Neglected Torticollis: Is it too Late for Surgical Treatment
*Corresponding Author(s):
Bee-See GohDepartment Of Otorhinolaryngology Head And Neck Surgery, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia
Tel:+60391456045,
Fax:+60391456675
Email:beesee@ppukm.ukm.edu.my; irenegbs@yahoo.com
Abstract
Congenital torticollis is the third most common musculoskeletal disorder in neonates after congenital hip dysplasia and club foot. Neglected congenital torticollis is defined when patient’s condition remains the same and intervention initiated after age of five-year-old. Neglected congenital torticollis however, can be successfully treated with surgery and physiotherapy. We present a case series involving three children (age range from 5 to 11-year-old), who were unsuccessfully treated with physiotherapy during neonatal period and lost to follow-up. We treated them with functional release of sternocleidomastoid (Z-plasty) and post-operative physiotherapy. All of them achieved good outcomes after 2 to 3 months post operation, indicating surgical intervention despite late presentation still carries a favourable outcome. This also improved the confidence level and self-esteem of the children in the society.
Keywords
Congenital torticollis; Neglected torticollis; Sternocleidomastoid muscle release; Torticollis
Introduction
Congenital torticollis or known as twisted neck has neither gender, nor right to left predilection [1]. The prevalence ranges from 0.3 to 3.92% in infants [2,3] documented that from total of 10% infants, 92.6% (98 infants) had isolated congenital muscular torticollis, while others are associated with either hip dysplasia (3.8%), brachial plexus palsy (1.9%), and metatarsus adduct us (1.9%) [1]. In some cases, congenital torticollis can be associated with plagiocephaly and facial asymmetry [3].
Case Report
Case 1
A 5-year-old girl, born full term assisted delivery with birth weight 3.0kg. Antenatal period was uneventful, with no history of intensive care unit admission or trauma. Post-natal, her neck was tilted to the right. She underwent physiotherapy until the age of 2 years old, and before lost to follow-up. Otherwise, there were no neck compression symptoms and was able to take orally well. Her parents sought treatment from otorhinolaryngology team at our centre at the age of 5 years old. Clinical examination showed the head tilted to the right with firm, shortened sternocleidomastoid muscle and inability to tilt to the left. Ultrasound of the neck showed entire length of right sternocleidomastoid muscle was echogenic from proximal to distal end with normal echo structure of muscle. Anteroposterior diameter of the muscle was slightly thicker, measuring 0.8cm, compared to the contralateral muscle 0.7cm. There was no focal lesion seen on the right sternocleidomastoid muscle, or the surrounding muscle. The left cervical structure was normal. Diagnosis of right torticollis secondary to fibrous sternocleidomastoid.
Case 2
An 8-year-old girl was born term via vacuumed assisted delivery, with birth weight 2.6kg. There was no history of intubation or ICU admission. Post-natal, there was limited neck movement and her head tilted to the right. She had undergone physiotherapy, subsequently lost to follow up. Her parents sought treatment again at the age of 7 years upon initiation of primary school. Orthopaedic team initial assessment led to MRI, showing evidence of right sternomastoid muscle fibrosis with atlantoaxial rotatory fixation type 2. CT neck excluded atlantoaxial rotatory fixation or subluxation.
Case 3
An 11-year-old girl, was born full term with birth weight of 2.67 kg and had normal antenatal and postnatal period. Her head was tilted to the right since the age of 3-month-old. It was not with any neck pain, neck spasm, stiffness or neck swelling. She was first referred to orthopaedic team and was on physiotherapy, before lost to follow up few years later. Her parents sought treatment again at age 11 years old. Clinically, her head tilted involuntarily to the right and she was unable to tilt the head to the left. There was a prominent and shorten right sternocleidomastoid muscle as compared to the left sternocleidomastoid muscle. There were no palpable neck nodes or neck swelling.
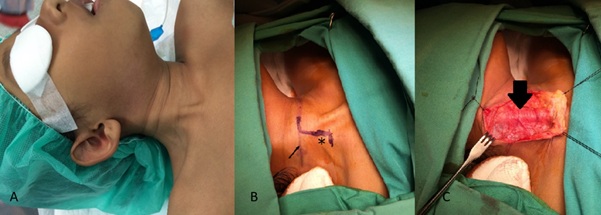 Figure 1: (A) Positioning of the patient; (B) Incision side; (black arrow) Horizontal skin incision at the level of cricoid cartilage. (*) Reverse Z incision at sternocleidomastoid (SCM), i.e. sternal head of the SCM was then divided using harmonic scalpel as far as the incision and the clavicular head was divided 1 cm from its insertion. The proximal end of the clavicular head was transposed to the distal end of sternal head of SCM; (C) Show fibrous and tight SCM muscle (black arrow).
Figure 1: (A) Positioning of the patient; (B) Incision side; (black arrow) Horizontal skin incision at the level of cricoid cartilage. (*) Reverse Z incision at sternocleidomastoid (SCM), i.e. sternal head of the SCM was then divided using harmonic scalpel as far as the incision and the clavicular head was divided 1 cm from its insertion. The proximal end of the clavicular head was transposed to the distal end of sternal head of SCM; (C) Show fibrous and tight SCM muscle (black arrow).
All patients underwent functional sternocleidomastoid Z-plasty (Figure 1). Post operatively, they were put on soft collar and underwent physiotherapy. All three patients had almost full range of neck movement during follow up 3 and 6 months (Figure 2)
 Figure 2: (A) Head position before operation; (B)Head position after 3 months post operation.
Figure 2: (A) Head position before operation; (B)Head position after 3 months post operation.
Discussion
The third most common congenital musculoskeletal anomalies in neonate is congenital torticollis, after hip dysplasia and clubfoot [3,4]. Torticollis or also known as twisted neck is defined as idiopathic condition that caused fibrosis or contracture on the unilateral sternocleidomastoid. This result in shortening of the sternocleidomastoid muscle, ipsilateral tilt and contralateral rotation of the face and chin [5]. It may be caused by trauma or ischemic insult that leads to fibrosis of sternocleidomastoid muscle [6]. The recommended initial treatment for congenital torticollis is physiotherapy (i.e. manual stretching and strengthening exercise [2]. An average of 54% to 97% was successfully treated with physiotherapy alone [2,7]. However, surgery is indicated if the head tilt persistently, limit lateral bending more than 15-degree, limit passive rotation and parents’ poor satisfaction. Surgery is usually performed at the age of 1 to 4 year old [8-10]. If a patient presents at the age of 5 years old or older, it is considered as a neglected congenital torticollis. The earliest age that had undergone surgery was 4 months old [6]. Most of the authors agree that early treatment will have better prognosis result [2,3,7,8]. All of three of our cases were on physiotherapy during infancy period. However, due to unsatisfactory result, parents were defaulted follow up and only seek treatment at the age of 5, 7 and 11 years old. There were 2 types of surgical treatment, either endoscopic or open surgery. Endoscopic released of sternocleidomastoid muscle below great auricular nerve documented at the age between 4 months till 2.5 years ( mean age 12 months old) [6]. To the authors’ knowledge, there was no report on endoscopic released procedure in the literature done for neglected congenital muscular torticollis.
For open technique, during 1980s, tenotomy was performed, but if adequate released was not achieved after tenotomy, the sternocleidomastoid is resected. Post operatively patient was put under neck split for 6-8 weeks and report a successful result [9] studied patients between age 10 to 19 years old with neglected congenital torticollis. They had undergone bipolar released of superior and inferior head and lengthening of the sternal head and by Z-plasty in all cases. Post operatively, all patients were put on head halter traction and physiotherapy. The study documented that only 2 out of 14 patients had poor outcomes [10] used unipolar and bipolar released without Z-plasty or muscle resection in a retrospective study. Post operatively the patients were put under halter traction and neck-stretching exercised. This technique of surgery depicted 89% had good to excellent result [11].
In the present case series, all patients underwent open surgery with Z-plasty released of the affected sternocleidomastoid that followed by regular neck physiotherapy for a few months. The results were satisfactory for the patients and parents. The neck condition improved after 2 to 6 months post operation and now 7 months to 2 years.
Conclusion
The present case series of neglected congenital torticollis depicted good outcomes following Z-plasty released of the abnormal sternocleidomastoid. Torticollis in childhood need to be addressed early. However surgical intervention in late presentation still carries a favourable outcome. Regardless, treatment aim is for full restoration of sternocleidomastoid function, permit head stabilization symmetrically and for pleasing aesthetics.
Ethical Approval
Not applicable.
Consent for Publication
Consent taken from all parents. All authors consented to publication.
Competing Interest
Not applicable
Funding
Not applicable
References
- Amaral MD, Cadilha RPBS, Rocha JAGM, Silva AIG, Parada F, et al. (2019) Congenital muscular torticollis: where are we today? A retrospective analysis at a tertiary hospital. Porto Biomed 4: 36.
- Cheng JC, Wong MW, Tang SP, Chen TM, Shum SL, et al. (2001) Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants. A prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am 83: 679-687.
- Min KJ, Ahn AR, Park EJ, Yim SY (2016) Effectiveness of Surgical Release in Patients With Neglected Congenital Muscular Torticollis According to Age at the Time of Surgery. Ann Rehabil Med 40: 34-42.
- Hahn HM, Cook KH, Lee J, Park DH, Park MC, et al. (2017) Use of Acellular Dermal Matrix in Treatment of Congenital Muscular Torticollis in Patients Over Eight Years of Age. J Craniofac Surg 28: 610-615.
- Gundrathi J, Cunha B, Mendez MD (2019) Congenital Torticollis, StatPearls Publishing: Treasure Island (FL).
- Burstein FD (2004) Long-term experience with endoscopic surgical treatment for congenital muscular torticollis in infants and children: a review of 85 cases. Plast Reconstr Surg 114: 491-493.
- Cheng JC, Au AW (1994) Infantile torticollis: a review of 624 cases. J Pediatr Orthop 14: 802-808.
- Lee KS, Chung EJ, Lee BH (2017) A comparison of outcomes of asymmetry in infants with congenital muscular torticollis according to age upon starting treatment. J Phys Ther Sci 29: 543-547.
- Tse P, Cheng J, Chow Y, Leung PC (1987) Surgery for neglected congenital torticollis. Acta Orthop Scand 58: 270-272.
- Sudesh P, Bali K, Mootha AK, Dhillon MS (2010) Results of bipolar release in the treatment of congenital muscular torticolis in patients older than 10 years of age. J Child Orthop 4: 227-232.
- Lim KS, Shim JS, Lee YS (2014) Is sternocleidomastoid muscle release effective in adults with neglected congenital muscular torticollis? Clin Orthop Relat Res 472: 1271-1278.
Citation: Bee-See Goh, Abdul-Aziz SSJ and Baki MM (2021) Neglected Torticollis: Is it too Late for Surgical Treatment. J Otolaryng Head Neck Surg 7: 55
Copyright: © 2020 Abdul-Aziz SSJ, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.