Lung and Thyroid Cancer Diagnosed During a Single Bronchoscopic Procedure
Abstract
Endobronchial Ultrasound-guided Transbronchial Needle Aspiration (EBUS-TBNA) is a minimally invasive sampling modality used in the evaluation of lung cancers with mediastinal and hilar/lobar lymphadenopathy. Its diagnostic utility in the evaluation of other mediastinal lesions is less clear.
We report a case of an 81-year-old male with concomitant lung and substernal thyroid lesions suspicious for malignancy on radiographic evaluation. Bronchoscopy with central EBUS-TBNA of the intrathoracic mass and electromagnetic navigation-guided nodule biopsy was performed without complication. To our knowledge, this is the first case of lung and thyroid cancer being diagnosed simultaneously during a single bronchoscopic procedure.
Keywords
EBUS-TBNA; Endobronchial ultrasound; Intrathoracic thyroid; Transbronchial needle aspiration
INTRODUCTION
EBUS-TBNA has emerged as the gold standard for the evaluation of mediastinal lesions due to its excellent diagnostic accuracy and safety profile [1-3]. Clinical utility has been well-established in the diagnosis and staging of lung cancers with mediastinal and hilar/lobar lymphadenopathy. However, its role in the evaluation of other intrathoracic lesions is less clear.
Ultrasound-guided Fine Needle Aspiration (US-FNA) biopsy is the sampling modality of choice in the evaluation of suspicious thyroid nodules/masses [4]. However, substernal thyroid lesions are not readily accessible via percutaneous approach, often necessitating diagnostic mediastinoscopy or surgical biopsy to exclude malignancy. Successful and safe intrathoracic thyroid sampling with EBUS-TBNA has been reported, potentially reducing the need for more invasive procedures [5]. This benefit is augmented in patients with suspicious lung and/or mediastinal lesions, allowing for concurrent evaluation of secondary cancer with a single procedure.
CASE DESCRIPTION
An 81-year-old male with a 45 pack-year smoking history was referred to our clinic for pulmonary nodules detected on workup for a 3-month history of unintentional weight loss. He did not complain of voice hoarseness, dysphagia, or dyspnea. There was no past history of malignancy or thyroid disease. Thoracic Computed Tomography (CT) revealed a 2 x 1.9 cm and 3.3 x 1.7 cm nodule with irregular margins in the superior and inferior lingular segments of the left lung, respectively, suspicious for malignancy. An enlarged and heterogeneous appearing 6 x 4 x 6.3 cm left thyroid lobe with mediastinal mass effect narrowing and rightward shift of the trachea was also noted (Figure 1). 18F-Flurodeoxyglycose Positron Emission Tomography (FDG-PET) follow-up demonstrated intense avid-FDG uptake of all lesions. Flexible bronchoscopy was performed under general anesthesia with central EBUS-TBNA of the mediastinal nodes and thyroid mass followed by electromagnetic navigational sampling of the lingular nodules. The trachea was noted to be significantly deviated to the right with saber-sheath narrowing from extraluminal compression (Figures 2a,2b). Total procedure time was 76 minutes without complications.

Figure 1: CT chest showing significantly enlarged left thyroid lobe with heterogenous appearance. There is resultant mild superior mediastinal extent as well as mass effect upon the trachea which is narrowed and displaced toward the right.
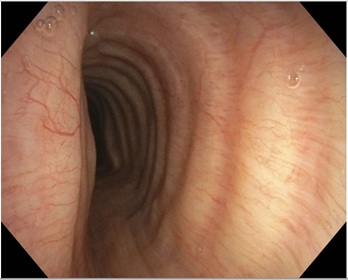
Figure 2a: Flexible bronchoscopy demonstrating rightward tracheal deviation with saber-sheath narrowing to 6 mm transverse luminal diameter.
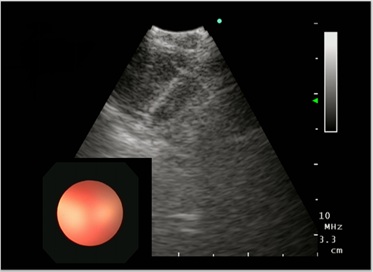
Figure 2b: Endobronchial ultrasound image of intrathoracic thyroid transbronchial needle aspiration.
Lung histopathology revealed TFT1 positive, thyroglobulin and p63 negative malignant cells consistent with primary lung adenocarcinoma. There were no malignant cells detected in the mediastinal lymph nodes. Thyroid cytology showed foci of atypical follicular epithelial cells with powdery chromatin pattern, occasional nuclear grooves and rare intranuclear inclusions suspicious for papillary thyroid cancer. The patient was referred to otolaryngology for left thyroid substernal lobectomy and potential total thyroidectomy.
DISCUSSION
It is estimated that up to 19% of substernal thyroid lesions are malignant [6]. Diagnostic sampling with US-FNA is challenging due the overlying sternum and anatomic relationship with several mediastinal structures. As a result, most cases require mediastinoscopy or surgical thoracotomy which may be poorly tolerated in patients with underlying cardiopulmonary disease [7].
EBUS-TBNA is a minimally invasive alternative with comparable diagnostic yield to mediastinoscopy for sampling of mediastinal lesions [8]. In the largest systematic literature review to date, 20 published cases of EBUS-TBNA thyroid aspiration have been reported to date [5]. Adequate aspirate was obtained in all cases with only one reported procedural complication. This has led to a growing body of literature supporting the role of EBUS-TBNA in the evaluation of substernal thyroid lesions with publication of protocolized procedures [9].
Our patient presented with lung and thyroid lesions both suspicious for malignancy, making bronchoscopy an ideal modality to acquire tissue samples from all lesions in a single procedure. The intrathoracic thyroid mass was successfully aspirated using EBUS-TBNA without procedural complications. Lung and thyroid cancer were diagnosed simultaneously, preventing the need for invasive diagnostic mediastinoscopy. This highlights the cost-effectiveness and safety of bronchoscopy as a multisampling modality. As the indications of EBUS-TBNA continue to expand, larger studies are needed to further validate diagnostic accuracy moving forward.
REFERENCES
- Yasufuku K, Chiyo M, Koh E, Moriya Y, Iyoda A, et al., (2005) Endobronchial ultrasound guided transbronchial needle aspiration for staging of lung cancer. Lung Cancer 50: 347-354.
- Chandra S, Nehra M, Agarwal D, Mohan A (2012) Diagnostic accuracy of endobronchial ultrasound-guided transbronchial needle biopsy in mediastinal lymphadenopathy: A systematic review and meta-analysis. Respir Care 57: 384-391.
- Vaidya PJ, Munavvar M, Leuppi JD, Mehta AC, Chhajed PN (2017) Endobronchial ultrasound-guided transbronchial needle aspiration: Safe as it sounds. Respirology 22: 1093-1101.
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, et al. (2016) 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26: 1-133.
- Madan K, Mittal S, Hadda V, Jain D, Mohan A, et al. (2016) Endobronchial ultrasound-guided transbronchial needle aspiration of thyroid: Report of two cases and systematic review of literature. Lung India 33: 682-687.
- Sahbaz NA, Tutal F, Aksakal N, Acar S, Aksu KI, et al. (2017) Cancer Frequency in Retrosternal Goiter. Am Surg 83: 1390-1393.
- Pace-Asciak P, Higgins K (2018) Review: The Management of an Intrathoracic Goiter. Medical Research Archives 6: 1-6.
- Czarnecka-Kujawa K, Yasufuku K (2017) The role of endobronchial ultrasound versus mediastinoscopy for non-small cell lung cancer. J Thorac Dis 9: 83-97.
- Kumar A, Mohan A, Dhillon SS, Harris K (2014) Substernal thyroid biopsy using endobronchial ultrasound-guided transbronchial needle aspiration. J Vis Exp 10: 51867.
Citation: Tosonian S, Thomas J, Soni S (2020) Lung and Thyroid Cancer Diagnosed During a Single Bronchoscopic Procedure. J Cytol Tissue Biol 7: 026.
Copyright: © 2020 Shawnt Tosonian, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.