Journal of Surgery Current Trends & Innovations Category: Clinical
Type: Research Article
Massive Ventral Hernia Repair: A Novel Technique with an Innovative Device
*Corresponding Author(s):
Luo YDepartment Of Surgery, College Of Medicine, Saskatoon, Canada
Tel:+1 3068441087,
Email:yil872@mail.usask.ca
Received Date: Nov 27, 2017
Accepted Date: May 26, 2017
Published Date: Dec 29, 2017
Abstract
To improve massive ventral hernia repair outcome, especially for those recurrent massive ventral hernia, we studied our novel technique with an innovative abdominal retractor. We designed the retractor, tested it in vitro and on animals. The feasibility, foldability and security were confirmed. Clinical massive ventral hernias were also repaired in the novel technique with satisfactory results. This innovative abdominal retractor has since been patented. Further research to optimize the flexibility, efficiency and biocompatibility in comparison with the traditional method is under process.
Keywords
Abdominal retractor; Innovative; Massive ventral hernia repair; Novel technique
INTRODUCTION
Massive ventral hernia happens up to 30% of the time following a laparotomy [1]. Some 100,000-150,000 ventral hernia cases were repaired annually in the United States. The repair of massive ventral hernia is frequently a challenge, with up to more than the 30% failure rate, in addition to complications, such as severe postoperative pain, infection, seroma, hematoma, and so on [2]. Currently, in clinic, we used a spatula (Figure 1) to prevent untoward injury to abdominal contents in our novel technique. However, the spatula had to be replaced along with each anchoring suture. Obviously, the procedure became inefficient and time consuming.
 Figure 1: Currently available spatula device used for the mesh application in the massive ventral hernia repair surgery.
Figure 1: Currently available spatula device used for the mesh application in the massive ventral hernia repair surgery.In order to overcome these challenges in massive ventral hernia repair, an innovative approach has been attempted.
We hypothesized that during mesh application in the massive ventral hernia repair, a novel easily applicable retractor that is flexible, foldable and puncture-proof can better facilitate the surgery as compared to the currently available spatula device (Figure 1). This study has been approved by the University of Saskatchewan Ethical Board (#20170063).
We hypothesized that during mesh application in the massive ventral hernia repair, a novel easily applicable retractor that is flexible, foldable and puncture-proof can better facilitate the surgery as compared to the currently available spatula device (Figure 1). This study has been approved by the University of Saskatchewan Ethical Board (#20170063).
MATERIALS AND METHODS
Design and production of the device
Firstly, we conceived the shape, size, and method of expansion of the device by designing a retractor composed of several layers of leaf-shaped paper and cardboard material. Secondly, a makeshift abdomen was created by placing an air-filled pillow in a small cardboard box. With a hard plastic sheet (Office Staples mat) placed between the air-filled bag and the lid, 42 puncture holes were made from the top using the suture passer. This experiment was performed twice to ensure that the selected plastic was puncture-proof. Thirdly, a novel retractor was finalized with 7 foldable hard plastic leaflets, joined together by a string on medial central end. Finally, the new retractor was tested on a mock pig abdominal hernia mesh repair surgery (n=2) as follows.
Abdominal surgery on pigs
Two healthy pigs (large white, 30-40kg, females) from Prairie Swine Center, Saskatoon, Saskatchewan, Canada, were sacrificed for a separate kidney procurement and ex vivo perfusion study (Protocol #416438) in the operating room of Veterinary Medical Center at the College of Veterinary Medicine, University of Saskatchewan. The retractor designed in the present study was tested when the abdominal wall was sewn back together. An appropriately sized flexible polythene plastic sheet (12 cm in diameter) was used in place of a mesh. We tested our retractor on both pigs regarding its manipulation (insertion, unfolding, refolding and retrieval), its protective reliability, and the time required in placement of a mesh.
CLINICAL CASE
A 56 year old female, BMI (body mass index) 42, with recurrent massive ventral after five repairs before including mesh repair and abdominal wall component separation reconstruction, came to the emergency department with persistent bowel obstruction for one week. She was treated conservatively with the nasal gastric tube and IV nutrition support. However, her symptoms were not relieved. CT scan showed complete bowel obstruction with definitive transitional site in small bowel incarcerated in the recurrent massive ventral hernia in the upper abdomen. The abdominal wall defect was about 20 cm. She was taken to the operating room, where she had laparotomy, mesh repair in our novel technique but with a spatula (Figure 2).
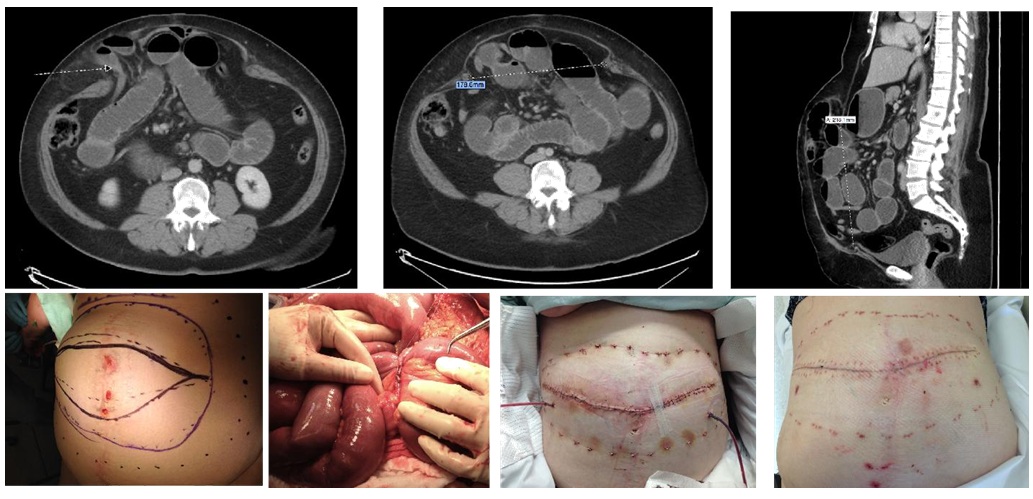 Figure 2: Clinical case. Top: CT scan showing bowel obstruction and recurrent massive ventral hernia. Bottom left two pictures: operative findings, the massive hernia and abdominal incision (lateral); adhesion band, causing complete obstruction (medial). Bottom right two pictures: early postoperative (medial), one month after the surgery (lateral).
Figure 2: Clinical case. Top: CT scan showing bowel obstruction and recurrent massive ventral hernia. Bottom left two pictures: operative findings, the massive hernia and abdominal incision (lateral); adhesion band, causing complete obstruction (medial). Bottom right two pictures: early postoperative (medial), one month after the surgery (lateral).RESULTS
Simple and innovative retractor design for use in abdominal hernia repairs
Our concept model was made from 8 layers of leaves in paper and cardboard (Figure 3). Appropriate size and shape, were reached together with unfolding and refolding capability as 9 cm × 12 cm elliptical leaflets, according to our further application in animal trial, to be protective over 15-20 cm in diameter intra-abdominal area. The strength of the plastic sheet against puncture due to the suture passer was tested on our makeshift abdomen. A total of 84 punctures were made, with no penetration, suggesting the plastic material (Office Staples mat) was very effective in protection (Figures 4 and 5). The next stage of our study involved making the device from the plastic material (Office Staples mat) and assembly. The final product consists of 7 leaflets of plastic material held together by a string in medial central side (Figure 6). The device was flexible yet strong and easy to fold and unfold. It could satisfactorily cover 15-20 cm intra-abdominal surgical area.
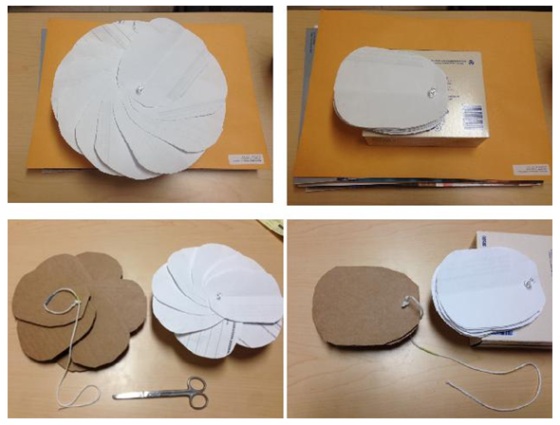
Figure 3: The initial concept model of the foldable leaf-shaped retractor made from the paper (upper), cardboard (lower left) as well as the paper (lower right).
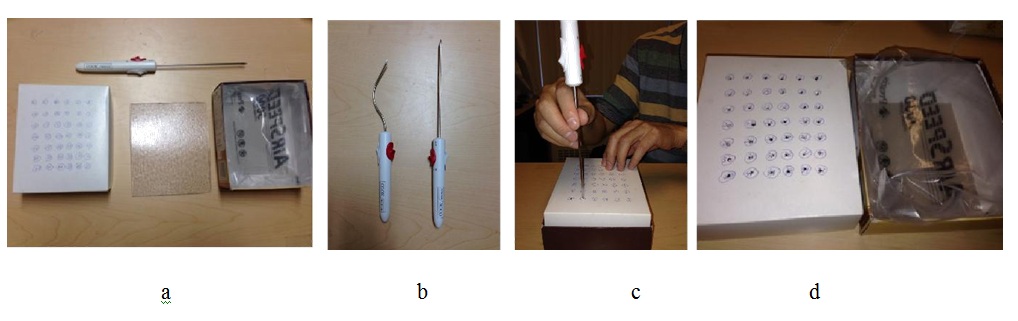 Figure 4: The setup of the makeshift abdomen, comprising of cardboard box (or lid) with an air pillow, designed to emulate the abdominal wall and contents and the test of the protective strength of the retractor material. (a) Retractor material cut to the appropriate size of the box and it will be placed between the lid and the air pillow; (b) Suture passers (Cook Medical Inc.); (c) A suture passer was used to puncture the cardboard box lid, using the makeshift abdomen with protective retractor material inside the cardboard box between the lid (representing abdominal wall) and a air pillow (representing abdominal contents); (d) The post-experimental puncture results, the intact air pillow and the lid with 42 puncture sites made by the suture passer, showing the retractor material was strong enough to protect against suture passer.
Figure 4: The setup of the makeshift abdomen, comprising of cardboard box (or lid) with an air pillow, designed to emulate the abdominal wall and contents and the test of the protective strength of the retractor material. (a) Retractor material cut to the appropriate size of the box and it will be placed between the lid and the air pillow; (b) Suture passers (Cook Medical Inc.); (c) A suture passer was used to puncture the cardboard box lid, using the makeshift abdomen with protective retractor material inside the cardboard box between the lid (representing abdominal wall) and a air pillow (representing abdominal contents); (d) The post-experimental puncture results, the intact air pillow and the lid with 42 puncture sites made by the suture passer, showing the retractor material was strong enough to protect against suture passer. Figure 5: Open view of the final design of the abdominal retractor consisting of 7 leaf-shaped sheets that spreads to cover the abdominal contents against the suture passer.
Figure 5: Open view of the final design of the abdominal retractor consisting of 7 leaf-shaped sheets that spreads to cover the abdominal contents against the suture passer.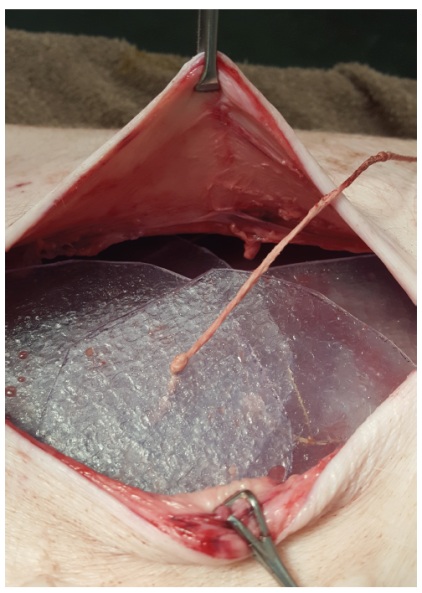 Figure 6: Pig abdominal surgery showing the retractor device unfolded inside abdominal cavity.
Figure 6: Pig abdominal surgery showing the retractor device unfolded inside abdominal cavity.A time-saving and protective retractor for abdominal surgery on pig model
With the device pictured as shown in figure 5, our experiment with two sacrificed pigs showed that the retractor provided ample protection with no injury to the abdominal contents from the suture passer (Figures 6 and 7). The surgeon noted that the device insertion into the abdomen required some manual manipulation to ensure that all areas of the abdomen were covered (Figure 6).
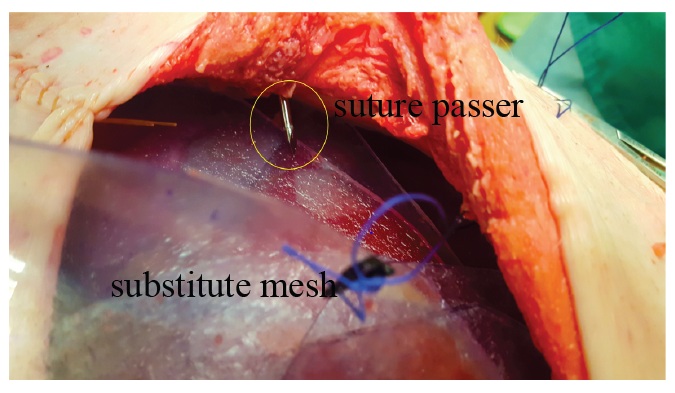 Figure 7: Pig abdominal surgery showing a suture passer traversing the abdominal wall and coming into contact with the retractor device. The retractor device successfully prevented the suture passer from injuring the underlying abdominal contents.
Figure 7: Pig abdominal surgery showing a suture passer traversing the abdominal wall and coming into contact with the retractor device. The retractor device successfully prevented the suture passer from injuring the underlying abdominal contents.The removal process on the other hand was quick and the compact size of the folded retractor proved beneficial (Figure 8). Only 26-28 minutes were needed to suture the mesh inside the abdomen. Roughly half the time was needed to do the same repair with currently available equipment (spatula) in the operating room.
 Figure 8: Conclusion of abdominal surgery. The sutures were tied from outside to anchor the mesh to the inside surface of the abdomen wall, after the retractor was removed.
Figure 8: Conclusion of abdominal surgery. The sutures were tied from outside to anchor the mesh to the inside surface of the abdomen wall, after the retractor was removed.CLINICAL CASE RESULT
During the surgery, an adhesion band causing complete bowel obstruction was found. It was divided. Extensive adhesions were lysed and the obstruction was released. The hernia defect, 21 cm ×18 cm was repaired with a 25 cm × 35 cm complex mesh using our new anchoring technique.
She recovered very well after the surgery. The follow-up 3 months showed that she was doing well, back to work, with no complications or recurrence (Figures 2 and 9).
She recovered very well after the surgery. The follow-up 3 months showed that she was doing well, back to work, with no complications or recurrence (Figures 2 and 9).

Figure 9: A different patient, 6 months after massive ventral hernia repair with a 27 cm × 34 cm complex mesh using our anchoring technique.
DISCUSSION
Massive ventral hernia happens commonly up to 30% after abdominal surgeries, especially after trauma laparotomy and multiple abdominal surgeries with postoperative incisional complications, such as infection, dehiscence, and so on [3]. These hernias often cause significant morbidity, leading to poor life quality and possible complication of bowel obstruction [2]. Repair of massive ventral hernia is frequently a challenge in general surgery, with up to more than a 30% failure rate, in addition to postoperative pain, incision complications, etc [2]. Every year, some 100,000-150,000 ventral hernia were repaired in the United States [4].
Over the last 20 years, tension-free repair of massive ventral hernia with mesh, especially by laparoscopy, becomes gradually popular with much better outcomes, such as less postoperative abdominal pain and a decreased recurrence rate close to 15% [2,3,5-10]. However, most research on massive ventral hernia repair is about modification of the existing approaches or surgical methods, including abdominal wall reconstruction. There was little research on surgical instruments or devices for this purpose, in particular, design of a retractor to facilitate this type of surgery.
Inlay mesh repair is one choice of surgical techniques, where the mesh is inserted and attached to inside surface of abdominal wall. Although the laparoscopic approach is to facilitate inlay mesh placement with less likelihood of infection, seroma or hematoma, it carries high rate of incidental enterotomy and usually takes longer surgical time [3]. In addition, very large ventral hernia, recurrent ventral hernia, incarcerated hernia and hernia with multiple past surgeries might be relative contraindicative for laparoscopic surgery [3]. On the other hand, open hernia repair usually needs to free the fascia muscular layer to facilitate the anchoring an inlay mesh and, thus creates a potential dead space between subcutaneous layer and fascia muscular layer. This approach leads to the shortcomings of open surgery: more postoperative pain, high rate of seroma, hematoma and mesh infection as well as longer patient stays in the hospital [3].
Our approach is to use an open technique but a laparoscopic instrument to speed up the surgery by not freeing the fascia muscular layer to omit the complications caused by the above mentioned dead space. After freeing the adhesions inside the abdomen, we repair the hernia by anchoring the inlay mesh with sutures across the whole abdominal wall with the help of laparoscopic suture passer. This technique has been used in clinical cases with good results. The patient hospital stay is shorter with little wound complications. However, incidental bowel perforation is a potential complication and although rare its consequence are devastating [1]. In order to prevent incidental injury to the intestines and other intra-abdominal organs intra-operatively, we usually have to use a spatula, which is relatively small, narrow and inadequate in providing complete protection to the intra-abdominal organs, including the intestines. We need to move and ensure the spatula stay precisely in place of every suture passer puncture, which not only slows down the surgery but is also less reliable. Therefore, we invented a new abdominal retractor, which is designed as being foldable and fan-shaped. It can protect all the intra-abdominal organs including the intestines from incidental suture passer injury.
Over the last 20 years, tension-free repair of massive ventral hernia with mesh, especially by laparoscopy, becomes gradually popular with much better outcomes, such as less postoperative abdominal pain and a decreased recurrence rate close to 15% [2,3,5-10]. However, most research on massive ventral hernia repair is about modification of the existing approaches or surgical methods, including abdominal wall reconstruction. There was little research on surgical instruments or devices for this purpose, in particular, design of a retractor to facilitate this type of surgery.
Inlay mesh repair is one choice of surgical techniques, where the mesh is inserted and attached to inside surface of abdominal wall. Although the laparoscopic approach is to facilitate inlay mesh placement with less likelihood of infection, seroma or hematoma, it carries high rate of incidental enterotomy and usually takes longer surgical time [3]. In addition, very large ventral hernia, recurrent ventral hernia, incarcerated hernia and hernia with multiple past surgeries might be relative contraindicative for laparoscopic surgery [3]. On the other hand, open hernia repair usually needs to free the fascia muscular layer to facilitate the anchoring an inlay mesh and, thus creates a potential dead space between subcutaneous layer and fascia muscular layer. This approach leads to the shortcomings of open surgery: more postoperative pain, high rate of seroma, hematoma and mesh infection as well as longer patient stays in the hospital [3].
Our approach is to use an open technique but a laparoscopic instrument to speed up the surgery by not freeing the fascia muscular layer to omit the complications caused by the above mentioned dead space. After freeing the adhesions inside the abdomen, we repair the hernia by anchoring the inlay mesh with sutures across the whole abdominal wall with the help of laparoscopic suture passer. This technique has been used in clinical cases with good results. The patient hospital stay is shorter with little wound complications. However, incidental bowel perforation is a potential complication and although rare its consequence are devastating [1]. In order to prevent incidental injury to the intestines and other intra-abdominal organs intra-operatively, we usually have to use a spatula, which is relatively small, narrow and inadequate in providing complete protection to the intra-abdominal organs, including the intestines. We need to move and ensure the spatula stay precisely in place of every suture passer puncture, which not only slows down the surgery but is also less reliable. Therefore, we invented a new abdominal retractor, which is designed as being foldable and fan-shaped. It can protect all the intra-abdominal organs including the intestines from incidental suture passer injury.
A novel retractor device for mesh application
This preliminary concept study involved innovative designing, creation, and testing of a surgical tool that will assist surgeons in mesh anchoring during open hernia repair surgery.
Our results demonstrated adequate protection, foldable design and easy application. There is evidence for further development of this simple useful device. It is important to note that our device does not require extra personnel to hold it in place, whereas the currently available spatula requires at least a two-person team. Reducing manpower, speeding up the surgery and prevention of complications will save taxpayers’ money on the health system and save patients from suffering.
Our study was still preliminary. Further investigations are warranted. Comparative studies with currently available spatula device on live animal are necessary for further evaluation of our novel retractor for safety, efficiency and biocompatibility [11,12]. Our concept design was still not thin and flexible enough making its application slightly cumbersome. A gear mechanism that turns the leaflets spreading to a pre-set perfect overlap would be ideal. Reusability of the device might be another consideration in our future study. Engineering optimization of leaflet shape, thickness, flexibility, number and biocompatibility is now undertaken.
Our results demonstrated adequate protection, foldable design and easy application. There is evidence for further development of this simple useful device. It is important to note that our device does not require extra personnel to hold it in place, whereas the currently available spatula requires at least a two-person team. Reducing manpower, speeding up the surgery and prevention of complications will save taxpayers’ money on the health system and save patients from suffering.
Our study was still preliminary. Further investigations are warranted. Comparative studies with currently available spatula device on live animal are necessary for further evaluation of our novel retractor for safety, efficiency and biocompatibility [11,12]. Our concept design was still not thin and flexible enough making its application slightly cumbersome. A gear mechanism that turns the leaflets spreading to a pre-set perfect overlap would be ideal. Reusability of the device might be another consideration in our future study. Engineering optimization of leaflet shape, thickness, flexibility, number and biocompatibility is now undertaken.
CONCLUSION
An innovative, foldable and reliable abdominal retractor useful for a new surgical technique in massive ventral hernia repair was proved in concept. Further optimization and verification are in process. This innovation has been patented.
ACKNOWLEDGEMENT
This research project was supported by College of Medicine Vice-Dean Summer Student Research Program 2016 and 2017, and Proof of Concept Fund from Innovation Enterprise, University of Saskatchewan 2017.
REFERENCES
- Kingsnorth A (2006) The management of incisional hernia. Ann R Coll Surg Engl 88: 252-260.
- Calisto JL, Kate V, Poggi L, Landmann A, Bender JS (2015) Laparoscopic Incisional Hernia Repair. Medscape.
- Read RC, Yoder G (1989) Recent trends in the management of incisional herniation. Arch Surg 124: 485-488.
- Leppaniemi A, Tukiainen E (2013) Reconstruction of complex abdominal wall defects. Scand J Surg 102: 14-19.
- Leppäniemi A, Tukiainen E (2012) Planned hernia repair and late abdominal wall reconstruction. World J Surg 36: 511-515.
- Andersen LPH, Klein M, Gogenur I, Rosenberg J (2009) Long-term recurrence and complication rates after incisional hernia repair with the open onlay technique. BMC Surg 9: 6.
- Vorst AL, Kaoutzanis C, Carbonell AM, Franz MG (2015) Evolution and advances in laparoscopic ventral and incisional hernia repair. World J Gastrointest Surg 7: 293-305.
- Rosen MJ (2009) Polyester-based mesh for ventral hernia repair: is it safe? Am J Surg 197: 353-359.
- Choi JJ, Palaniappa NC, Dallas KB, Rudich TB, Colon MJ, et al. (2012) Use of mesh during ventral hernia repair in clean-contaminated and contaminated cases: outcomes of 33,832 cases. Ann Surg 255: 176-180.
- Zhang Z, Bernard E, Luo Y, Wang H, Deng S, et al. (2000) Animal models in xenotransplantation. Expert Opin Investig Drugs 9: 2051-2068.
- Hannon JP, Bossone CA, Wade CE (1989) Normal physiological values for conscious pigs used in biomedical research. Letterman Army Institute of Research, Presidio of San Francisco, California.
Citation: Luo Y, Raj MT, Zhang WJ, Lim J, Xu Y, et al. (2017) Massive Ventral Hernia Repair: A Novel Technique with an Innovative Device. J Surg Curr Trend Innov 1: 003.
Copyright: © 2017 Luo Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!