Osteopathic Treatment in Adult Patients Whit Hemoglobinopathies: A Coort of Study for Pain Evaluation and Quality of Life
*Corresponding Author(s):
Florinda FracchiollaMeyer Pediatric Hospital, Viale Pieraccini, 24, 50139 Florence, Italy
Tel:+39347195897,
Email:florindafracchiolla@hotmail.it
Abstract
Background: WHO estimates 180 million Hemoglobinopathies individuals worldwide, 7244 in Italy. Iron overload from transfusion therapy causes severe organic complications.
Objective: To evaluate the use of OMT, on the cohort of adult patients to assess pain and QoL.
Methods: Patients enrolled received a 30' OMT, once a week for 2 weeks, every 15 days for three weeks. VAS administered for pain measurement and SF36 for QoL, Before-After OMT. The convenience sampling with 10 enrolled subjects. The Pediatric Ethics Committee approved.
Results: Eight subjects enrolled. At the first detection, the mean pain reported 7 SD+-2.39, at the last detection of the after-OMT, it was 0.38 SD+-0.52.
The VAS difference between the first treatment and the second was 4.75 (P<0.0002), and 6.63 after the 5th (P<0.0001). For the QoL, we highlight average 88.6 SD+-14.26; 97.6 SD+-15.16, at the end of the treatment, P=0.43.
Conclusion: The study highlights the usefulness of OMT in the treatment of osteoarticular pain. For QoL, the improvement is not statistically significant.
The results we obtained highlight the efficacy of OMT in adults with BTM, especially in pain reduction, positively influencing QoL. An increase in the sample and an RCT study would be useful.
Keywords
Hemoglobinopathies; Osteopathic manipulative treatment; Pain; Thalassemia; Quality of life
Introduction
Thalassemic syndromes are a heterogeneous group of anemias of an autosomal recessive hereditary nature, caused by mutations affecting the genes of the protein chains of hemoglobin.
Beta Thalassemia (BT) is characterized by the deficit or total absence of the synthesis of beta-globin chains, which encodes the Hemoglobin Protein (Hb). Beta Thalassemia Mayor (BTM) or Cooley disease, is the homozygous form of BT and is associated with microlitic, hypochromic anemia and splenomegaly, due to dyseritropoiesis and hemolysis [1].
The World Health Organization (WHO) has estimated the presence in Europe, Africa and Asia of about 180 million microcitemic individuals, of whom 40% are healthy carriers of BT [2]. In Italy it is estimated that there are almost 2.5 million healthy carriers, that is, people who carry the genetic defect, who do not exhibit symptoms [3]: in particular, 7000 cases have been recorded [4] with a prevalence that reaches 15-20% in some Regions (Sicily, Sardinia) and in specific territories (for example Po Delta) [5].
As reported by the Rare Diseases Observatory, there are different types of thalassemia: in Africa, alpha thalassemia is more widespread (reduced synthesis of alpha chains), while in the Mediterranean basin beta (more reduced synthesis of beta chains) is more widespread, called also Mediterranean Anemia [6].
In the VI Congress of the Italian Thalassemia and Hemoglobinopathies Society (SITE), specialists defined thalassemia as an "emerging disease". From the census conducted between 2008 and 2010 in the 134 Italian centers, which deal with thalassemia, 7244 sufferers, with an increasing trend due to the presence of immigrants from areas of the globe where the pathology is endemic [7].
The onset of the disease occurs between 6 and 24 months of life and presents with severe anemia, which requires systemic transfusions to keep the Hb at the level of 90-100 g / l, so as to allow carrying out the normal physiology of the organism [8]. However, the transfusion of concentrated Red Blood Cells (RBC) is the cause of a progressive iron overload which, if not removed, leads to serious complications of various organs (mainly the heart, liver and endocrine glands) [9]. The treatment of BTM involves periodic transfusion RBC, generally every two to three weeks, and treatment with ferro-chelating drugs, such as: Deferoxamine, Deferiprone, and finally Deferasirox, available in Italy since 2007, which provides for a single daily administration with demonstrated ferrochelation in all the organs involved.
In thalassemia patients there are numerous musculoskeletal and osteoarticular problems: splanchnocranium enlargement, spinal deformity, scoliosis, compression of peripheral nerves, spontaneous fractures, loss of bone mass, analgesic contractures, myalgias, etc.
While the side of the disease, that is the etiopathogenetic component of the disease with its possible complex therapies, is extremely studied, the person's experience and Quality of Life (QoL) is less investigated. The most popular sources of information and dedicated websites deal precisely and precisely with the mechanics of the disease and its therapy, but do not take into consideration the psychological, emotional, social, relational, affective, working and economic aspects of the thalassemic patient. The side of illness - that is, living with disease - can only be investigated by listening to the voices of those who experience the disease and treatments firsthand, to understand what their true basic needs are, beyond the limits intrinsic data from the disease, and how partially they can be satisfied [10]. In southern Iran, a cross-sectional study on the usefulness of complementary medicines in thalassemia patients in Shiraz has recently been published, through the use of natural herbal products to help patients reduce serum ferritin and iron load in patients [11].
In December 2015, a report entitled 'The Value for the person with BTM was released by the SITE; a project to analyze the social cost and the tools to live with the disease, which analyzes emotional, emotional and lived aspects, both from the patient and the caregivers' point of view, highlighting the complexity of the disease and the goals achieved [12].
Currently in high development countries people with thalassemia have a life expectancy and quality standards of the same similar to the healthy population, provided that they can access an adequate treatment regime. It is important to underline that integration with other professional figures has also led to significant progress in understanding pathology and treatment.
From the analysis of the literature, Thalassemia is a disease that is not very well studied and discussed, especially in some areas, such as nursing and even less, from an osteopathic point of view [13-14]. At the moment our territory does not yet have numerous specialist centers for the diagnosis and treatment of these patients, as the pathology itself is not very widespread and, precisely for this reason, it has proved difficult to face a study that reaches conclusions today clinical and therapeutic aspects of maximum certainty [15].
The birth of scientific societies such as SITE, have the aim of being able to fill these shortcomings present in the scientific world, through the publication of evidence of efficacy in support of assistance to patients suffering from a pathology with such high dependence. At the pharmacological level, many progresses have been made, but the priorities linked to the general state of health of the thalassemic patient, due both to its clinical situation and to the complications related to the type of treatment, still remain very high; among which osteo-articular pain caused by ectopic extra-medullary localization factors, arthrosis, arthritis from iron accumulation and osteoporosis-osteopenia from endocrinopathies [16].
The Meyer pediatric hospital in Florence, within the Pediatric Cancer and Stem Cell Transplant department, offers a clinical care pathway for patients suffering from thalassemia and Hemoglobinopathies. To date, there is a cohort of adult patients who report functional musculoskeletal limitations, with a consequent reduction in daily life activities and an increase in painful perception.
In order to address these aspects within the treatment path, the Osteopathic Manipulative Treatment (OMT) was recently introduced, enriching the multi-professional team of the osteopath. Osteopathy is based on the consideration of the person as a unit, or the whole of the body, mind and spirit; and on the ability of the 'body' system to make corrections, restoring balances, through the mechanisms of self-regulation, physiologically already present within it. Great importance is attached to the relationship between structure and function, two interdependent aspects [17]. Osteopathy uses the 'manipulative touch' to support the patient's health [17]. Touch plays a crucial role in relationship in both children and adults [18]. The empathic relationship with the patient is an essential condition for the success of osteopathic treatments [19]. Also Touch has an affective and symbolic function [20]. It is a highly complex sensory modality. Perception of stimuli varies from person to person based on life experiences and genetic and epigenetic factors [21]. Human touch seems to attenuate the physiological response to stress in children and decreases the expression of cortisol [22], regulating oxytocin, vasopressin [23], and vagal tone [24]. Studies show that touch, used in osteopathic techniques, is an expression of compassion, skill and competence [25]; probably encourages the DNA to behave differently, promoting mitochondrial biogenesis, with possible effects on the reduction of the inflammatory state [26], on the attenuation of the sensation of stress and perceived pain, on the improvement of mood and increase in self-confidence and towards others, with cascading effects on pro-social behaviors [27].
Osteopathic manipulative touch is targeted and reflexive, palpation has an impact on the musculoskeletal, immune, endocrine, neuropsychic systems [28,29]. Through the touch, stimulation is produced on the skin, which represents the first delimiting structure of the body, the interface between inside and outside. It is the first physical barrier to potentially negative stimuli (antigens), with an efficient immune system capable of organizing a specific immune response by dendritic cells [30]. The immune response is a normally systemic response that involves system sectors located in areas of the body. It is not possible to separate the immune cell from its context and from the influences exerted by the environment in which it operates, consisting of vessels, nerves, cells, substances and tissue structures, whose messages are represented by hormones, neurotransmitters, cytokines and other substances biologically active, being a system in constant motion [30]. Recent studies show how osteopathic manipulation can act on the connective fascia, which, having its own contractility potential [31], can produce effects in musculoskeletal dynamics [32].
Inflammation also represents a complex phenomenon, which starting from stimuli of an infectious, chemical, physical, immune, psychic nature involves vessels, tissues, organs and systems, and is regulated by intrinsic mechanisms, by cytokines, chemokines and immune cells, nervous and endocrine circuits [29]. The noxious, irritating, thermal stimulus reaches the underlying nerve endings (the C fibers) which release chemicals, substance P, a neuropeptide that transmits the pain signal in the brain, but is not only a pain messenger, as it has a role of activator of the inflammatory response by immune cells present in the dermis [31,33].
For some years, in chronic, post-traumatic stress-induced, affective diseases, the phenomenon of interception has been observed, as a multidimensional construct, together with the phenomenon of sensitization, defined as an amplification response, having a neurological basis following of repeated stimuli, and the possible applications of manual therapies [34].
Touch-based manual practices, especially osteopathy, seem to produce anti-inflammatory and hyper-parasympathetic effects, offering an alternative method [...] to modify temporary or permanent sensitization states for the entire duration of the interaction with the treatment of peripheral tissues.
This is supposed to produce a biological and neurological cascade of events that modify the interoceptive processes, interrupting the vicious circle of a low-threshold and persistent inflammatory condition [34,35].
The study of this approach, applied in these pathologies, however, represents a gray area, worthy of investigation.
The goal of our research was to measure, through an observational survey, the possible effects of osteopathic manipulative therapy on the pre-post treatment pain trend, and the QoL of patients suffering from anemia, treated at the center Florentine, especially on those affected by BTM.
Materials And Methods
The study was based on measuring the possible effects of OMT, administered once a week for the first two weeks, every 15 days for the three consecutive weeks, with duration of 30 minutes. The detection was carried out through the use of validated evaluation scales, such as: Visual Analogic Scale (VAS) for Before-After treatment pain and the 36-item short-form SF-as a questionnaire to measure the quality of patient's life [11], Before-After osteopathic treatment cycle.
For convenience, given the rarity of the pathology and the small size of the sample, the entire population affected by Thalassemia Mayor and Intermedia has been included, being treated at the DH Oncohaematological service of the Meyer Pediatric Hospital in Florence. Twenty-five of the thirty-five subjects in charge of the aforementioned department were enrolled on the basis of the following inclusion criteria: Presence of osteo-articular pain, osteoporosis, functional limitation, declared unsatisfactory QoL; and exclusion: tumor pathologies, suspected bleeding condition, damage to the integrity of a bone, and / or tendon, and / or ligament, and / or joint, suspected malformation or cerebral hemorrhage, psychiatric diseases or mental limitations, the lack of knowledge of Italian language, minors and teenagers aged 25 or under. A sample size of ten enrolled units had been established, based on the prevalence of beta thalassemia in the Tuscany region. However, our evaluation was performed on a sample of only eight units, due to the logistical difficulties that occurred during the study period (Figure 1).
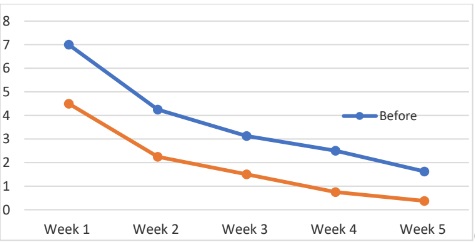 Figure 1: Before-After OMT Pain Trend.
Figure 1: Before-After OMT Pain Trend.
The sampling was of convenience structured on voluntary participation upon receipt of written informed consent. The study took place in the period from 13 November 2015 to 1st October 2017.
The research was in accordance of Helsinky Declaration. The protocol was approved by the pediatric ethics committee of the Tuscan region on 12 November 2015.
At the time of enrollment, the patient was included in the study: pain was detected by VAS scale and QoL was measured through the FS36 questionnaire at zero time.
Subsequently, the patient underwent a 30-minute OMT session, weekly for the first two weeks, every 15 days for the following 3 weeks, and a total of 5 osteopathic manipulation sessions. The pain symptom was measured before and after each session and the QoL was measured again at the end of the session.
The data were collected anonymously using special forms, assigning a numerical code to each patient (for example 001) and entered in an anonymized database, suitably pre-established through the EXCEL calculation program and processed in an aggregate manner with the EPINFO statistical program. The confidence interval (I.C.) used was 95%, the P value less than 0.05. The variables were assessed on the basis of their frequency and their means, the qualitative ordinal and nominal ones subjected to the Chi2 test, the quantitative ones assessed with Student's T test for parametric data and ANOVA for the analysis of variance; if the test is not parametric, the variance with the Kruskal-Wallis test will be evaluated. The data will be crossed to establish the relationship between the score of the answers and the demographic and anamnestic characteristics.
The study does not aim to generalize the data to the whole thalassemia population, but to evaluate the effectiveness of a treatment still with scarce evidence. However, it may be useful for promoting future studies.
Results
There were 8 subjects enrolled. The analysis of the data showed that the sample consisted of 1 male and 7 female patient, one of whom was pregnant at 22+5 weeks of gestation. The average age is 41.8 years DS+- 6.8. Out of 8 enlisted subjects, two are unemployed while one is not responding; in most cases (five) it is paperwork, one of which is a freelancer, currently unemployed. The survey participants almost all present one or more hobbies, only two do not respond, most of them have a hobby that physically engages them in activities, such as walking. Most of the respondents are affected by Thalassemia Mayor, only one person has Blackfan-Diamond syndrome. Seven out of eight subjects have active or past co-morbidities of some importance including: HCV infection, stroke, diabetes, cirrhosis, osteoporosis and dysmenorrhea.
Six out of eight patients have joint pain, seven out of eight have previous trauma, iron chelation therapy is present in most of the participants, and one person uses antidepressants.
Results of pain perception data: Pain was measured with the VAS scale before and after each osteopathic treatment, for all 5 sessions weekly.
At zero time (first detection performed before the first treatment) has an average pain of 7 DS+-2.39, ranged between 4 and 10, median 7 modes 4 emerged. The last post-treatment detection indicates an average perceived pain value of 0.37 DS +- 0.52, range between 0 and 1, median0 mode 0. (Table 1) Shows the average values on the perception of pain before and after osteopathic treatment, for each session of the treatment cycle.
|
Before-After OMT - VAS detection per cycle of five sessions |
|||||
|
|
Before |
After 5 Day |
Difference |
DS |
P Value |
|
Before OMT average time 0 and after 1 treatment |
7 |
4,5 |
2,5 |
+- 2,39 |
0,068 |
|
2 before OMT average and after 2 treatment |
4,25 |
2,25 |
2 |
+- 1,91 |
0,02 |
|
3 before OMT average and after 3 treatment |
3,125 |
1,5 |
1,63 |
+- 1,45 |
0,01 |
|
4 before OMT average and after 4 treatment 0,001 |
2,5 |
0,75 |
1,75 |
+-1,07 |
0,001 |
|
5 before OMT average and after 5 treatment |
1,625 |
0,375 |
1,25 |
+- 0,52 |
0,02 |
Table 1: Osteopathic Manipulative Treatment (OMT) and Visual Analogic Scale (VAS).
In the table two shows the numerical values of the average of the VAS scale relating to the perception of pain deriving from the comparison of the Before-After single osteopathic treatment value, for the entire cycle of treatments, five sessions of manipulative therapy, the first two weekly, the following three, every fifteen days. (Table 2)
|
Mean Difference of Pain Perception before treatment 1 and after subsequent treatements OMT |
|||
|
|
average difference best perception pain |
DS |
P Value |
|
|
|
|
|
|
Mean difference before 1 after 2 |
4,75 |
+- 1,39 |
0,00025 |
|
|
|
|
|
|
Mean difference before 1 after 3 |
5,5 |
+- 1,19 |
0,00004 |
|
|
|
|
|
|
Mean difference before 1 after 4 |
6,25 |
+- 0,71 |
0,00001 |
|
|
|
|
|
|
Mean difference before 1 after 5 |
6,63 |
+- 0,52 |
0,00001 |
|
|
|
|
|
Table 2: Above graph one, shows the trend of the values mentioned in table two.
Results of perception of QoL data: The 36-item short-form scale (SF-36) was used, administered before starting the cycle of 5 treatments (T0) and at the end of the cycle itself. Out of 8 observed parameters, the following was highlighted:
- At zero time an average 88.6 SD + - 14,3, range 74.1 - 119.3, median 86.3 and mode of 74.1.
- At the end of the treatment cycle an average of 97.6 SD + - 15.2, range between 76.2 and 123.8, median of 98.9, mode of 76.2.
Table number three shows the detailed values concerning each item making up the FS36 scale and the total of the values. At Student's T test, a value of P = 0.42 is highlighted.
Table number four shows the average values for each item and the total of the averages. At the student's T test, a value of 0.43 is highlighted (Tables 3 & 4).
|
QoL score comparison before OMT and post OMT cycle (five sessions)
|
||
|
|
total PRE |
total POST |
|
|
|
|
|
Physical activity value |
88,1 |
107,8 |
|
|
|
|
|
Role value and physical health |
74,1 |
85,2 |
|
|
|
|
|
Physical pain value |
95,5 |
85,6 |
|
|
|
|
|
Health value in general |
77 |
104,5 |
|
|
|
|
|
Vitality value |
80,3 |
96,5 |
|
|
|
|
|
Value Social activities |
119,3 |
123,8 |
|
|
|
|
|
Role and emotional state |
90,1 |
101,2 |
|
|
|
|
Table 3: The detailed values concerning each item making up the FS36 scale.
|
Average QoL score comparison Before OMT and After OMT cycle (five sessions)
|
||
|
|
Averages Before |
Averages After |
|
|
|
|
|
Average physical activity BEFORE |
65,6 |
70 |
|
|
|
|
|
Average role value and physical health BEFORE |
3 |
40,6 |
|
|
|
|
|
Average physical pain value BEFORE |
22,5 |
62,2 |
|
|
|
|
|
Average Health value in general BEFORE |
76,8 |
35 |
|
|
|
|
|
Average vitality value BEFORE |
84,4 |
49,4 |
|
|
|
|
|
Average value social activities BEFORE |
18 |
59,4 |
|
|
|
|
|
Role and emotional state BEFORE |
5,6 |
66,7 |
|
|
|
|
|
Average mental health value BEFORE |
65,6 |
79,5 |
|
|
|
|
|
Average Values Total |
341,5 |
462,8 |
|
|
|
|
Table 4: The average values for each item and the total of the averages.
Discussion
From the above data, the sample under study is mainly composed of female persons, with an average age of 41.8 years DS+- 6.8. It is interesting how the distribution of age groups and gender can be superimposed on the aforementioned study [10], probably due to the need to address aspects of illness of the disease.
Noteworthy, in our sample, the presence of an interviewee during pregnancy, given that ISTAT data published in 2015 estimate that only 12% of thalassemia women can have children, due to the high complication of infertility linked to transfusions [10].
Most of the interviewees declare to do clerical work; one declares himself unemployed, finally one freelancer. The belonging of most patients enrolled in similar types of work could be due to the need to have flexible work commitments and reduced physical effort. However, it remains a very important fact for the assessment of the QoL, the possibility of maintaining a constant but flexible working commitment to the care commitment that the disease itself requires; think of the impact of transfusions, their frequency and constant medical consultations for primary and related problems (orthopedic, cardiology, endocrinology, etc.). The fact that most of the sample has a hobby or an interest, such as reading, listening to music, light physical activity, etc., indicates an active lifestyle and that in everyday life it does not seem to be deeply affected by the disease. The major limitation to all these daily activities is determined by tiredness and a sense of fatigue caused by anemia (35%), followed by commitments related to visits to the hospital and transfusions and therapies (19%). The pains of the skeletal muscle system are also mentioned, which limit physical activities (13%), the management of complications of the disease (8%), the general state of health (6%) and the psychological factors due to the lowering of the mood, lack of stimuli, presence of fears and worries (6%) [10]. Only one interviewee said he had to stop physical activity, probably due to the worsening of the painful symptoms and the current state of the disease, as well as to advancing age which may have caused functional limitations.
Almost all of the participants (seven out of eight) report comorbidities such as osteoporosis, hepatitis c, diabetes, cirrhosis, dysmenorrhea, cerebral ischemia, allergies, constipation, frequent in patients with thalassemia or polytransfusions, especially if prior to the discovery of the hepatitis C virus. Seven out of eight people report previous traumatic injuries, which could affect exacerbating pain symptoms and problems affecting the osteoarticular system; it would therefore be necessary to enlarge the sample to perform a stratification to limit the confounder.
The presence of joint pain is reported by the entire enrolled sample, none of them reported the use of pain relieving drugs, except one person who indicated taking Chondrotin for the treatment of osteoarthritis; also for this variable further studies and the enlargement of the sample would be necessary. At the conclusion of our study, which aimed to improve pain symptoms, important results can be highlighted: the difference between average pain referred to patients at zero time (equal to 7) and pain reported at the end of the treatment cycle, after the administration of the last OMT, (equal to 0.375) is comforting; this associated with a P value lower than 0.05 already from the second week of OMT also highlights a statistical significance of the data. Even analyzing the difference in perceived pain between the detection at time zero and that perceived after each administration of OMT it is noted that this is already wide from the first treatment (4.75; SD1.39; P Value = 0, 00025), but very clear at the end of the 5 weeks (6.63; SD 0.52; P Value = 0.00001) (tables 1 & 2). As regards the impact on the QoL (SF36 scale) [11], even if with an improvement trend, the data do not reach the expected statistical significance. However, there is a clear improvement both on the raw value and on the averages, values that could have significant changes with the increase in the sample size.
From a first evaluation, some items show an improvement in the QoL; examples are: the value of "Physical activity" which has gone from an average of 88.1 to an average of 107.8 with a difference of 17.7 points; the value of "Health in general" with an initial score of 77 and a post-surgery score of 104.5, with a difference of 27.5 points.
Even analyzing the averages for each item investigated, it is noted that these have all increased after osteopathic treatment, except for the raw value of the Mental Health item.
The analysis of the sum of the QoL values 708.8 vs 780.8 indicates an improvement, even if it does not follow the exponential trend obtained with the "pain" variable.
Finally, from the total average values this improvement is appreciated (88.6; SD 14.2625 vs 97.6; SD 15.1562 with an average increase of 9 points). Unfortunately, these data on the ANOVA test, applying the Kruskal-Wallis test, have not been confirmed the statistical significance, P Value = 0.43 (Tables 3 & 4).
Conclusion
At the conclusion of our study, we can affirm that the results obtained by us, even if coming from a small sample, highlight the usefulness and efficacy of OMT in adult patients with Thalassemia Mayor with various types of joint pain, but it could also be hypothesized that those who have benefited from osteopathic treatment for several consecutive sessions, although affected by other chronic disabling diseases, such as BTM, may also enjoy the positive effects.
This survey highlights the benefits that OMT could offer to thalassemia patients, taking advantage of a new treatment opportunity for the endpoints identified and pursued within the same specialist care center, thus opening a reflection on the possibility of including in the team also the figure of the osteopath, in line with the need to deal with the management of complex pathologies within a multidisciplinary setting. A final aspect, not of secondary importance, that
emerged in this study was that the OMT included in the transfusion care protocol probably influenced the increase in the QoL of the patients, with possible implications for the management of one's daily life, decreasing the time and the costs necessary to deal with the management of these aspects often in third structures, with consequent possible effects on work and / or family and / or social life absences.
Unfortunately, the thalassemia population on which we carried out the study was limited, and enrollment was made difficult by the inclusion and exclusion criteria, which served to limit their confounders, biases and modifiers; it would therefore be desirable to carry out the multicenter study in order to expand the sample and perform necessary stratifications. The organizational and structural difficulties did not allow to complete the study on the chosen number of 10 units, but it proved its effectiveness on the pain symptom and therefore, indirectly, also on the QoL. Unfortunately, the second area studied, that of QoL, did not achieve the same results with the expected statistical significance; however, it showed an important improvement trend that could have a more comforting result with an increase in the sample size.
At the conclusion of our study, we observe how the results are in line with other surveys carried out and published after the start of this study, aimed at people with BTM, aimed at investigating qualitative-quantitative aspects of the QoL and care of themselves.
The limitations of the study were those of the small size of the sample and the logistical difficulties, which led to having to conclude the study with a sample lower than the predetermined one, which was already very small. For the future, it may be useful to carry out a cohort study with a competing cohort to better evaluate the effectiveness of the OMT, but it needs more resources and a multicenter design to allow the evaluation of the variables studied on a larger sample.
Competing interests
The authors have declared that no competing interests exist.
References
- Weatherall DJ, Clegg JB (2001) The Thalassaemia syndromes 4th edition. Blackwell Scientific.
- Silvestroni IB (1998) Le talassemie un problema medico-sociale ieri e oggi. Roma Istituto Italiano di Medicina Sociale.
- Atzeni MM, Masala A (2002) La Beta talassemia omozigote. Caleidoscopio Italiano.
- https://www.osservatoriomalattierare.it/malattie-rare/talassemia
- Rosatelli MC, Dozy A, Faà V, Meloni A, Sardu R, et al. (1992) Molecular characterization of β-thalassemia in the Sardinian population. Am J Hum Genet 50: 422-426.
- Rosatelli MC, Tuveri T, Scalas MT, Leoni GB, Sardu R, et al. (1992) Molecular screening and fetal diagnosis of β-thalassemia in the Italian population. Human Genetics 89: 585-589.
- http://www.vita.it/it/article/2010/10/29/la-talassemia-tornamaparlalinguestraniere/105659/
- Ganz T (2003) Hepcidin A key regulator of iron metabolism and mediator of anemia of inflammation. Blood 102: 783-788.
- Angastiniotis M, Eleftheriou A, Galanello R, Harteveld CL, Petrou M, et al. (2013) Prevention of thalassaemias and other haemoglobins disorders.
- Kontoghiorghes GJ, Neocleous K, Kolnagou A (2003) Benefits and risks of deferiprone in iron overload in Thalassaemia and other conditions: Comparison of epidemiological and therapeutic aspects with deferoxamine. Drug Saf 26: 553-584.
- Bordbar M, Pasalar M, Safaei S, Kamfiroozi R, Zareifar S, et al (2017) Complementary and alternative medicine use in thalassemia patients in Shiraz, southern Iran: A cross-sectional study. J Tradit Complement Med 8: 141-146.
- https://www.medicinanarrativa.eu/wp-content/uploads/2015/12/Introduzione-al-report-Il-valore-per-la-persona-con-Beta-Talassemia-Major.pdf
- https://www.medicinanarrativa.eu/wp-content/uploads/2015/12/Introduzione-al-report-Il-valore-per-la-persona-con-Beta-Talassemia-Major.pdf
- https://www.tuttosteopatia.it/wp-content/uploads/the-european-framework-for-standards-of-osteopathic-practice-efsop11.pdf
- Maggio A, Caronia F, Russo G (2000) Clinica e Terapia della Talassemia.
- Castoldi G, Liso V (2013) Malattie del sangue e degli organi emopoietici. 6°e. McGraw-hill 102-105.
- Becker R (2009) La vita in movimento. Futura Publishing Society.
- Radman Z (2013) The Hand, an Organ of the Mind. Cambridge: The MIT Press.
- https://icomedicine.com/wp-content/uploads/2020/08/EFSOET-ICOM.pdf.
- Morte LK (2005) The human orbitofrontal cortex: Linking reward to hedonic experience. Nature Reviews Neuroscience 691-702.
- Finnerup NB, Johannesen IL, Fuglsang-Frederiksen A, Bach FW, Jensen TS (2003) Sensory Function in spinal cord injury patients with and without central pain. Brain 126: 57-70.
- Matthews HL, Janusek LW (2011) Epigenetics and psychoneuroimmunology: Mechanisms and models. Brain Behav Immun 25: 25-39.
- Morhenn V, Beavin LE, Zak PJ (2012) Massage Increases Oxytocin and Reduces Adrenocorticotropin Hormone in Humans. Altern Ther Health Med 18: 11-18.
- Rapaport M, Schettler P, Bresee C (2012) Journal of Alternative and Complementary Medicine. A Preliminary Study of the Effects of Repeated Massage on Hypothalamic-Pituitary-Adrenal and Immune Function in Healthy Individuals: A Study of Mechanisms of Action and Dosage. J alter and complementary med 18: 789-797.
- Dunbar RIM (2010) The social role of touch in humans and primates: Behavioural function and neurobiological mechanisms. Neurosci Biobehav Rev 34: 260-268.
- Elkiss ML, Jerome JA (2012) Touch: More than a basic science. J Am Osteopathic Ass 112: 514-517.
- Crane JD, Ogborn DI, Cupido C, Melov S, Melov S, et al. (2012) Massage therapy attenuates inflammatory signaling after exerciseinduced muscle damage. Sci Transl Med 1: 4.
- Bordoni B, Zanier E (2015) Understanding fibroblasts in order to comprehend the osteopathic treatment of the fascia. Evid Based Complement Alternat Med.
- Mitchell LE, John AJ (2012) Touch-More than a Basic Science. J Am Osteopath Assoc 112: 514-517.
- Bottaccioli IL (2008) Sistema immunitario: La bilancia della vita 22: 231-235.
- Bordoni B, Zanier E (2014) Clinical and symptomatological reflections: The fascial system. J Multidiscip Healthc 7: 401-41.
- Bordoni B, Marelli F (2017) Emotions in motion: Myofascial interoception. Complement Med Res 24: 110-113.
- Schleip R, Jäger H, Klingler W (2012) What is “fascia?” A review of different nomenclatures. J Bodyw Mov Ther 16: 496-502.
- Walkowski S, Singh M, Puertas J (2014) La terapia manipolativa osteopatica induce il rilascio precoce di citochine plasmatiche e la mobilizzazione di una popolazione di cellule dendritiche del sangue. Plos One 9: 90-132.
- Alessandro G, Cerritelli F, Cortelli P (2016) Sensitization and Interoception as Key Neurological Concepts in Osteopathy and Other Manual Medicines. Front Neurosci 10: 100.
Citation: Ciofi D, Fracchiolla F, Cuccoli B, Casini F, Ferroni T, et al. (2022) Osteopathic Treatment in Adult Patients Whit Hemoglobinopathies: A Coort of Study for Pain Evaluation and Quality of Life. J Community Med Public Health Care 9: 116.
Copyright: © 2022 Daniele Ciofi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.