Long-Term Care for Older Adults in Rural China: Findings from the Recent Chinese Longitudinal Healthy Longevity Survey
*Corresponding Author(s):
Ye ZhangThe School Of Business, Nanjing University, 22 Hankou Road, Nanjing, China
Tel:+86 2583621233,
Email:zhangye@nju.edu.cn
Abstract
Population aging poses a significant challenge for rural China’s long-term care system. Based on a nationally representative elderly survey in 2018, this paper attempts to provide a recent profile of the demand for and supply of long-term care among the rural elderly. It shows that there was a substantial demand for LTC services in rural China, but many of the needs were unmet or not satisfactory. Informal home-based care still dominated the delivery of LTC services; meanwhile, community-based and institutional care played a trivial role. As for financing mechanisms, public LTC financing was at most minimal, and the vast majority of older rural people relied on out-of-pocket spending for their LTC services. Based on the findings, several policy recommendations are discussed.
Keywords
Long-term care; Older adults; Rural China
Introductiojn
The past decade has witnessed an accelerating population aging in China, especially in rural areas. According to the seventh population census, more than 190 million people in China were 65 and over in 2020, accounting for 13.6% of the total population. In particular, people who were 80 and older and were most likely to need Long-Term Care (LTC) amounted to more than 35 million. Due to the large-scale rural-to-urban migration of prime-aged workers, population aging is more pronounced in rural areas. Specifically, almost half of China’s older people lived in rural areas, taking up as high as 17.8% of the rural population relative to 11% in urban areas. Population aging means increasing demand for LTC services. One of the most pressing challenges is how to meet the increasing demand for LTC at an acceptable cost. In this paper, LTC refers to services for people who suffer from chronic illnesses or disabilities [1]. Compared with care services for people with other health conditions like acute or episodic illnesses, LTC typically lasts over prolonged periods and even until the end of the recipient’s life. It means LTC can be a significant burden for families in terms of money, time, and effort spent on caregiving. In this paper, LTC includes paid (formal) and unpaid (informal) services for the elderly who need assistance.
This paper focuses on LTC issues among the rural elderly. The rural area faces a much more significant LTC challenge. Traditionally, the rural elderly rely more on the family to provide LTC services for the lack of formal care arrangements. However, largely due to the shrinkage of the family size and rural-to-urban migration, more and more rural elders come to live alone or with their spouse, without children residing nearby (so-called “nest-empty elders”), which means they can count less and less on their children to provide necessary LTC. Under this circumstance, formal LTC services are supposed to emerge and prosper to fill the gap. However, restricted by factors such as the low-income level of rural residents, the shortage of the LTC workforce, and the geographically dispersed living style, private enterprises rarely find it attractive to deliver LTC in rural areas because of the narrow profit margin unless subsidized heavily by the government. Meanwhile, it is not unusual for government-sponsored public nursing homes in rural areas to encounter the problem of low occupancy rates, which can be partially attributed to traditional attitudes towards eldercare, partially due to the poor quality of LTC services.
One prerequisite to better cope with the urgent LTC challenge is acquiring up-to-date facts about LTC in rural China. For example, how many older adults need LTC services? Who are their primary caregivers? Are they satisfied with the LTC services they have received? How can they finance the paid assistance if incurring? This study aims to answer such questions by providing an overview of long-term care for rural elderly from both the demand and supply sides, drawing on a nationally representative survey dataset. We also attempt to identify potential problems and make relevant policy recommendations.
The paper proceeds as follows. Section 2 introduces the data. Section 3 summarizes the potential demand for LTC in rural China. Section 4 describes the supply side of LTC according to the setting where LTC is delivered. Section 5 introduces financing mechanisms for LTC services available in rural China. Section 6 gives some policy recommendations and concludes the paper.
Data
The data used in this paper is drawn from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The CLHLS has been conducted by the Center for Healthy Aging and Development Studies at Peking University in China and co-sponsored by the National Institute on Aging in the United States. It covers 22 out of 31 provinces (autonomous regions or municipalities) and hosts approximately 85 percent of the total population in mainland China. Half of the counties and cities in each sample province were randomly selected. The baseline wave was conducted in 1998, and 7 follow-up waves were conducted respectively in 2000, 2002, 2005, 2008/09, 2011/12, 2014, and 2018. The CLHLS primarily focused on the oldest-old elderly aged 80 and over in its first two waves, and it expanded to cover the elderly aged 60 and over since the 2002 wave.
The CLHLS collects extensive information about the interviewees and their families, including demographic characteristics, socioeconomic conditions, living arrangements, and health status. In particular, for interviewees who are disabled and need some LTC services, the CLHLS collects information about their primary caregivers, expenditures (if incurring), and their assessment of the services, making it possible to provide a profile of the LTC demand and supply among the rural elderly. This paper draws on the most recent 2018 wave of the CLHLS. The 2018 wave interviewed 15,777 older persons aged 65 and over, of which 7,041 lived in rural areas. As shown in table 1, after adjusting the sampling weights, 50.5 percent of interviewees were urban residents, 47.7 percent were male, 93.4 percent were of Han ethnicity, and 18.9 percent were 80 and over. These proportions are very close to those from the population census in 2020. The differences fall into 0.1~2.2 percentage points. Hence, our sample is nationally representative, and its summary statistics can well reflect the overall situation in rural China.
|
Variable |
(1) |
(2) |
(3) |
|
CLHLS 2018 |
Census 2020 |
Difference (1)-(2) |
|
|
Urban |
0.505 |
0.526 |
-0.022 |
|
Male |
0.477 |
0.465 |
0.012 |
|
Han ethnicity |
0.934 |
0.939 |
-0.005 |
|
Aged 80 and over |
0.189 |
0.188 |
0.001 |
Table 1: Summary statistics of key variables and comparison with census data.
Note: (1) Means of selected key variables are reported in the table; (2) Column (1) is computed based on the wave 2018 of the CLHLS, adjusting the sampling weights; column (2) is computed from the 2020 population census data.
The Demand For LTC Among The Rural Elderly
We start by describing the LTC demand among older adults in rural China. Since the need for LTC mainly derives from physical or cognitive disability, we turn to analyze disability situations among the rural elderly. We use respectively two indicators to measure physical and cognitive disability as follows.
Disabled ADLs: Physical disability is defined based on Activities of Daily Living (ADLs). The CLHLS questions about ADLs are based on international standards [2], adapted to the Chinese culture and social context, and well verified by carefully conducted pilot study tests [3,4]. Specifically, ADLs cover six routine tasks of life, including eating, dressing, moving, using the toilet, bathing, and continence. Disabled ADL is constructed as a binary variable that equals 0 if the respondent reported no restriction in all six daily activities and equals 1 otherwise.
Impaired MMSE: Cognitive disability is defined based on the Mini-Mental State Examination (MMSE). Following the widespread practice in the literature [5], MMSE is used to measure five areas of cognitive function of the elderly: orientation, reaction, calculation, recall, and language. The MMSE is a 24-question measure with a total score ranging from 0 to 30. Based on the MMSE score, we construct an indicator of whether the respondent has an MMSE score of less than 24, which is suggested in the literature as indicating cognitive impairment [5,6]. It is worth emphasizing that cognitive function is as essential as ADLs for the elderly to live independently [7].
As shown in figure 1, many of the rural elderly suffered physical or cognitive disabilities in 2018. Specifically, about 6% of people aged 65 and over had “disabled ADL,” meanwhile as high as 12.3% of them had a cognitive disability. If considering these two types of disabilities together, the physically or cognitively disabled elderly amounted to 15.5%. Furthermore, among the elderly aged 80 and older, the proportion with disabled ADLs rose to 16%, the proportion with impaired cognitive function rose sharply to 31.8%, and the proportion with a physical or cognitive disability jumped to 38%. To sum up, with the rapid population aging, there was a substantial proportion of the rural elderly that were disabled, which, in turn, means a massive demand for LTC, especially among the oldest old.
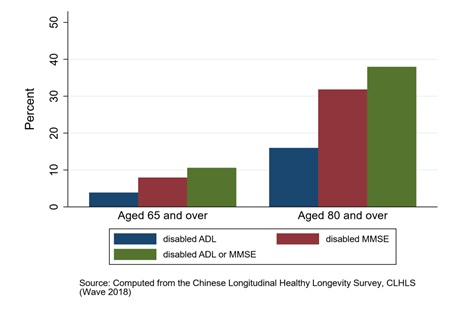 Figure 1: Fraction of older adults who were physically or cognitively disabled.
Figure 1: Fraction of older adults who were physically or cognitively disabled.
The Supply Of LTC Services For The Rural Elderly
Now, we turn to the supply side of LTC in rural China. According to the setting where it is delivered, LTC can be categorized into three types: home-based, community-based, and institutional care. As shown in figure 2, in 2018, almost all rural elderly (99.4%) were living at home; even among the elderly who were physically or cognitively disabled, only about 1.7% lived in nursing homes. Hence, home and community-based care overwhelmingly dominated LTC delivery in rural China.
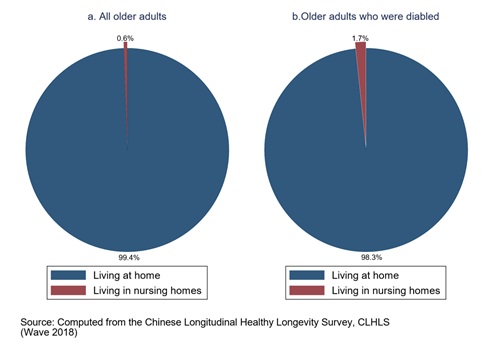 Figure 2: Living at home or in nursing homes?
Figure 2: Living at home or in nursing homes?
Home-based care
For the elderly who lived at home and suffered from disabled ADL and therefore needed some form of LTC, the CLHLS asked them about their primary caregivers and their assessment of the care services they received. The findings are as follows. First, the spouse, instead of children (including children, grandchildren, children-in-law and grandchildren-in-law), ranked as the number one LTC primary provider. Figure 3.a shows that almost one-third of elders reported their spouse as their primary caregiver, compared with one-quarter reporting their children. This finding is consistent with the fact that more and more older people become nest-empty due to the large-scale rural-to-urban migration of youngsters. It means the traditional pattern of elder care in rural China, “raising children to support the elderly,” was shaken to such an extent that it only plays the second important role.
Second, only 3.6% of the elderly who lived at home were mainly cared for by hired aides. This fact can be partially attributed to their low-income level and partly reflects the under development of the elder care market in rural China. Last but maybe the most striking finding is that almost 40% of the disabled elderly reported being unable to access LTC services when needed. The huge gap in the unmet needs reflected the unpleasant fact that there was indeed a loophole in the rural LTC system, which should be a priority of future policy intervention.
As for the quality of the LTC delivery, Figure 3.b shows that only about 45% of elders who received LTC services thought their needs were fully met; meanwhile, more than half thought it was so-so or unmet. This finding raises a concern about how to ensure LTC quality in the future.
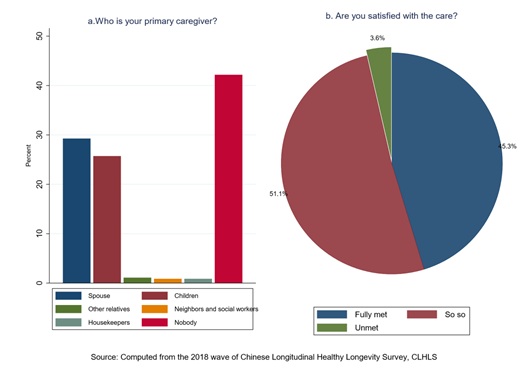 Figure 3: Primary caregivers when in need of LTC.
Figure 3: Primary caregivers when in need of LTC.
Community-based care
The CLHLS also asks interviewees about the services their community provides, including personal care, psychological counseling or comforting, sending doctors or delivering medicine to home, assistance with daily shopping, providing healthcare knowledge, and organizing social activities. As shown in figure 4, the community’s first three most frequently provided items were healthcare knowledge providing, sending doctors or delivering medicine to home, and organizing social activities, with a proportion of 41, 37 and 18%, respectively. It might be no surprise considering their low cost and occasionally occurring nature. As for the personal care services most relevant to LTC, only a few villages or communities (7.6%) provided them in 2018. A few more communities provided assistance in daily shopping and psychological counseling services, both with a proportion of barely above 10%. Overall, community-based care played a very limited role in delivering LTC services.
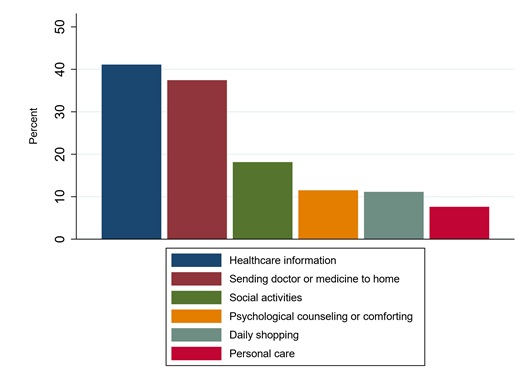 Figure 4: What services does your community provide?
Figure 4: What services does your community provide?
Institutional care
Institutional care, or nursing home care, played an at best ignorable role in providing LTC for the rural elderly until 2018. As shown in Figure 2.b, only 1.7% of the elderly who were disabled lived in nursing homes. This could be explained by multiple reasons, such as the backward eldercare industry, the low payment capacity of rural elders, or the traditional Chinese culture that regards children’s behavior of sending elderly parents to nursing homes as violating the virtue of filial piety. Besides, among the very few elders who lived in nursing homes, only 5.7% chose to live there voluntarily for access to more contact with other older persons; others had to live there due to no children or children’s care being unavailable (Figure 5).
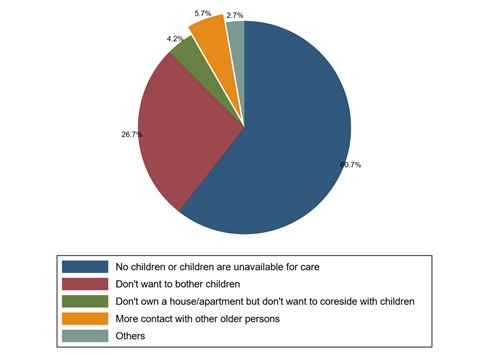 Figure 5: The reason for living in nursing homes.
Figure 5: The reason for living in nursing homes.
As for the expense of living in eldercare institutions, the average was about 1,800 yuan (Figure 6.a), far beyond the average income per capita per month among rural elders (i.e., 939 yuan) computed based on the study sample. Therefore, unaffordability was undoubtedly one of the most important reasons that hindered rural older people from living in nursing homes. Figure 6.b further shows that only 11% answered that the expense was paid by the collective or the government. Thus, the payment for institutional care mainly relies on out-of-pocket expenditures borne by children or themselves. This fact raises the question of LTC financing, which will be elaborated on in the next section.
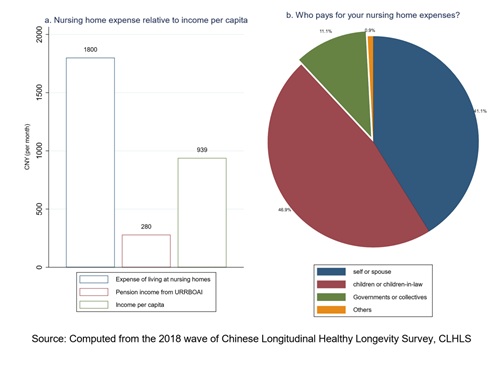 Figure 6: How to finance the LTC spending?
Figure 6: How to finance the LTC spending?
Financing Mechanisms For LTC In Rural China
Experience from western countries shows that insurance, especially social insurance, can be an efficient tool to protect people from unpredictable and catastrophic LTC expenditure. In rural China, several social insurance programs might help people to alleviate their LTC expenses.
Long-Term Care Insurance (LTCI): No specific social program aimed to provide LTC financing existed in China until 2016 when the central government launched the pilot of Long-Term Care Insurance (LTCI) in 15 cities and expanded to 49 cities since 2020. LTCI aims to assure older people of affordable LTC services. All the pilots are funded by the existing social health insurance programs-the Urban Employee Basic Medical Insurance (UEBMI) and the Urban-Rural Resident Basic Medical Insurance (URRBMI), by earmarking a particular percentage or a fixed amount per person from the existing risk pool of funds for LTC spending [8]. As a program still in progress, the eligibility and the benefits package vary from city to city. Evidence on its efficacy, sustainability, and impact on enrollees’ access to LTC, quality of the LTC, etc., is accumulating [9,10] and far from conclusive. Unfortunately, the LTCI pilots mainly focused on urban residents; rural residents have benefited little to date. When and how it will expand to cover all rural elderly should be prioritized on policymakers’ agenda.
Urban and Rural Resident Basic Medical Insurance (URRBMI): The URRBMI was built on integrating the New Rural Cooperative Medical Insurance (NRCMI) and the Urban Resident Basic Medical Insurance (URBMI) in 2016. The NRCMI was introduced in 2003, covering rural residents, and the URBMI was piloted in 2007, covering urban residents whom the UEBMI uncovers. Until 2018, there was 83% of rural elders enrolled in the URRBMI and 93% for any health insurance (Figure 7) in our elderly sample. Established as health insurance, the URRBMI aims to provide enrollees with financial protection from catastrophic medical expenditures. Therefore, it is no wonder that the URRBMI typically does not cover care services, with no mention of LTC. However, it does not mean there is no room for the URRBMI to play a part. First, the increasing complexity of care needs (e.g., multiple comorbidities) and their delivery requires integrating medical care and LTC services. For example, the home healthcare services, which require skilled care services and can be regarded as a mixture of medical and LTC care services, might be supported by the URRBMI more or less. On the other hand, the pilot LTCI and the URRBMI are financed by the same funds, which means, de facto, a competing relationship for resources between them. This fact also requires higher-level integration and coordination among them.
Urban and Rural Resident Basic Old-age Insurance (URRBOAI): In rural China, URROAI can date back to the New Rural Pension Scheme (NRPS), piloted in 2009 and aimed to solve or alleviate the pension problems of rural residents. In 2012, the NRPS merged with the former Urban Resident Basic Pension Scheme and integrated into a uniform system (i.e., URRBOAI). All rural residents aged 16+, not in education, and not covered by an urban residential pension scheme are eligible for the NRPS. After reaching 60 years of age, enrollees can claim a pension income consisting of two parts: one from the personal account accumulated from individual contributions and the other from the basic account subsidized by the central and local governments. According to the 2018 wave of the CLHLS, about 40% of the rural elderly aged 65+ enrolled in the URRBOAI and received an average monthly pension income of 280 yuan RMB (Figure 7). At first blush, the URRBOAI seems irrelevant to the LTC provision. However, it can support the elders with LTC needs indirectly by securing them a pension income, which can, in turn, help them to afford paid care services. Meanwhile, from international experience, the establishment of a formal pension scheme might alter the functioning of existing informal private care arrangements. A formal pension scheme might crowd out or displace intra-family elder care support, especially that provided by adult children [11,12]. Our research [13], based on the 2008 and 2011 waves of the CLHLS, also shows that after receiving pension income, the elderly become less dependent on their children as primary caregivers and switch to purchasing formal care services from the market.
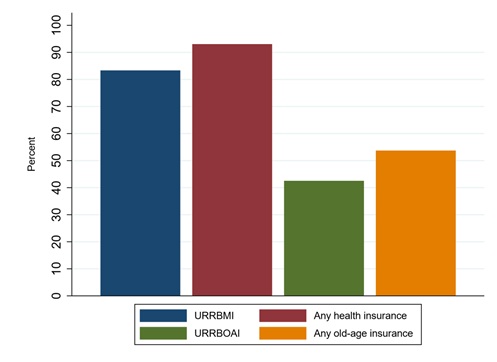 Figure 7: Participation rates in social programs.
Figure 7: Participation rates in social programs.
The wubao (“five guarantees”) system: As a part of the social welfare system in rural areas, the wubao system can date back to the 1950s. The target recipients are older adults who are childless or have no family [14]. Under this system, the government guarantees food, clothing, housing, medical care, and burial expenses. More than 5 million older people benefited from this system in 2014 [8]. As a form of care services enjoyed by the wubao elders, some of them can be accommodated by social welfare homes (jinglao yuan), that is, nursing homes owned and mostly operated by the government. Actually, the wubao system has long played the last resort role in providing LTC services for rural elders. Unfortunately, we notice that more than 40 percent of home-dwelling elders had nobody to count on when they needed help. Many of them were supposed to be covered by the wubao system. This means the wubao system might not work as well as it should, or its coverage might be expanded timely according to the new development of the rural aging situation.
In sum, though there seemed to be multiple mechanisms that could be used to finance the utilization of LTC services, it turns out that most of the rural elders still relied on out-of-pocket expenditures. In the future, more emphasis should be put on coordinating and integrating all the current mechanisms to make the best use of them.
Conclusion
This paper aims to provide a profile of the demand for and the supply of long-term care in rural China based on the most recent 2018 wave of the CLHLS. It shows that there was a substantial demand for LTC services; however, the supply seemed to fall far behind the demand, resulting in a huge gap of unmet or unsatisfied LTC needs. Informal home care from family members still dominated the LTC supply in rural China; community-based and institutional care played at best an ignorable role. Public LTC financing was minimal: older adults largely relied on their own out-of-pocket expenditures. Considering the unprecedented speed and large scale of population aging in rural China, policymakers have a long way to go to establish a safety net for LTC delivery.
As for policy implications, several points need to address. First, a sustainable financing system must be established to ensure that the elders have access to affordable LTC services. The LTCI is expected to expand to cover all rural residents who need LTC services in the near future. In areas where LTC facilities are relatively abundant, while LTCI has not been piloted, increasing subsidies through pension programs or expanding the coverage of health programs might be a good alternative. In addition, the government has to deliberately balance allocating resources among the four mechanisms mentioned before, based on more research and evidence on their relative efficacy.
Second, the development of the formal LTC industry is a pivotal factor in determining access to LTC services. Even with a sound financing system but no LTC facilities available conveniently, elders can still find it challenging to obtain necessary LTC services. Considering the vital role that nursing institutions play in providing LTC services in OECD countries [15], policies should be adopted to encourage the development of nursing institutions (especially private institutions) through subsidies or tax exemption measures. In recent years, the government has issued a series of policy directives to encourage the private sector to engage in LTC delivery, resulting in a proliferation of private LTC facilities in cities. However, how to stimulate them to provide LTC services in rural areas is still a question to be answered. Meanwhile, governments must focus more on enlarging and strengthening training programs to produce more qualified workers for LTC.
Third, we have noticed that communities-referring to villages or collectives in rural areas-only played a very limited part in providing long-term care services. This fact reflects that the role of the collective, as the bottom representative of the government and the policy practitioner and supplemental fund raiser of the wubao system, is substantially shattered. This is, inturn, mainly due to the weakening of the collective economy that can be traced back to rural reform in the 1980s. In the new era, how to strengthen and re-establish the collective as one main character to provide basic LTC services should receive more attention from policy makers.
JEL Classification
I11, I18; J14.
Acknowledgment
We thank Ke Shi, Yuankui Wang, Yingyue Xu, and Xu Yan for their assistance in data preparation and cleaning. We acknowledge financial support from the Humanity and Social Science Project of the Ministry of Education (Grant No. 17YJA790016) and the “Undergraduate Training Program for Innovation and Entrepreneurship” of Nanjing University (2022/2023). All errors are our own.
References
- Feder J, Komisar HL, Niefeld M (2000) Long-Term Care In The United States: An Overview. Health Affairs 19: 40-56.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW (1963) Studies of Illness in the Aged. The Index of ADL: A Standardized Measure of Biological And Psychosocial Function. JAMA 185: 914-919.
- Zeng Y, Vaupel JW, Zhenyu X, Chunyuan Z, Yuzhi L (2002) Sociodemographic and health profiles of the oldest old in china. Population and Development Review 28: 251-273.
- Gu D, Zeng Y (2004) Data assessment of the chinese longitudinal healthy longevity survey. In Determinants of healthy longevity of the oldest-old in china. Peking University Press, Beijing, China.
- Folstein MF, Folstein SE, McHugh PR (1975) “"Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: 189-198.
- Deb S, Braganza J (1999) Comparison of rating scales for the diagnosis of dementia in adults with down’s syndrome. J Intellect Disabil Res 43: 400-407.
- Greiner PA, Snowdon DA, Schmitt FA (1996) The loss of independence in activities of daily living: The role of low normal cognitive function in elderly nuns. Am J Public Health 86: 62-66.
- Feng Z, Glinskaya E, Chen H, Gong S, Qiu Y, et al. (2020) Long-term care system for older adults in china: Policy landscape, challenges, and future prospects. Lancet 396: 1362-1372.
- Feng J, Wang Z, Yu Y (2020) Does long-term care insurance reduce hospital utilization and medical expenditures? Evidence from china. Soc Sci Med 258: 113081.
- Lei X, Bai C, Hong J, Liu H (2022) Long-term care insurance and the well-being of older adults and their families: Evidence from china. Social Science & Medicine 296: 114745.
- Ettner SL (1994) The Effect of the Medicaid Home Care Benefit On long-Term Care Choices of the Elderly. Economic Inquiry 32: 103-127.
- Stabile M, Laporte A, Coyte PC (2006) Household responses to public home care programs. J Health Econ 25: 674-701.
- Cheng L, Liu H, Zhang Y, Zhao Z (2018) The heterogeneous impact of pension income on elderly living arrangements: Evidence from china’s new rural pension scheme. Journal of Population Economics 31: 155-192.
- Feng Z, Liu C, Guan X, Mor V (2012) China’s rapidly aging population creates policy challenges in shaping a viable long-term care system. Health Aff (Millwood) 31: 2764-2773.
- Norton EC (2000) Long-term care. Handbook of health economics 1: 955-994.
Citation: Cheng L, Zhang Y (2023) Long-Term Care for Older Adults in Rural China: Findings from the Recent Chinese Longitudinal Healthy Longevity Survey. J Gerontol Geriatr Med 9: 159.
Copyright: © 2023 Lingguo Cheng, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.