Journal of Physical Medicine Rehabilitation & Disabilities Category: Medical
Type: Research Article
Isokinetic Analysis of Rotator Cuff Musculature of Sedentary Wheelchair Users and Basketball Athletes with Spinal Cord Injury
*Corresponding Author(s):
Poliane Silva FreitasDepartment Of Biomechanics, Medicine And Rehabilitation Of The Locomotor Apparatus, Ribeirão Preto Medical School, University Of São Paulo, Brazil
Tel:+55 16981344785,
Email:fisiopolifreitas@gmail.com
Received Date: Mar 17, 2017
Accepted Date: May 02, 2017
Published Date: May 16, 2017
Abstract
Objectives
This study aimed to compare the isokinetic parameters of the rotator cuff in the shoulders of paraplegic wheelchair basketball athletes and sedentary controls.
Design
Cross - sectional study.
Methods
An isokinetic evaluation was performed to quantify the peak torque, power, and work exerted by the rotator cuff muscle group, using a biodex system. All thirty-six individuals with spinal cord injury, aged between 18 and 45 years. Concentric isokinetic tests were performed in the seated position with the shoulder at 45° abduction from the scapular plane and flexed at 30° to the frontal plane. Subjects completed five repetitions at 60°/s and 180°/s, and ten repetitions at 300°/s, bilaterally, with an interval of one minute between each series. For the statistical analysis, the t - test was used with an alpha of 5%.
Results
Peak torque/weight, work, and muscle power of wheelchair basketball athletes were significantly greater than those of the control group (p<0.05). There was no statistical difference when comparing the dominant limb with - dominant one in either group. Internal rotators were stronger than the external rotators both for athletes and for non - athletes.
Conclusions
Wheelchair basketball athletes presented, bilaterally, greater values for muscle performance (torque, work, and power). These results suggest that the wheelchair sport influences the shoulder musculature of those with traumatic spinal cord injury.
This study aimed to compare the isokinetic parameters of the rotator cuff in the shoulders of paraplegic wheelchair basketball athletes and sedentary controls.
Design
Cross - sectional study.
Methods
An isokinetic evaluation was performed to quantify the peak torque, power, and work exerted by the rotator cuff muscle group, using a biodex system. All thirty-six individuals with spinal cord injury, aged between 18 and 45 years. Concentric isokinetic tests were performed in the seated position with the shoulder at 45° abduction from the scapular plane and flexed at 30° to the frontal plane. Subjects completed five repetitions at 60°/s and 180°/s, and ten repetitions at 300°/s, bilaterally, with an interval of one minute between each series. For the statistical analysis, the t - test was used with an alpha of 5%.
Results
Peak torque/weight, work, and muscle power of wheelchair basketball athletes were significantly greater than those of the control group (p<0.05). There was no statistical difference when comparing the dominant limb with - dominant one in either group. Internal rotators were stronger than the external rotators both for athletes and for non - athletes.
Conclusions
Wheelchair basketball athletes presented, bilaterally, greater values for muscle performance (torque, work, and power). These results suggest that the wheelchair sport influences the shoulder musculature of those with traumatic spinal cord injury.
Keywords
Isokinetic evaluation; Shoulder; Strength
INTRODUCTION
Wheelchair basketball is disseminated worldwide and is practiced for competition, recreation and rehabilitation of people with disabilities in the lower limbs. Spinal cord injured individuals lose motor control of lower limbs to the extent that they need to use their upper limbs as an alternative to performing daily activities such as transfers, pressure relief and locomotion [1-4], so they are current candidates to practice this sport modality. Typically wheelchair basketball produces a major overload to the upper limbs, characterized by locomotion on the court as well as to other movements demanded during the game such as passing, rebounding, dribbling and shooting [5].
This study have determined the importance of muscle strength in sport, and it is perhaps even greater in adapted sports, where players with spinal cord injury may experience a loss of active fibers and muscle mass due to their particular injury [6]. In this regard, some researchers have stated that both the player’s functional potential and their strength will influence physical performance in practice sports [7].
Muscle strength can be assessed by different methods according to the type of contraction: isometric, isokinetic, and isotonic [8]. The isokinetic dynamometer proved to be reliable to measure muscle strength, by allowing the evaluation of peak torque, work and power at a previously determined constant angular velocity [8].
Aspects such as muscle imbalance [2], on - court agility lateral stiffness [9], incidence of musculoskeletal injuries [10] and pain in wheelchair basketball athletes [7,11-13], have already been addressed in the literature. However, there is a gap concerning the comparison of isokinetic shoulder evaluation between sedentary and athletic individuals with traumatic spinal cord injury at different angular velocities (60, 180, and 300°/s). The objective of the present study was to compare the peak torque, work, and muscle power obtained by isokinetic dynamometry of internal and external shoulder rotators in individuals with traumatic spinal cord injury who practiced wheelchair basketball as well as those who did not.
This study have determined the importance of muscle strength in sport, and it is perhaps even greater in adapted sports, where players with spinal cord injury may experience a loss of active fibers and muscle mass due to their particular injury [6]. In this regard, some researchers have stated that both the player’s functional potential and their strength will influence physical performance in practice sports [7].
Muscle strength can be assessed by different methods according to the type of contraction: isometric, isokinetic, and isotonic [8]. The isokinetic dynamometer proved to be reliable to measure muscle strength, by allowing the evaluation of peak torque, work and power at a previously determined constant angular velocity [8].
Aspects such as muscle imbalance [2], on - court agility lateral stiffness [9], incidence of musculoskeletal injuries [10] and pain in wheelchair basketball athletes [7,11-13], have already been addressed in the literature. However, there is a gap concerning the comparison of isokinetic shoulder evaluation between sedentary and athletic individuals with traumatic spinal cord injury at different angular velocities (60, 180, and 300°/s). The objective of the present study was to compare the peak torque, work, and muscle power obtained by isokinetic dynamometry of internal and external shoulder rotators in individuals with traumatic spinal cord injury who practiced wheelchair basketball as well as those who did not.
METHODS
Participants
The present study was approved by the Ethics in Research Commission from the University of São Paulo (FMRP/USP), under the code No. 14185/2014. The volunteers signed a free and informed consent form after previous explanations on the research and the inclusion criteria analysis. It was a transversal study with collected data initially combined in only one study center.
The sample consisted of 36 male subjects with complete traumatic spinal cord injury below T1, aged between 18 and 45 years, divided into 18 wheelchair basketball athletes and 18 paraplegic non - athletic individuals. Inclusion criteria for the athletes were as follows: 1) having spinal cord injury for at least two years; 2) using a wheelchair for locomotion in daily life; 3) training, at least, three times a week; and 4) having participated in competitions for at least two years. For the non - athletes: 1) having a traumatic spinal cord injury for at least two years; 2) moving independently in a wheelchair in daily life; 3) not having practiced any other sport for at least two years. Excluded from both groups were: 1) individuals with joint deformities adjacent to the shoulders; 2) those with soft tissue injuries in the shoulders during recovery period; 3) recent surgery in upper limbs; 4) active musculoskeletal injury of upper limbs. The study evaluated wheelchairs basketball athletes and paraplegic non - athletic individuals.
All 36 subjects were classified as ASIA A.
Sample size calculation considered data from a pilot study. The average value of peak torque for external rotation of the dominant upper limb at 60º/s, corrected by the body weight, was: athletes (59.08 ± 14.68 N.m/kg) and non - athletes (43.10 ± 16.42 N.m/kg), considering the difference between the averages of 15.9 N.m/kg and a significance level of 5%. Resulted in a total of 36 subjects, being 18 athletes and 18 non - athletes.
The sample consisted of 36 male subjects with complete traumatic spinal cord injury below T1, aged between 18 and 45 years, divided into 18 wheelchair basketball athletes and 18 paraplegic non - athletic individuals. Inclusion criteria for the athletes were as follows: 1) having spinal cord injury for at least two years; 2) using a wheelchair for locomotion in daily life; 3) training, at least, three times a week; and 4) having participated in competitions for at least two years. For the non - athletes: 1) having a traumatic spinal cord injury for at least two years; 2) moving independently in a wheelchair in daily life; 3) not having practiced any other sport for at least two years. Excluded from both groups were: 1) individuals with joint deformities adjacent to the shoulders; 2) those with soft tissue injuries in the shoulders during recovery period; 3) recent surgery in upper limbs; 4) active musculoskeletal injury of upper limbs. The study evaluated wheelchairs basketball athletes and paraplegic non - athletic individuals.
All 36 subjects were classified as ASIA A.
Sample size calculation considered data from a pilot study. The average value of peak torque for external rotation of the dominant upper limb at 60º/s, corrected by the body weight, was: athletes (59.08 ± 14.68 N.m/kg) and non - athletes (43.10 ± 16.42 N.m/kg), considering the difference between the averages of 15.9 N.m/kg and a significance level of 5%. Resulted in a total of 36 subjects, being 18 athletes and 18 non - athletes.
Measures
Isokinetic evaluation was performed to quantify the peak torque corrected by weight, muscle power and work exerted by internal and external shoulder rotators using a biodex isokinetic dynamometer system 4 Pro® (biodex medical system inc., Shirley, NY, USA). Subjects completed five minutes of active free upper limb exercises to warm up the joints and muscles and received orientations about the procedure and the effort required for the test as well as the testing sequence.
Subjects were positioned and stabilized uniformly, in the seated position, with 45° of shoulder abduction in the scapular plane and 30° of shoulder flexion in the frontal plane. Range of motion was 70°, being 30° for Internal Rotation (IR) and 40° for External Rotation (ER), from a reference position of the forearm horizontal at 0°. The humerus was aligned with the rotational axis of the dynamometer. The elbow was supported at 90° of flexion and the forearm was in neutral pronation/supination. Self-adhesive straps were placed horizontally across the chest and pelvis to provide greater stabilization of the trunk to the seat and to minimize substitution during testing. This seated position was chosen in order to reduce stress and pain to the anterior capsule and rotator cuff, which could potentially alter the test results. Isokinetic assessments of IR and ER shoulder muscles in this seated position were shown to be valid and reliable [14]. The position protocol used was in agreement with the systematic review of the positional reliability of the shoulder rotators isokinetic evaluation carried out by edouard [14]. Subjects performed five sub maximal repetitions for warm-up and familiarization with movements in the isokinetic dynamometer at angular speeds of 60°/s, 180°/s and 300°/s. After this, maximal effort was made at these angular speeds to perform 5 repetitions for 60°/s and 180°/s, and 10 repetitions for 300°/s. One minute of rest separated each series of movements.
At each angular velocity, IR and ER dynamic strength was evaluated using measurements of the Peak Torque (PT) normalized to Body Weight (PTBW) (in N.m.kg - 1) to allow comparison between subjects with different morphological conditions [14].
Subjects were positioned and stabilized uniformly, in the seated position, with 45° of shoulder abduction in the scapular plane and 30° of shoulder flexion in the frontal plane. Range of motion was 70°, being 30° for Internal Rotation (IR) and 40° for External Rotation (ER), from a reference position of the forearm horizontal at 0°. The humerus was aligned with the rotational axis of the dynamometer. The elbow was supported at 90° of flexion and the forearm was in neutral pronation/supination. Self-adhesive straps were placed horizontally across the chest and pelvis to provide greater stabilization of the trunk to the seat and to minimize substitution during testing. This seated position was chosen in order to reduce stress and pain to the anterior capsule and rotator cuff, which could potentially alter the test results. Isokinetic assessments of IR and ER shoulder muscles in this seated position were shown to be valid and reliable [14]. The position protocol used was in agreement with the systematic review of the positional reliability of the shoulder rotators isokinetic evaluation carried out by edouard [14]. Subjects performed five sub maximal repetitions for warm-up and familiarization with movements in the isokinetic dynamometer at angular speeds of 60°/s, 180°/s and 300°/s. After this, maximal effort was made at these angular speeds to perform 5 repetitions for 60°/s and 180°/s, and 10 repetitions for 300°/s. One minute of rest separated each series of movements.
At each angular velocity, IR and ER dynamic strength was evaluated using measurements of the Peak Torque (PT) normalized to Body Weight (PTBW) (in N.m.kg - 1) to allow comparison between subjects with different morphological conditions [14].
Statistical analysis
Data were analyzed with the help of the prism graphPad 5.0 a program. Sample distribution was tested with the Shapiro - wilk test. The quantitative variables were summarized as means and standard-deviations, and the qualitative variables were grouped into categories and expressed in percentages. Student t-test was used to compare mean differences between the groups and between the agonist and antagonist. To define the balance between the ER and the IR musculature of the shoulder (ER/IR) at the angular velocity of 60°/s, the limit values of 66 - 75% were used for the athletes [15] and 60 - 70% for the non - athletes [16]. The significance level was set at 5%.
RESULTS
There was no statistical difference between the athlete and non - athlete regarding age, weight, height and time since injury (Table 1). Wheelchair basketball athletes presented higher peak torque, work and muscle power values of the rotator cuff when compared to the non - athletes at the velocities of 60°/s, 180°/s and 300°/s (Table 2). There was no statistical difference for the internal rotators of the non - dominant limb at the velocities of 180°/s and 300°/s. There was no statistical difference between the dominant and non - dominant limb in all tested variables and at all speeds. The athletes did not practice any resisted exercises to strengthen the shoulder girdle. Their pieces of training focused only on techniques for wheelchair mobility, throwing practice, particular basketball movements, and game tactics.
| Athletes | Non - athletes | p-value* | |
| Variables | Mean ± SD | Mean ± SD | |
| Age (years) | 35.6 ± 1.6 | 32 ± 1.8 | 0.25 |
| Weight (kg) | 75.7 ± 3.1 | 73.4 ± 4.0 | 0.65 |
| Height (cm) | 174 ± 0.02 | 171 ± 0.01 | 0.19 |
| Time since injury (years) | 11.7 ± 1.0 | 9.0 ± 1.1 | 0.07 |
| Time playing (years) | 8.1 ± 3.6 |
| 60°/s | 180°/s | 300°/s | ||||||||
| Movements | Variables | Athletes | Non - athletes | p - value* | Athletes | Non - athletes | p - value* | Athletes | Non - athletes | p - value* |
| Mean/ SD | Mean/ SD | Mean/ SD | Mean/ SD | Mean/ SD | Mean/ SD | |||||
| DER | PT/Weight | 58.93 ± 2.65 | 44.55 ± 3.33 | <0,01 | 52.87 ± 2.57 | 40.45 ± 3.20 | <0,01 | 59.47 ± 4.21 | 47.68 ± 4.02 | <0,05 |
| Work | 222.7 ± 7.78 | 175.9 ± 9.97 | <0,01 | 188.8 ± 5.81 | 140.4 ± 9.51 | <0,01 | 329.7 ± 9.29 | 247.2 ± 14.2 | <0,01 | |
| Power | 29.77 ± 1.04 | 21.53 ± 1.29 | <0,01 | 58.73 ± 2.00 | 41.03 ± 3.26 | <0,01 | 68.47 ± 2.82 | 44.93 ± 3.55 | <0,01 | |
| NDER | PT/Weight | 55.51 ± 4.07 | 40.33 ± 2.05 | <0,01 | 49.85 ± 3.37 | 38.82 ± 2.62 | <0,01 | 56.13 ± 3.98 | 45.79 ± 3.33 | <0,05 |
| Work | 195.1 ± 12.1 | 154.7 ± 8.25 | <0,01 | 172.1 ± 10.6 | 130.6 ± 7.08 | <0,01 | 294.8 ± 16.3 | 228.8 ± 11.9 | <0,01 | |
| Power | 26.48 ± 1.75 | 19.32 ± 1.03 | <0,01 | 54.32 ± 3.98 | 38.27 ± 2.14 | <0,01 | 60.76 ± 4.50 | 40.63 ± 2.79 | <0,01 | |
| RID | PT/Weight | 83.87 ± 4.57 | 64.02 ± 4.47 | <0,01 | 75.97 ± 3.36 | 58.91 ± 3.61 | <0,01 | 78.99 ± 3.39 | 65.86 ± 3.62 | <0,01 |
| Work | 325.4 ± 12.8 | 270.5 ± 11.4 | <0,01 | 290.5 ± 14.1 | 223.9 ± 12.8 | <0,01 | 530.5 ± 22.0 | 412.4 ± 18.4 | <0,01 | |
| Power | 42.77 ± 1.82 | 32.36 ± 1.56 | <0,01 | 90.07 ± 4.50 | 61.07 ± 4.13 | <0,01 | 108.2 ± 5.86 | 72.59 ± 4.18 | <0,01 | |
| NDIR | PT/Weight | 78.82 ± 4.79 | 62.57 ± 4.35 | <0,01 | 71.11 ± 4.68 | 60.18 ± 4.01 | <0,01 | 74.28 ± 4.83 | 64.82 ± 4.14 | 0,29 |
| Work | 301.0 ± 17.1 | 253.1 ± 12.9 | <0,05 | 266.4 ± 17.7 | 229.0 ± 11.6 | <0,08 | 443.9 ± 42.0 | 393.5 ± 21.6 | 0,14 | |
| Power | 39.14 ± 2.56 | 31.24 ± 1.78 | <0,01 | 81.50 ± 6.53 | 64.82 ± 4.06 | <0,05 | 96.09 ± 8.67 | 70.74 ± 4.78 | <0,01 | |
Note: SD - Standard Deviation; PT - Peak Torque; * t test was used; boldface indicates statistical difference. DER - Dominant External Rotation; NDER - Nondominant External Rotation; DIR - Dominant Internal Rotation; NDIR - Nondominant Internal Rotation
Twelve athletes (66%) presented muscle imbalance on the dominant side, (6 with a predominance of ER and 6 of IR), and eleven athletes (61%) on the non - dominant side (7 with a predominance of ER and 4 of IR). Among non - athletes, 8 subjects (44%) presented with muscle imbalance on the dominant side (7 ER and 1 IR), while on the non - dominant side were found 12subjects (66%) (6 ER and 6 IR), although there was no statistical association between the occurrence of imbalance between ER and IR, dominance, or practice of sports. May be the values of table 3 show the ER/IR ratio of the dominant and non - dominant limbs, at all the velocities tested in both groups. There was no significant difference in the muscle imbalance between the groups. Table 1 shows the characteristics among the groups. The same table shows that there wasn’t any statistical difference between those characteristics in both groups.
| Velocities | Shoulder | Athletes | Non - athletes | p - value* |
| 60°/s | D | 0.71 ± 0.02 | 0.70 ± 0.03 | 0.8 |
| ND | 0.71 ± 0.03 | 0.67 ± 0.03 | 0.5 | |
| 180°/s | D | 0.69 ± 0.02 | 0.68 ± 0.03 | 0.7 |
| ND | 0.71 ± 0.03 | 0.65 ± 0.02 | 0.1 | |
| 300°/s | D | 0.74 ± 0.02 | 0.72 ± 0.04 | 0.6 |
| ND | 0.82 ± 0.07 | 0.72 ± 0.05 | 0.2 |
D - Dominant; ND - Non - Dominant
Figure 1 correlation between time (years) since injury and peak torque/weight (N.m/kg) of the dominant internal rotators of the athletes and non - athletes at 60°/s
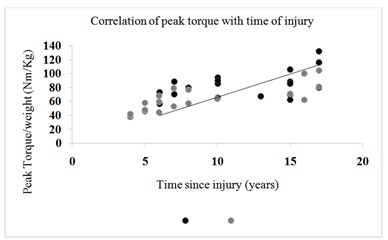
Figure 1: Correlation of peak torque with time of injury.
DISCUSSION
The results of the present study confirmed the hypothesis that values from isokinetic parameters for the shoulder rotator cuff from wheelchair basketball athletes were higher than the non - athletic group at all the tested angular velocities.
Loss of muscle mass in the acute phase after the spinal cord injury results in a catabolic state in which multiple intracellular signaling pathways stimulate the expression of specific genes. This results in protein degradation via proteasome and autophagy [17] and is accompanied by increased adipose tissue in the abdominal circumference and upper limbs [18], representing significant health risks after the spinal cord injury. Despite the similarity between groups concerning anthropometric parameters of height and weight, the difference of muscle performance variables may be caused by the differences in the proportion of body tissue distribution, with a higher percentage of muscle mass among those involved with regular sports activity [6].
Spinal cord injuries are associated with the accumulation of visceral fat tissue [6]. Spinal cord injured practitioners of sports activities develop greater muscle mass even having a body weight similar to another group [19]. When referring to wheelchair basketball, there is a component of aerobic predominance associated with the prolonged metabolic demand for the energy expenditure of dynamic acceleration, deceleration, and positional changes. Simultaneously, the anaerobic component is also present and is responsible for the short and intense bursts [20]. As a result, the practice of wheelchair basketball stimulates the production of proteins that lead to muscle hypertrophy and increase in strength [21], which explains the greater muscle performance of wheelchair basketball athletes.
The daily activities performed by wheelchair users demand frequent usage of both upper limbs simultaneously, either to push the wheelchair on the flat and inclined surface, to overcome an obstacle, to perform transferences, or to push up and prevent pressure ulcers [19]. Bilateral strengthening of upper limbs is one of the bases of the rehabilitation process and seeks to prepare the body to perform those tasks by inducing symmetrical hypertrophy of the shoulder girdle. However, despite the end of inpatient rehabilitation programs, repeated practice continues to strengthen upper limbs even more [11,19]. This may be the reason for the peak torque increase observed in the present sample over time since the injury occurred and for the symmetry between the dominant and the non - dominant limbs in both groups.
Although a muscular imbalance in the agonist and antagonist relationship of shoulder rotators in both groups was observed, there was no difference between athletes and non - athletes, which indicates that the wheelchair basketball did not influence external and internal rotation strength ratio. Other studies confirm the same results [6,11,14]. Biomechanical studies by surface electromyography and kinematic analysis showed high demands of muscular activities in the shoulder griddle due to the weight support of the individual in the wheelchair [7]. To prevent displacement of the humeral head and to keep it centralized in the glenoid cavity, a muscle balance of the internal and external rotators is necessary. Muscle overload can lead to their imbalance [7,22,23]. The shoulder joint is subject to a high load during the movement of the wheelchair, the peak torque generated in this movement can range from 300 to 1400 N, and the velocities from 0.4 to 1.5 m/s, with relatively high combined forces of the rotator cuff muscles, especially the sub scapular and infraspinatus muscles [24,25].
Studies show that practice of wheelchair basketball is associated with a high rate of shoulder injury, due to a muscle imbalance [21,26], which is also observed when the wheelchair athletes are compared to sedentary individuals [11,27,28,]. The study by Burnham et al., [11] investigated the role of imbalance in shoulder strength as a factor in the development of rotator cuff problems. The evaluation of the peak torque of abductors and adductors, and internal and external rotators of 19 paraplegic athletes and 20 healthy male individuals indicated that the weakness of rotators and adductors is associated with the rotator cuff impact syndrome in wheelchair athletes, but does not clarify the relationship between cause and consequence. In another study, 296 individuals with spinal cord injury who used the wheelchair for locomotion were divided into 103 patients playing overhead sport (at least 1 - 2 times per week) and 193 that did not practice any sports activity. Magnetic resonance imaging was performed on both shoulders. A torn rotator cuff was present in 75.7% of the patients in the sports group and 36.3% of the patients in the non - sports group [27].
On the other hand, Fullerton et al., [29] directly compared the occurrence and prevalence of shoulder pain in wheelchair athletes and non - athletes, by asking for the presence and duration of shoulder pain in 257 individuals. Wheelchair athletes were less likely to have shoulder pain than non - athletes. Also, those who participate in wheelchair sports enjoyed more years without shoulder pain than non - athletes. Thus, the study suggests that athletic activity has a protective effect on shoulder pain. Mulroy [10] showed that individuals who had decreased muscle strength and lower levels of physical activity before the onset of shoulder pain were more likely to develop it. Finally, Finley and Rodgers [30] have shown that wheelchair sports alone did not affect the risk of developing shoulder pain. Given this contradictory findings, there is still need for clarification of the participation of muscle imbalance in the development of musculoskeletal injuries and pain in shoulders of wheelchair - bound individuals.
One limitation of this study is that classification of the athlete’s functional capacity in court was not taken into account, and this may have interfered with the muscle strength. However, this would only apply to athletes and is very likely to be a consequence of muscle performance rather than a cause. The position used for the isokinetic evaluation may have interfered with the results, due to the compensation of adjacent muscles, even if they used stabilization straps. This position of the arm was considered the most resembling functional activities of daily living and sports performance. Another limiting factor was the possibility of the basketball athlete having better functioning before deciding to play basketball. This problem could have been remedied with a longitudinal study. Finally, body composition of the sample was not evaluated and might interfere with muscle performance. To overcome this problem, peak torque was corrected by body weight.
Loss of muscle mass in the acute phase after the spinal cord injury results in a catabolic state in which multiple intracellular signaling pathways stimulate the expression of specific genes. This results in protein degradation via proteasome and autophagy [17] and is accompanied by increased adipose tissue in the abdominal circumference and upper limbs [18], representing significant health risks after the spinal cord injury. Despite the similarity between groups concerning anthropometric parameters of height and weight, the difference of muscle performance variables may be caused by the differences in the proportion of body tissue distribution, with a higher percentage of muscle mass among those involved with regular sports activity [6].
Spinal cord injuries are associated with the accumulation of visceral fat tissue [6]. Spinal cord injured practitioners of sports activities develop greater muscle mass even having a body weight similar to another group [19]. When referring to wheelchair basketball, there is a component of aerobic predominance associated with the prolonged metabolic demand for the energy expenditure of dynamic acceleration, deceleration, and positional changes. Simultaneously, the anaerobic component is also present and is responsible for the short and intense bursts [20]. As a result, the practice of wheelchair basketball stimulates the production of proteins that lead to muscle hypertrophy and increase in strength [21], which explains the greater muscle performance of wheelchair basketball athletes.
The daily activities performed by wheelchair users demand frequent usage of both upper limbs simultaneously, either to push the wheelchair on the flat and inclined surface, to overcome an obstacle, to perform transferences, or to push up and prevent pressure ulcers [19]. Bilateral strengthening of upper limbs is one of the bases of the rehabilitation process and seeks to prepare the body to perform those tasks by inducing symmetrical hypertrophy of the shoulder girdle. However, despite the end of inpatient rehabilitation programs, repeated practice continues to strengthen upper limbs even more [11,19]. This may be the reason for the peak torque increase observed in the present sample over time since the injury occurred and for the symmetry between the dominant and the non - dominant limbs in both groups.
Although a muscular imbalance in the agonist and antagonist relationship of shoulder rotators in both groups was observed, there was no difference between athletes and non - athletes, which indicates that the wheelchair basketball did not influence external and internal rotation strength ratio. Other studies confirm the same results [6,11,14]. Biomechanical studies by surface electromyography and kinematic analysis showed high demands of muscular activities in the shoulder griddle due to the weight support of the individual in the wheelchair [7]. To prevent displacement of the humeral head and to keep it centralized in the glenoid cavity, a muscle balance of the internal and external rotators is necessary. Muscle overload can lead to their imbalance [7,22,23]. The shoulder joint is subject to a high load during the movement of the wheelchair, the peak torque generated in this movement can range from 300 to 1400 N, and the velocities from 0.4 to 1.5 m/s, with relatively high combined forces of the rotator cuff muscles, especially the sub scapular and infraspinatus muscles [24,25].
Studies show that practice of wheelchair basketball is associated with a high rate of shoulder injury, due to a muscle imbalance [21,26], which is also observed when the wheelchair athletes are compared to sedentary individuals [11,27,28,]. The study by Burnham et al., [11] investigated the role of imbalance in shoulder strength as a factor in the development of rotator cuff problems. The evaluation of the peak torque of abductors and adductors, and internal and external rotators of 19 paraplegic athletes and 20 healthy male individuals indicated that the weakness of rotators and adductors is associated with the rotator cuff impact syndrome in wheelchair athletes, but does not clarify the relationship between cause and consequence. In another study, 296 individuals with spinal cord injury who used the wheelchair for locomotion were divided into 103 patients playing overhead sport (at least 1 - 2 times per week) and 193 that did not practice any sports activity. Magnetic resonance imaging was performed on both shoulders. A torn rotator cuff was present in 75.7% of the patients in the sports group and 36.3% of the patients in the non - sports group [27].
On the other hand, Fullerton et al., [29] directly compared the occurrence and prevalence of shoulder pain in wheelchair athletes and non - athletes, by asking for the presence and duration of shoulder pain in 257 individuals. Wheelchair athletes were less likely to have shoulder pain than non - athletes. Also, those who participate in wheelchair sports enjoyed more years without shoulder pain than non - athletes. Thus, the study suggests that athletic activity has a protective effect on shoulder pain. Mulroy [10] showed that individuals who had decreased muscle strength and lower levels of physical activity before the onset of shoulder pain were more likely to develop it. Finally, Finley and Rodgers [30] have shown that wheelchair sports alone did not affect the risk of developing shoulder pain. Given this contradictory findings, there is still need for clarification of the participation of muscle imbalance in the development of musculoskeletal injuries and pain in shoulders of wheelchair - bound individuals.
One limitation of this study is that classification of the athlete’s functional capacity in court was not taken into account, and this may have interfered with the muscle strength. However, this would only apply to athletes and is very likely to be a consequence of muscle performance rather than a cause. The position used for the isokinetic evaluation may have interfered with the results, due to the compensation of adjacent muscles, even if they used stabilization straps. This position of the arm was considered the most resembling functional activities of daily living and sports performance. Another limiting factor was the possibility of the basketball athlete having better functioning before deciding to play basketball. This problem could have been remedied with a longitudinal study. Finally, body composition of the sample was not evaluated and might interfere with muscle performance. To overcome this problem, peak torque was corrected by body weight.
CONCLUSION
The practice of wheelchair basketball showed an influence over the shoulder muscles of those with traumatic spinal cord injury, since the athletes presented, bilaterally, higher values of functional performance (peak torque, work, and power), when compared to non - athletes. There was symmetry between the dominant and non - dominant limbs in both groups. Basketball athletes and non - athletes presented bilateral agonist and antagonist muscle imbalance of the shoulder rotator muscles. The correlation was found between the time of spinal cord injury and the peak torque for internal rotators at 60°/s in both groups. These data contribute to future work related to the isokinetic parameters of the shoulder rotators in wheelchair basketball athletes and non - athletes with spinal cord injury.
REFERENCES
- Ambrosio F, Boninger ML, Souza AL, Fitzgerald SG, Koontz KM, et al. (2005) Biomechanics and Strength of Manual Wheelchair Users. J Spinal Cord Med 28: 407-414.
- Cool AM, Witvrouw EE, Mahieu NN, Danneels LA (2005) Isokinetic Scapular Muscle Performance in Overhead Athletes With and Without Impingement Symptoms. J Athl Train 40: 104-110.
- Johnson MP, McClure PW, Karduna AR (2001) New method to assess scapular upward rotation in subjects with shoulder pathology. J Orthop Sports Phys Ther 31: 81-89.
- Kerr J, Borbas P, Meyer DC, Gerber C, Buitrago Téllez C, et al. (2015) Arthroscopic rotator cuff repair in the weight-bearing shoulder. J Shoulder Elbow Surg 24: 1894-1899.
- International Wheelchair Basketball Federation (2010) IWBF classification for wheelchair basketball. International Wheelchair Basketball Federation, Switzerland, UK.
- Inukaia Y, Takahashib K, Wang DH, Kira S (2006) Assessment of total and segmental body composition in spinal cord-injured athletes in Okayama prefecture of Japan. Acta Med Okayama 60: 99-106.
- Mulroy SJ, Hatchett P, Eberly VJ, Haubert LL, Conners S, et al. (2015) Shoulder Strength and Physical Activity Predictors of Shoulder Pain in People With Paraplegia From Spinal Injury: Prospective Cohort Study. Phys Ther 95: 1027-1038.
- Sisto SA, Dyson-Hdson T (2007) Dynamometry testing in spinal cord injury. J Rehabil Res Dev 44: 123-136.
- Mason BS, Lemstra M, Van der Woude LH, Vegter R, Goosey-Tolfrey VL (2015) Influence of wheel configuration on wheelchair basketball performance: wheel stiffness, tyre type and tyre orientation. Med Eng Phys 37: 392-399.
- Pellegrini A, Pegreffi F, Paladini P, Verdano MA, Ceccarelli F, et al. (2012) Prevalence of shoulder discomfort in paraplegic subjects. Acta Biomed 83: 177-182.
- Burnham RS, May L, Nelson E, Steadward R, Reid DC (1993) Shoulder pain in wheelchair athletes. The role of muscle imbalance. Am J Sports Med 21: 238-242.
- Gil-Agudo A, Mozos MSC, Ruiz B, del-Ama AJ, Pérez-Rizo E, et al. (2016) Shoulder kinetics and ultrasonography changes after performing a high-intensity task in spinal cord injury subjects and healthy controls. Spinal Cord 54: 277-282.
- Mccasland LD, Budiman-mak E, Weaver FM Adams E, Miskevics S (2006) Shoulder pain in the traumatically injured spinal cord patient: evaluation of risk factors and function. J Clin Rheumatol 12: 179-186.
- Edouard P, Samozino P, Julia M, Gleizes CS, Vanbiervliet W, et al. (2011) Reliability of isokinetic assessment of shoulder-rotator strength: a systematic review of the effect of position. J Sport Rehabil 20: 367-383.
- Ellenbecker TS, Mattalino AJ (1997) Concentric isokinetic shoulder internal and external rotation strength in professional baseball pitchers. J Orthop Sports Phys Ther 25: 323-328.
- Hughes RE, Johnson ME, O'Driscoll SW, An KN (1999) Normative values of agonist-antagonist shoulder strength ratios of adults aged 20 to 78 years. Arch Phys Med Rehabil 80: 1324-1326.
- Cohen S, Nathan JA, Goldberg AL (2015) Muscle wasting in disease: molecular mechanisms and promising therapies. Nat Rev Drug Discov 14: 58-74.
- Gorgey AS, Wells KM, Austin TL (2015) Adiposity and spinal cord injury. World J Orthop 6: 567-576.
- Gagnon D, Babineau AC, Champagne A, Desroches D, Aissaoui R (2014) Trunk and Shoulder Kinematic and Kinetic and Electromyographic Adaptations to Slope Increase during Motorized Treadmill Propulsion among Manual Wheelchair Users with a Spinal Cord Injury. BioMed Research International 2015.
- Coutts KD (1992) Dynamics of wheelchair basketball. Med Sci Sports Exerc 24: 231-234.
- Lai KM, Gonzalez M, Poueymirou WT, Kline WO, Na E, et al. (2004) Conditional activation of akt in adult skeletal muscle induces rapid hypertrophy. Mol Cell Biol 24: 9295-9304.
- Perry J, Gronley JK, Newsam CJ, Reyes ML, Mulroy SJ (1996) Electromyographic analysis of the shoulder muscles during depression transfers in subjects with low-level paraplegia. Arch Phys Med Rehabil 77: 350-355.
- Reyes ML, Gronley JK, Newsam CJ, Mulroy SJ, Perry J (1995) Electromyographic analysis of shoulder muscles of men with low-level paraplegia during a weight relief raise. Arch Phys Med Rehabil 76: 433-439.
- Arnet U, van Drongelen S, Scheel-Sailer A, van der Woude LH, Veeger DH (2012) Shoulder load during synchronous handcycling and handrim wheelchair propulsion in persons with paraplegia. J Rehabil Med 44: 222-228.
- Fokter SK, Cicak N, Skorja J (2003) Functional and Electromyographic Results After Open Rotator Cuff Repair. Clinical Orthopaedics & Related Research 415: 121-130.
- Lal S (1998) Premature degenerative shoulder changes in spinal cord injury patients. Spinal Cord 36: 186-189.
- Akbar M, Brunner M, Ewerbeck V, Wiedenhöfer B, Grieser T, et al. (2015) Do overhead sports increase risk for rotator cuff tears in wheelchair users? Arch Phys Med Rehabil 96: 484-488.
- Mulroy SJ, Farrokhi S, Newsam CJ, Perry J (2004) Effects of spinal cord injury level on the activity of shoulder muscles during wheelchair propulsion: an electromyographic study. Arch Phys Med Rehabil 85: 925-934.
- Fullerton HD, Borckardt JJ, Alfano AP (2003) Shoulder pain: a comparison of wheelchair athletes and nonathletic wheelchair users. Med Sci Sports Exerc 35: 1958-1961.
- Finley MA, Rodgers MM (2004) Prevalence and identification of shoulder pathology in athletic and nonathletic wheelchair users with shoulder pain: A pilot study. J Rehabil Res Dev 41: 395-402.
Citation: Freitas PS, Serenza FDS, Santana TS, Manoel LS, Riberto M (2017) Isokinetic analysis of rotator cuff musculature of sedentary wheelchair users and basketball athletes with spinal cord injury. J Phys Med Rehabil Disabil 3: 017.
Copyright: © 2017 Poliane Silva Freitas, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!