Microneedle Radiofrequency Combined with Human Fibroblast Conditioned Media for Acne Scars and Skin Rejuvenation
*Corresponding Author(s):
Tanihaha EdwinDepartement Of Dermatology And Venerology, Iora Dermatology Clinic, Jakarta, Indonesia
Tel:+ 62 87776658096,
Email:edwintanihaha@yahoo.com
Abstract
Background: Acne vulgaris is one of the most common dermatology problems in the world. Acne scar can cause stress for sufferers. Microneedle Radiofrequency (MR) clinically has an effectiveness treating acne, acne scars and skin aging. MR acting as electrodes and directly deliver radiofrequency energy deep into the skin to induce new collagen production, dermal thickening and re epitelization.
Cases: Seventeen patients (12 acne scar and 5 aging patients, 25-50 years old, Fitzpatrick skin type III-IV) with acne scars and aging skin who received three sessions of microneedle radiofrequency treatment for 2 months at 3 weeks intervalper session.
Discussion: We use Goodman and Baron’s Global Acne Scarring System to assess the improvement of acne scars. It showed that by qualitative grading system from 12 patients (grade 3 and grade 4 acne scars), 58% patients showed 2 grade improvement, 33% showed1 grade improvement and 8.3% showed 3 grade improvement. Quantitative assessment showed that 58,3% of the patients had moderate improvement, 25% had good improvement and 16,6% had very good improvement. Global Aesthetic Improvement Scale (GAIS) are used to assess the improvement in skin texture, wrinkles graded by physician. It showed 60 % patients has 51 to 75% improvement and 40% patients has 26 to 50% improvement.
Conclusion: Microneedle radiofrequency is an effective therapy in treating moderate and severe acne scars and skin rejuvenation.
Keywords
Acne scars; Microneedle radiofrequency; Pigmentation; Skin texture; Wrinkles
INTRODUCTION
Acne is a chronic inflammatory disease of the pilosebaceus unit [1]. It is the most frequent skin lesion which affects >80% of world's population during some periods of their life and 85% of adolescents in the developed countries [2]. Sitohang S, Virgayanti P, et al. reported that the prevalence of acne vulgaris in Indonesia is not known with certainty, because surveillance for this disease is rarely carried out. CiptoMangunkusumo Hospital from 2008 to 2010 reported 6.612 acne vulgaris outpatient patients [3].
Scar is defined as “the fibrous tissue that replaces normal tissue destroyed by injury or disease” [4]. In acne, atrophic scars are much more common than hypertrophic scars. They most commonly involve the dermis, but can also involve the underlying fat. The phases of healing include inflammation (in the infrainfudibular region of the pilosebaceous structure), granulation tissue formation with fibroplasia and neovascularization, wound contracture and tissue remodeling [5]. Acne scars are associated with decreased self-confidence, including perception of decreases employability and embarrassement, and are negatively perceived by society [6].
Aging is a process perhaps best defined as decreased maximal function and reserve capacity in all body organs, resulting in an increased likelihood of disease and death. Like all other tissues, skin unavoidably ages, a processs than affect the function and appearance of the skin [7]. Skin aging is degenerative process whereby alteration from the passage of time (chronological/intrinsic aging) are superimposed with effect produced by environmental factors (e.g sun, heat, pollution, smoking) [8].
Microneedle Radiofrequency (MR) is widely used for acne scar without epidermal injury [9]. Insulated microneedle radiofrequency works by delivering radiofrequency energy only at the tip of the needles so can minimize epidermal disruption by only 5%, comparing with factional ablative laser around 10-70% [10]. Recent research shows the effectiveness of MR for skin tightening, wrinkle reduction and acne scaring [11].
METHODS
We did a case report to 17 patients (12 acne scar patients and 5 aging skin patients) with skin type III to IV. The inclusion criteria were healthy patients from 25 to 50 years old with depressed acne scars, aging skin patients who agreed and signed the informed consent letter. The exclusion criteria were patients who have blood disorder, taking blood thiner medicine, ginko biloba, vitamin e, history of keloids, pregnancy or breast feeding, skin allergy or dermatitis on the face, autoimmune disorder and refuse informed consent letter. We used microneedle radiofrequency device (ENSEMBLE, BISON Medical, Seoul, South Korea) with insulated needles to minimized the down time and deeper penetration.
The purpose of doing this case report was to improve the conditions of atrophic scars, skin texture, wrinkles using different grading system. All participants were asked to fill out an informed consent letter and take a photo session before and after each treatment.
Every patient received 3 treatments with 3 weeks interval between treatment.They were treated with certain parameters based on their facial condition. Topical anasthesia was applied to all participant around 20 minutes before treatment. Facial areas were treated with insulated needle using 1.75mm to 2.5mm penetration depth, power 40 W, out time 100ms.
Before we start the treatment, we applied serum (QT cell, S.THEPHARM, Co.,Ltd, Seoul, South Korea) that contain Human Fibroblast Conditioned Media (hDF-CM) in the skin target area, then did microneedle radiofrequency treatment and apply the serum again. After treatment we applied antibiotic cream and soothing cream all over the treated area. We evaluate the degree of the acne scar improvement using Goodman and Baron’s quantitative and qualitative acne scar grading system (Table 1, 2a & 2b).
|
Grade |
Level of Disease |
Characteristic |
Examples |
|
1 |
Macular disease |
Erythematous, hyper or hypopigmrnted flat marks visible to patient or observer irrespective of distance |
Erythematous, hyper or hypopigmented flat marks |
|
2 |
Mild disease |
Mild atrophy or hypertrophy that may not be obvious at social distances of 50cm or greater and may be covered adequately by make up or the normal shadow of shaved beard hair in males or normal body hair if extrafacial |
Mild rolling, small soft papular |
|
3 |
Moderate disease |
Moderate atrophic or hypertropic scarring that is obvious at social distances of 50cm or greater and is not covered easily by make up or the normal shadow of shaved beard hair but is still able to be flattened by manual stretching of the skin |
More significant rolling, shadow “boxscar’, mild to moderate hypertrophic or opular scars |
|
4 |
Severe disease |
Severe atrophic or hypertropic scarring that is obvious at social distances of 50cm or greater and is not covered easily by make up or the normal shadow of shaved beard hair in males or bidy hair (if extrafacial is not able to be flattened by manual stretching of the skin |
Punch out atrophic (deep “box scar”), “ice pick”, bridges and tunnels, gross atrophy, dystrophic scars significant hypertrophy or keloid |
Table 1: Goodman and Baron’s qualitative acne scar grading system [12,13].
|
Grade or Type |
Number of Lesions 1 (1-10) |
Number of Lesions 2 (11-20) |
Number of Lesions 3 (>20) |
|
Milder scarring (1point each) Macular erythematous pigmented Mildly atrophic dish like Moderate scarring (2 point each) Moderate atrophic, dish like Punched out with shallow bases small cars (<5mm) Shallow but broad atrophic areas Severe scarring (3 points each) Punched out with deep but normal bases, small scars (<5mm) Punched out with deep but abnormal bases, small scars (<5mm) Linear or troughed dermal scarring Deep, broad atrophic areas Hyperplastic Popular scars Keloidal/hypertrophic scars |
1 points
2 points
3 points
2 points Area < 5mm 6 points
|
2 points
4 points
6 points
4 points Area 5-20 mm2 12 points |
3 points
6 points
9 points
6 points Area > 20 cm2 18 points |
Table 2: (a) Goodman and Baron’s quantitative scar grading system [12,13].
|
Grade |
Improvement status |
|
0-5 5-10 10-15 >15 |
Minimal reduction in GSGS scores Moderate reduction in GSGS scores Good reduction in GSGS scores Very good reduction in GSGS scores |
Table 2: (b) Assessment of improvement using Goodman and Baron’s quantitative acne scar grading system [12,13].
Beside that acne scar grading system, the attending physician also evaluated the degree of improvement in skin texture, wrinkles and pigmentation, according to the Global Aesthetic Improvement Scale (GAIS):
0=No Improvement
1=≤25% mild improvement
2=26–50% moderate improvement
3=51–75% good improvement
4=76–100% excellent improvement
DISCUSSION
Acne scar therapy is still a challenge in various medical literature. Several therapy modalities are widely used in in the treatment of atrophic scars, such as peels (chemical peels and tca peels), dermabrasion, laser, microneedle, microneedle radiofrequency, derma filler, and surgery [14,15].
Aging skin occurs naturally and affects the quality of epidermis and dermis layer of the skin. In aging skin there is an increase in matrix metalloproteinase levels which causes a decrease in collagen and elastin skin [16].
Microneedle radiofrequency device has been widely used for the treatment of various skin disorders, such as wrinkles, atropich scars, acne vulgaris, and roscasea. It has a thermotherapy mechanism, spesifically the ability to reduce the activity of the sebaceous glands through a thermal stimulation [17].
Microneedle radiofrequency releases thermal energy in the dermis layer, so thereby preventing damage to the epidermis. The radiofrequency energy stimulates the formation of collagen and growth factors in the skin, resulting in dermal thickening [18]. Moreover, it has a lower downtime than ablative laser in treating acne scars [19]. Radiofrequency has a chromophore dependent properties, so it can be applied to all skin types and has less side effect of pigmentation than laser [20]. The microneedle itself also has another function as various drug delivery agent to penetrate through the skin barrier and bring the drug directly into the dermis [21].
RESULTS
All participants completed 3 treatment session at 3 week intervals. Most patients have various scar acne problem, such as ice pick, rolling scar, and box scar. Beside that, they also had acne vulgaris, and aging skin condition like wrinkles, dull skin and deep nasolabial fold. Microneedle radiofrequency can improve the appearance of scar acne, acne vulgaris, skit texture in aging skin.
The physician combine microneedle radiofrequency treatment with human fibroblast conditioned media which can help to release growth factors to stimulate angiogenesis, modulate inflammation, collagen formation and promote wound healing process.
The assessment of acne scar improvement using Goodman and Baron’s quantitative scale are listed in table 3. Participant with grade 4 acne scar, 7 participants showed improvement by 2 grade (70%), 2 participants showed improvement by 1 grade (20%), and 1 participants showed by 3 grade (10%). In participants who had grade 3 acne scars, 2 participants (100%) improved by 2 grade. Based on the assessment the improvement of acne scar from Goodman and Baron’s quantitative grading system, we found 58,3% of participants had a moderate improvement, 25% had a good improvement and 16,6% had a very good improvement. The assessment of acne scar improvement using Goodman and Baron’s qualitative scale, from 12 participants, 10 participants had grade 4 and 2 participants had grade 2.
We assessed the improvement in skin texture, and wrinkles using Global Aesthetic Improvement Scale (GAIS) and obtained 51-75% improvement in 60% participants and 26 to 50% improvement in 40% participants.
This therapy has varied pain relief and can be tolerated by all participants. All participants reported mild erythema for 2 to 3 days pasca treatment (Figures 1-6).
|
Previous to Treatment Grade of Acne Scar |
No of Patients |
Post Treatment Reduction of Scars by 3 Grades (%) |
Post treatment Reduction of Scars by 2 Grades (%) |
Post Treatment Reduction of Scars by 1 Grades (%) |
|
Grade 3 Grade 4 |
2 10 |
0 (0) 1 (10%) |
1 (100%) 7 (70%) |
0 (0) 2 (20%) |
Table 3: Physician assessment response based on Goodman and Baron’s qualitative acne scar grading.
 Figure 1: (a) Grade 4 acne scars, (b) Significant improvement in acne scars after 3x treatment (grade 4 to grade 2).
Figure 1: (a) Grade 4 acne scars, (b) Significant improvement in acne scars after 3x treatment (grade 4 to grade 2).
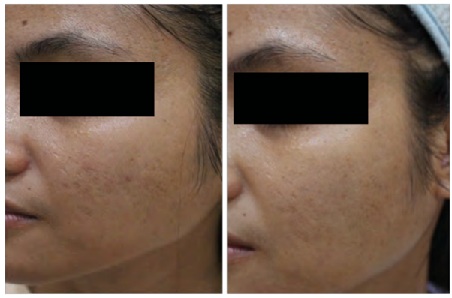 Figure 2: (a) Grade 4 acne scars, (b) Significant improvement in acne scars after 3 treatment (grade 4 to grad1).
Figure 2: (a) Grade 4 acne scars, (b) Significant improvement in acne scars after 3 treatment (grade 4 to grad1).
 Figure 3: (a) Grade 4 acne scars, (b) Significant improvement in acne vulgaris and acne scars after 3x treatment (grade 4 to grade 3).
Figure 3: (a) Grade 4 acne scars, (b) Significant improvement in acne vulgaris and acne scars after 3x treatment (grade 4 to grade 3).
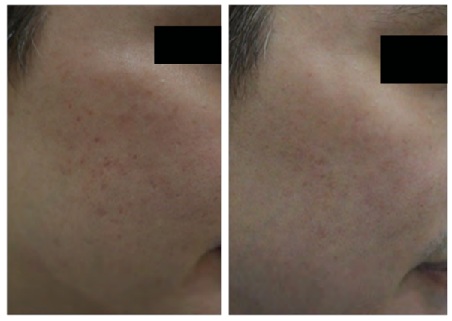 Figure 4: (a) Grade 3 acne scars, (b) Significant improvement in acne scars after 3x treatment (grade 3 to grade.
Figure 4: (a) Grade 3 acne scars, (b) Significant improvement in acne scars after 3x treatment (grade 3 to grade.
 Figure 5: (a) Before treatment, (b) After treatment, the treatment has shown a significant improvement in nasolabial lines, skin texture, and acne scars.
Figure 5: (a) Before treatment, (b) After treatment, the treatment has shown a significant improvement in nasolabial lines, skin texture, and acne scars.
 Figure 6. (a) Before treatment, (b) After treatment the treatment has shown a significant improvement in lines, wrinkles, nasolabial lines, skin texture and has a skin lightening effect and deep lines.
Figure 6. (a) Before treatment, (b) After treatment the treatment has shown a significant improvement in lines, wrinkles, nasolabial lines, skin texture and has a skin lightening effect and deep lines.
CONCLUSION
In addition to microneedle radiofrequency function in delivering drugs right into the dermis layer, release the growth factors and stimulate collagen formation, MR also has a higher level of presicion than laser, because it can be adjusted according to the depth of skin layer we need.
Combination between microneedle radiofrequency with human fibroblast conditioned media into scar acne and aging skin will enhance the satisfactory result. MR can be considered as an effective therapeutic option in the case of acne scar, and skin rejuvenation with minimal downtime and satisfactory result.
REFERENCES
- Brown BC, McKenna SP, Siddhi K, McGrouther DA, Bayat A (2018) The hidden cost of skin scars: quality of life after skin scarring. J PlastReconstr Aesthetic Surg 61: 1049-1058.
- Ibrahim NK, Nagadi SA, Idrees HJ, Alghanemi LG, Essa RI, et al. (2019) Acne vulgaris: Prevalence, predictors, and factors influencing quality of life of female medical students at King Abdulaziz University, Jeddah. Journal of Dermatology and Dermatologic surgery 23: 7-12
- Micali G, Lacarrubba F, et al. (2019) Classification of acne scars: clinical and instrumental evaluation. Acne scars classification and treatment, 2nd Page no: 1
- Veraldi S, barbareschi M (2010) Pathophysiology of acne scars. Acne scars classification and treatment,1st edition. Page no: 8-10
- Parnell LKS (2018) Itching for knowledge about wound and scar pruritus. Wounds 30: 17-36.
- Finch CE, Tanzi R (1997) Genetics of aging. Science 278: 407-411.
- Chung J, Cho S, et al (2004) Why does the skin age. Photoaging, 1st Page no: 1
- Hamer MA, Luba MP, Ikram MA, Laven JS, et al. (2017) Lifestyle and physiological factors associayed with facial wrinkling in men and women. J Invest Derm 137: 1692-1699.
- Hruza GJ, Taub AF, Collier SL, Mulholland RS (2009) Skin rejuvenation and wrinkle reduction usding a fractional radiofrequency system. Journal of Drugs in Dermatology 8: 259-265.
- Elawar A, Dahan S (2018) Non-insulated fractional microneedle radiofrequency treatment with smooth motor insertion for reduction of depressed acne scars, pore size and skin texture improvement. J Clin Aesthet Dermatol 11: 41-44.
- Hantash BM, Renton B, Berkowitz RL, Stridde BC, Newman J (2009) Pilot clinical study of a novel minimally invasive bipolar microneedle radiofrequency device. Lasers Surg Med 41: 87-95.
- Goodman GJ, Baron JA (2006) Post acne scarring: A qualitative global scarring grading system. Dermatol Surg 32: 1458-1466.
- Goodman GJ, Baron JA (2006) Postacne scarring--A quantitative global scarring grading system. J Cosmet Dermatol 5: 48-52.
- Saeed M, Elethawi A, Ali Elethawi, Al-Ani Z, Abdullah R (2016) Application of fractional microneedling radiofrequency and autologous platelet rich plasma in managing facial acne scars. British Journal of Medicine and Medical Research 14: 1-18.
- Aldag C, Teixeira D, Leventhal PS (2016) Skin rejuvenation using cosmetic products containing growth factors, cytokines and matrikines: a review of the literature. Clinical, Cosmetic and Investigational Dermatology 9: 411-419.
- Ruiz-Esparza J, Gomez JB (2003) Nonablative radiofrequency for active acne vulgaris: the use of deep dermal heat in the treatment of moderate to severe active acne vulgaris (thermotherapy): a report of 22 patients. Dermatol Surg 29: 333–339.
- Chien A (2018) Retinoids in Acne Management: review of current understanding, future considerations and focus on topical treatments. J Drugs Dermatol 17: 51-56.
- Kesty K, Goldberg D (2020) Radiofrequency microneedling for acne, acne scars and more. Dermatological reviews 1: 33-37.
- Dayan E, Chia C, Burns AJ, Theodorou SJ (2019) Adjustable dept fractional radiofrequency combined with bipolar radiofrequency: a minimally invasive combination treatment for skin laxity. Aesthetic Surgery Journal 39: 112-119.
- Singh A, Yadav S (2016) microneedling: advances and widening horizons. Indian Dermatology Online Journal 7: 244-254.
Citation: Edwin T, Hidajat D (2020) Microneedle Radiofrequency Combined with Human Fibroblast Conditioned Media for Acne Scars and Skin Rejuvenation. J Clin Dermatol Ther 6: 056.
Copyright: © 2020 Tanihaha Edwin, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.