulence of the arterial flow, predisposes to the formation of aneurysms [5,6,8].
CT angiography is currently the best technique for the diagnosis and preoperative evaluation of these aneurysms. The 3D VRT reconstructions are valuable to understanding their often complex anatomy [9].
Their localization makes surgical treatment delicate because of the presence of narrow vascular-nervous relationships and the difficulty of finding an adequate approach. The current treatment is based on endovascular coil embolization [4,8,9].
Conclusion
Aneurysms of the vertebrobasil arregion are rare and their presence should be investigated for associated fenestration, which is a predisposing factor. Radiologists and neuro surgeons should be aware of this high probability of lesion association.
Competing Interests
The authors declare no competing interests
References
- Trivelato FP, Abud DG, Nakiri GS, de Castro Afonso LH, Ulhôa AC, et al. (2016) Basilar Artery Fenestration Aneurysms: Endovascular Treatment Strategies Based on 3D Morphology. Clin Neuroradiol 26: 73-79.
- Peluso JPP, Van Rooij WJ, Sluzewski M, Beute GN (2007) Aneurysms of the vertebrobasilar junction: incidence, clinical presentation, and outcome of endovascular treatment. Am J Neuroradiol 28: 1747-1751.
- Hoffman WF, Wilson CB (1979) Fenestrated basilar artery with an associated saccular aneurysm: Case report. J Neurosurg 50: 262-264.
- Albanese E, Russo A, Ulm AJ (2009) Fenestrated vertebrobasilar junction aneurysm: diagnostic and therapeutic considerations: Case report. J Neurosurg;110: 525-529.
- Peltier J, Gayet J-B, Toussaint P, Deramond H, Le Gars D (2006) Anévrisme termino-vertébral sur fenestration de l’artère basilaire. Neurochirurgie 52: 52-56.
- Tanaka M, Kikuchi Y, Ouchi T (2006) Neuroradiological Analysis of 23 Cases of Basilar Artery Fenestration Based on 2280 Cases of MR Angiographies. Interv Neuroradiol 12: 39-44.
- Gao L, Guo X, Zhou J, Zhang Q, Fu J, et al. (2013) Basilar artery fenestration detected with CT angiography. Eur Radiol 23: 2861-2867.
- Saatci I, Cekirge HS, Karcaaltincaba M, Basgun N, Berker M, et al. (2002) Endovascular treatment of kissing aneurysms at the fenestrated basilar artery. Case report with literature review. Surg Neurol 58: 54-58.
- Ezaki Y, Kazekawa K, Tsutsumi K, Yagi N, Mori K, et al. (2003) A vertebrobasilar junction aneurysm associated with fenestration treated by intra-aneurysmal embolization. Acta Neurochir (Wien) 145: 807-809.
Citation: Kasse Y, Akpo G, Niang I, Ka KD, Diagne R, et al. (2021) Incidental Finding of A Fenestrated Vertebrobasilar Junction Aneurysm. J Angiol Vasc Surg 6: 083.
Copyright: © 2022 Youssoupha Kasse, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.