Osteopathy in the Cranial Field from a Systems Theory Perspective
*Corresponding Author(s):
Rene J ZweedijkDutch Osteopathic Association, Panta Rhei Opleidingen, Netherlands
Tel:+31 653420392,
Email:rene@pro-osteo.com
Abstract
There is a lot of controversy about osteopathy in the cranial region. Various terms are used in the literature. Explanatory mechanisms and effectiveness are also under discussion. The aim of this article is to describe through literature review the historical base of this confusing situation, provide a clear and generally acceptable definition of the terms used, provide a scientific explanation for primary respiration and propose future research in this field. W.G. Sutherland, considered as founder of osteopathy in the cranial field, had two different periods in his scientific life. The first was dominated by mechanical view on the cranium which scientifically can be supported by the “five Model” concept. However, this “five model” concept gives no scientific base for terms such as “primary respiration”, ”Breath of Life” and others that were described by Sutherland is the later period of his life and nowadays used in Biodynamic model of Osteopathy in the Cranial Field (BOCF). Although there is a great controversy about the Biodynamic aspect of osteopathy in the cranial field, today it is considered as an important part of the profession, and furthermore osteopathy is not osteopathy without it. In this article a scientific approach which has his origin in systems biology and chaos theory, is presented. A proposition is made for scientific substantiation of “Primary respiration” and related concepts, including suggestions for future research. For research and support, the field of mathematics, artificial intelligence, chaos theory and complex systems thinking can be of fundamental and essential value.
Introduction
There is a lot of controversy about osteopathy in the cranial region. Various terms are used in the literature, such as Osteopathy in the cranial field, Cranial Osteopathic Manipulative Medicine (Cranial OMM), craniosacral osteopathy, or craniosacral therapy [1-3]. In some countries, cranial osteopathy has a very different meaning and refers to more biodynamic aspects of osteopathy [4]. In addition to the fact that there is no uniformity in terminology, explanatory mechanisms and effectiveness are also under discussion. Guillaud indicates that there is little or no sound scientific basis for Cranial OMM and that high-quality effect studies are lacking [5]. Others, such as King and Cerritelli, report positive results [6,7].
It is clear that more good research is needed on both the explanatory mechanisms and the effectiveness, as many systematic reviews show that the quality of studies carried out is often weak to poor [1,8].
The definition of Cranial Osteopathic Manipulative Medicine is as follows: Cranial osteopathic manipulative medicine (Cranial OMM) involves the manipulation of the primary respiratory mechanism to improve structure and function in children and adults [1]. The primary respiratory mechanism plays a central role in this definition. It is precisely this primary respiratory mechanism, important as it may be in osteopathic practice that causes much confusion, controversy, discussion, and misunderstanding. Concepts such as "Primary respiratory mechanism" (PRM), "Breath of Life", "tide", "potency", "Cranial Rhythmic Impulse" (CRI) are used interchangeably, which causes a lot of confusion. Recent publication of Rasmussen in this journal describes a third rhythm in the cranium, but also here terms as CRI and PRM are mixed and there is no clear definition and explanation for both of them [9]. The history of the Cranial-OMM provides some clarity as to the origin of this confusing situation. The fact that Sutherland had two different periods in his intellectual life concerning the cranium and that these two views are constantly mixed, may be crucial in the professional confusion still present in osteopathy. The importance of evidence-based practice obliges osteopathy to clarify these terms and seek scientific support for them [10].
This article aims to describe through a literature review the historical base of this confusing situation, provide a clear and generally acceptable definition of the terms used, provide a scientific explanation for primary respiration movement and propose future research in this field.
History of Cranial Osteopathy
WG Sutherland formulated his first cranial hypothesis as early as 1899 when he was still a student of AT Still. WG Sutherland spent his whole life developing his ideas on cranial mobility. In the first period, between 1910 and 1930, he focused on the mobility of the cranial bones, the sutures, and the importance of the foramina. From the beginning of the 1930s, he concentrated on the dura mater with its intracranial connections. At the end of the 1930s, his focus is on the Cerebro Spinal Fluid (CSF) and the mobility/motility of the brain [11]. In his work "the Cranial Bowl" he describes that the mobility of the skull originates from a mechanism inside the skull, the primary respiratory mechanism [12]. According to him, because other structures that can stimulate the sutures to move, such as muscles, are lacking, the movement had to come from within the skull. Sutherland described the 5 elements of cranial mobility: 1) the mobility of the sutures, 2) the reciprocal tension of the membranes, 3) the mobility of the sacrum around the axes of Sutherland, 4) the fluctuation of CSF and 5) the inherent motility of the brain [13]. In this period he found the fluctuation of LCS and the inherent motility of the brain to be leading. A colleague working in the same period, Charlotte Weaver, saw the bone fragments of the skull as modified vertebrae based on embryological studies, something which had already been described by Goethe at the end of the 18th century [11]. In 1943 Sutherland’s view changed. By working with patients he came concluded that the Primary Respiratory Mechanism (PRM) is not only felt in the skull but throughout the whole body. He speaks of a force, "the Breath of Life", which puts the body into motion, as it were. In 1948 he speaks of the "Tide" and of "potency". He sees this as a mechanism that moves through the patient as it were. As a metaphor, he uses the lights of a lighthouse that rotate and regularly shines a beam of light on something. At the beginning of the fifties, he stops testing mobility and starts working with Fulcrums and Still Points. In the sixties, his lessons are published by Ada Sutherland and Ann Wales. Unfortunately, there are no books that clearly depict the intellectual path Sutherland has taken. In 1961 Rachel and John Woods speak about "The Cranio Rhymthic Impulse (CRI)" for the first time, a rhythm of 6-12 cycles/min. This indicates the rhythm that can be felt in the skull. In his "pressure-stat" model Upledger speaks of the same rhythm [3]. There is no consensus about what the physiological foundation for this rhythm is [14]. According to Nelson, it is the Traub Hering Mayer movements that are perceived [15]. Others such as Milne indicate that the CRI has its origin in entrainment between different rhythms present in the skull [16]. More about this later. In the 50s to 70s Magoun and Becker published their work in which they particularly shed light and elaborate on the insights of Sutherland's last life period [2,17]. Sutherland's last phase is characterized by the vision that the body is a polyrhythmic system in which the "the Breath of Life" transubstantiates into PRM within the body and generates different rhythms such as the "long tide", a Fluid Rhythm of 2-3 c/min and a 300-sec rhythm [11]. Over the last 40 years, it was James Jealous in particular who developed Sutherland's later ideas and called them biodynamic aspects within osteopathy, Biodynamic model of Osteopathy in the Cranial Field (BOCF) [11]. Table 1 shows years and the development of Cranial OMM.
|
1910-1920 Sutherland starts studying cranial bone fragments, sutures and foraminae |
|
Early thirties Sutherland experiments with the dura mater and its duplicates. |
|
Late 1930s Sutherland focuses on the fluctuation of the CSF and talks about the Primary Respiratory Mechanism (PRM). |
|
1936-1938 Charlotte Weaver dissects foetal skulls and concludes that the bones of the base of the skull are modified vertebrae. SSB is an embryological homologue to the intervertebral disc |
|
1943 Sutherland describes the Breath of Life |
|
1948 Sutherland starts working with the tidal potency |
|
1951 Sutherland stops testing agility, works with fulcrums and Still Points |
|
1960s Sutherland's work is published by Ann Wales and Ada Sutherland. |
|
1970s Sutherland's students Rolin Becker and Robert Fulford expand Sutherland's work after 1943 |
|
1980s James Jealous delves into the works of Sutherland and links this to works of E.Blechschmidt and others. |
Table 1: Shows years and the development of Cranial OMM.
The five-model concept in osteopathy
Osteopathy focuses on promoting the body's capacity for self-healing and is based on the concept of the unity of the individual's structure (anatomy) and function (physiology). The human body is a unity formed by the permanent continuity of structures.
The “five model concept”, defined by the Educational Council on Osteopathic Principles (ECOP), is a generally accepted and useful model and are perspectives of how one might view the patient in osteopathy [18,19]. The five models contain:
- Mechanical model
- Neurological model
- Respiratory/circulatory model
- Bioenergetic/metabolic model
- BioPsychoSocial(behavioural) model
A Dysfunction concerns an altered function concerning one (or a number of the models) and leads to the disruption of the body's self-healing capacity [18,20].
The “model of 5” in Cranial-OMM
Osteopathy claims to be holistic, using a different model for the cranium is contrary to holism, and strange to say the least. It would therefore be obvious to apply the “five model” concept with its dysfunctions to Cranial-OMM as Kales proposes in his publication in 2017 [21]. In principle, this is in line with Sutherland's initial findings for his period before 1948 [11]. There is an overload of research supporting the observations done by Sutherland in his early period, and the premise that the five model concept can be used in scientific support of osteopathy in the cranial field, and can serve as a model for future research [7,9,13,21,22]. Discussion of these findings is beyond the aim of this article.
Primary Respiratory Technique, Cranial Rhythmic Impulse, Breath Of Life
It may be clear that none of the above models form the foundation for the "primary respiration mechanism", the "Cranial Rhythmic Impulse" or "The Breath of Life", not even the circulatory model with its Traub-Hering-Mayer waves or the recently described third rhythm by Rasmussen [9,15,23]. Sutherland's theory that the cranium needs mobility in connection with the primary respiratory mechanism is therefore outdated. It is cognitive dissonance to deny this. Strangely enough, it is still taught in schools all over the world and can be found in many osteopathic papers. It is also remarkable that the different terms are used interchangeably in both education and literature. The fact that the above models cannot form a basis for the PRM, does not mean that it is not perceivable and that it does not play an essential role in osteopathic research and treatment. Indeed, osteopathy is not osteopathy without the implementation of the PRM and osteopathic touch is not osteopathic touch without the perception of the PRM. Within the biodynamic model of osteopathy in the cranial field, the "primary respiratory mechanism" and "the breath of life", among other things, play a central role.
Biodynamic model of osteopathy in the cranial field
In an excellent article from 2005, John McPartland writes: "The nonrational aspects of osteopathy (and other alternative medical systems) are the most difficult lessons to impart and the most difficult traditions to maintain [11]. Still's principle "Man-as-triune" (Body-Mind-Spirit), which formed the basis of his work fell victim to medical reductionism, a consequence of Western thinking, where there is no, or little and room for the intuitive and instinctive. Within the osteopathic community, there remains the conviction that Still's and Sutherland's later principles make osteopathy into osteopathy and these principles should be respected and implemented.
The language that Still and Sutherland use reflects their deep connection with the natural world. This unique connection has been picked up by James Jealous. He used the name Biodynamics, a term he borrowed from the German embryologist Erich Blechschmidt, who probably, in turn, adopted the term from Rudolph Steiner, the German anthroposophist. Biodynamics can be defined as: "a new way to integrate scientific understanding with a recognition of spirit in nature" (https://www.biodynamics.com/what-is-biodynamics). Over the past 45 years Jealous has combined Sutherland’s lessons, drawn from the mouths of his pupils such as Ruby Day and Ann Wales, with the study of his work. Through this, he has come to his own unique interpretation of Sutherland’s work and partly that of Still. Jealous is particularly interested in the later phase of Sutherland's work. Jealous has published very little, his works are united on audiotapes [11,24,25].
McPartland indicates that the origin of biodynamics lies with Hippocrates, something that can still be found in the oath of Hippocrates, "Primum non nocere" and man as a three-part being, "body-mind-spirit" [11]. Besides, within the biodynamic aspects of osteopathy (also called the Biodynamic model of Osteopathy in the Cranial Field (BOCF)), names are given to processes that are perceptible in the interaction between patient and practitioner. We will discuss a number of these processes and consider whether a possible explanation for this can be found within science, or at least in which direction a possible substantiation can be found. It should be noted that the BOCF is so rich in terms and principles that it is impossible to cover everything.
Primary Respiratory Mechanism (PRM) and "Breath of Life", new insights
According to Sutherland, the human body is a polyrhythmic system [11]. It is "The Breath of Life", an external force, at least so it seems, which is characteristic of all living beings, and which incites the body to movement, manifesting itself in the various rhythms felt in the body. The question is; what exactly does Sutherland describe, and what is the possible explanation for this mechanism?
Life and rhythms
Researcher Jeremy England published a paper in 2013 in which he states that the origin of life is not so much a matter of luck, but that the origin of life and evolution are the result of fundamental laws of nature. It is no more surprising than rocks rolling down a hill. That life arises is a natural process. It is a law that life arises. Using computer simulations, he showed that structures can become more complicated under the influence of rhythmic forces. Based on the ideas of Jeremy England, life can therefore be qualified as emergent structure and function [26]. It is a law that life becomes more and more complicated and complex under the influence of the rhythm of life. There is, in Biblical terms, a force that breathes life into dead matter.
"The Breath of Life", a term used by Sutherland and in BOCF, is the metaphor for a special emerging characteristic of the body. "The Breath of Life" seems to come from outside but is however a process within the body. The body is a complex adaptive system with emergent properties. Life emerges in the same way that consciousness arises in a normally functioning brain. When all parts of the system work together optimally, a well-functioning complex system emerges, and "The Breath of Life" shows itself; it is a product of the WHOLE. The “Breath of Life” may be said to correspond to the force described by England [26].
Chaos and rhythms
Living systems evolve in an intrinsically unpredictable way, driven in part by the complex relationships between systems. They co-create their future. These interactions generally take the form of positive and negative feedback. The dynamics of feedback systems can take three main forms. On the one hand, they can be stable or fixed, potentially leading to rigidity, and on the other hand, they can be unstable or chaotic, ultimately leading to disintegration. Lastly, dynamic systems can show periodic behavior. Such behavior is characteristic of living systems, such as humans. Their functioning is based on basis oscillators, waves, rhythms, and clocks (Figure 1).
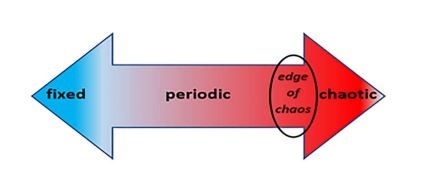 Figure 1: Life resides on the edge of chaos, the transition zone between order and disorder [27].
Figure 1: Life resides on the edge of chaos, the transition zone between order and disorder [27].
Fixed and periodic behavior are orderly, while chaotic behavior represents disorder. The edge of chaos refers to a transition area between order and disorder. Life in all its potential resides on the edge of chaos. Waldrop [28] wrote in his book entitled Complexity: “The edge of chaos is where life has enough stability to sustain itself and enough creativity to deserve the name of life [28].
Life exists because of rhythms and waves. These are characterized by a certain orderliness, but must also show some degree of chaotic behavior. This duality is characteristic for the edge of chaos, and therefore of life. In Waldrop’s words: “The edge of chaos is the constantly shifting battle zone between stagnation and anarchy, the only place where a system can be spontaneous, adaptive, and alive [28].”
Systems theory and rhythms
A human body is not a machine. Besides the fact that the human body can be seen as a system with chaotic properties [29], it is also a complex adaptive system [30]. The body adapts to changes in the internal and extreme environment to maintain homeostasis and allostasis. These changes are so present that Lloyd argues that it is better to speak of homeodynamics rather than homeostasis, since the latter suggests a static phenomenon, whereas it is a dynamic mechanism [31]. This of course also applies to allostasis where allodynamics is a more appropriate term [32]. The theory of complex systems shows that interaction between parts (cells, tissues, organs, organ systems) leads to collective behavior of those parts; the system behaves as a whole. Complex systems are self-regulating, there is no control center and the body is an autopoietic system [33]. Complex systems exhibit emergent behavior in which the whole can exhibit completely different behavior than the separate parts. An appealing example of this is a swarm of birds preparing for migration to the south, which also exhibits emergent behavior.
Information and rhythms
For Sutherland and the Biodynamic model of Osteopathy in the Cranial Field (BOCF) rhythms are so important for health, the question is, “why?” Human beings are living systems that interact with their environment. These systems are open systems maintained by continual flows of matter, energy, and information. Without this triad, life cannot exist. Of this triad, information deserves special interest. This because it is an interesting observation that information shapes biological organization in fundamental ways and at every organizational level. Organisms use information for interaction with the environment, and to construct, maintain, repair, and replicate themselves [34]. To understand what life is, what health is, and what are useful interventions, it is therefore necessary to understand the role of information.
Information is stored in the structures of systems, and transmitted by rhythms, vibrations, and oscillations. These processes create resonances in the tissues and fine-tuning between organs. In healthy organisms, these rhythms are rather free to express themselves. Organisms, like humans, cannot exist without information and interaction. Man is made of information and rhythms. This is in line with Sutherland's and BOCF theory, that the body is polyrhythmic; life in all its fullness is an interplay of rhythms.
Harmony, rhythms, Breath of Life, and primary respiration
As described before, the body is a complex adaptive system with emergent properties. "Life emerges in the same way that consciousness arises in a normally functioning brain. When all parts of the system work together optimally, a well-functioning complex system emerges, and "The Breath of Life" shows itself. Rhythms in the body ensure a relatively stable systemic functioning [35]. There is a multitude of rhythms measurable in the human body [36]. Part of these rhythms is aimed at organic stability through calibration of the system and its properties, during sleep and rest. Organisms continually adapt to internal and external processes and signals, and do so by continuously adjusting their rhythms simultaneously and adequately. This tuning and synchronization of rhythms reduces the energy consumption of the organism. Huygens has been able to observe a similar synchronization with two clocks with pendulum mechanism that stood next to each other, and that after some time started to synchronize, more precisely, they started to run in counter-phase [37]. The many rhythms in an organism can be compared to the vibrations of the various instruments in an orchestra. If they are well attuned to each other they can, for example, play a beautiful piece of music. The life of an organism can be characterized as a continuous and ever-changing sequence of polyrhythms. Thus, following Moser [35], in a certain sense, you can speak of “The symphony of life”.
The November 2019 Science magazine published an article on research into rhythms during non-rapid eye movement sleep, using time series, among other things. The results of that research show that there is then a coherent pattern of oscillating electrophysiological, hemodynamic, and CSF dynamics. The sleeping brain exhibits neural slow waves of CSF flow, and these CSF dynamics are linked to neural and hemodynamic rhythms [38]. One of the researchers noted: “We said that there are electrical waves of activity in the neurons. But before now, we did not realize that there are actually waves in the CSF, too. It’s such a dramatic effect” [39].
Sutherland's observation that a human being is a system with different rhythms is confirmed by science [33,35,36,]. Synchronization takes place between these rhythms, where the micro-level (cell) influences the macro-level (brain) and vice versa [31,35,40]. When the patient is laid down relaxed on the treatment table, the osteopath perceives the Primary Respiratory Mechanism (PRM). This primary respiratory mechanism could find its origin in the mutual amplification of various rhythms based on [41]:
- Entrainment of certain rhythms: synchronization between the rhythms
- Magnetic effect: entrainment even when there is no synchronization between rhythms
- Superposition: Adding or subtracting a rhythm is a combination of entrainment and the magnetic effect
All this leads to resonance with a relatively large amplitude: the primary respiratory mechanism. This same mechanism is probably the basis for other rhythms such as the long tide and the 300-sec rhythm. Stress, pain, poor nutrition, circulatory disorders, hormonal disorders, somatic dysfunctions and such are all capable of disrupting this rhythm. Sleeping well, breathing exercises, and even listening to the recitation of a poem have been shown to increase the coherence between breathing, Heart Rate (HRV) and an EEG [42].
Wholeness
One of the basic principles of the biodynamic vision is "the wholeness", a principle that is also described in the literature and is a property in complex adaptive systems such as humans [25,35]. To understand exactly what this means, we consult the Hungarian thinker and writer Koestler (1905-1983) [41]. He suggested that the hybrid nature of systems or subsystems within larger systems should be referred to by the word Holon. At the same time, holons are self-contained wholes in relation to their constituent parts, and dependent parts in relation to encompassing systems. In other words, holons are both wholes and parts (Figure 2). Holons are self-sufficient, have a degree of independence and autonomy, and exist in symbiosis with their environment. But holons are also part of larger wholes, i.e. more encompassing holons. This means that although each Holon is relatively autonomous, the functioning of holons is partly determined by holons higher up in the hierarchy, that the behavior of holons is dependent on their environment, and that holons are related to holons lower down in the hierarchy. This implies that there is always two-way communication; bottom-up if you want to consider the effect of viruses in adipocytes, for example, and top-down if you want to consider what stress means for the epigenome. Sutherland said: “every drop knows the tide”, meaning that every cell in the human body is important and is a part of the WHOLE [43]. In BOCF the view of Erich Blechschmidt on the development of the embryo, where he states that the embryo develops as one, is supported by the theory of Koestler.
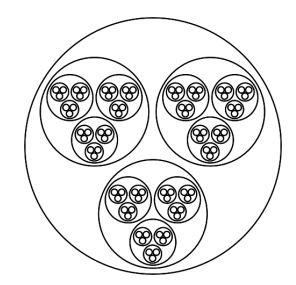 Figure 2: Holons by model of Koestler, the outer circle symbolizes man, the smaller circles organ systems, organs, tissues and cells [41].
Figure 2: Holons by model of Koestler, the outer circle symbolizes man, the smaller circles organ systems, organs, tissues and cells [41].
Neutral
Neutral is an important concept within the BOCF. All parts of the body form a whole, it feels like one big drop. One could say that neutral is a condition for complex systems to achieve emergent behavior. In the same way, for optimal functioning, the patient must be in neutral. Not only the patient needs to be neutral but also the osteopath. Cerritelli shows that a consciously directed palpation is experienced differently by the patient's brain and that different brain networks are active than when the osteopath listens to music during the palpation [44]. It should be noted that it is probably not the attention that is important, but the intention of the palpation. This is supported by the observation of Bengston who, through an intent approach to tumor cells in mice, was able to influence tumor growth and tumor markers [45]. Based on this consideration it can be stated that Neutral means that the osteopath approaches the body as a whole, in the here and now and with the right intention, independent of ego. Only then a complex duo-system arises.
Neutral and synchronisation
Interaction takes place between complex systems in each other's environment. This interaction, for example between two people, can be more or less meaningful. This depends, among other things, on the extent to which people want to offer each other space. This is also the case in the relationship between osteopath and patient. This relationship only works when the osteopath skips the importance of his ego. The osteopath should not treat anyone for a suspected condition without implicit or explicit consent, even with the best of intentions. Without that permission, a practitioner can do more harm than good. Patients should allow the osteopath to enter into a treatment relationship, with which they then form a duo system. You could say that also the relationship should be neutral.
In this neutral therapeutic relation process, the different rhythms of the body of the patient are observed and respected by the osteopath. The body of the patient forms one HOLON, all parts are united and reading to shift, the body is in the “here and the now”. This approach means that the complex system of the patient and the complex system of the osteopath “meet” and form one therapeutic HOLON. The aim of the palpation is observing and not to disturb but to respect the various rhythms and to Synchronise with them [43]. This approach makes every treatment relationship and even every treatment unique and incomparable. Becker talks about "zone C", ‘The fulcrum in the room’ [17]. A manual treatment like an osteopathic treatment that is done with respect for the self-healing capacity of the body is an interaction between two systems that influence each other. This also explains the poor intertester reliability, but also the better intratester reliability, which has been demonstrated in studies by, among others, Moran [46]. The observation of rhythms in the patient is a process in which the osteopath is part of the process and therefore it is a personal and unique observation. No experimental setup will ever be able to replace this observation, but mathematical models could give a prediction of the process if and when all factors are known [47].
Fulcrum
There are many definitions of what a fulcrum is, many of them from a mechanistic perspective [48]. A fulcrum can also be defined from a biodynamic perspective [43]. An organism is an open system, which means that it can interact with the environment. Interaction always involves changing the structure of a system. When a system receives information, for example through senses such as ear, eye, and skin, this leads to structural change. Rearranging a system means changing the functioning and information in the system. In an organism, this corresponds to a change in the state with possible health effects.
A fulcrum concerns a time-space event, the place, and the moment that the body's inherent power reveals itself. Metaphorically, a fulcrum is a soft but clear speaking voice and a listening ear, which can be at different times in different places. It concerns a place where the body is very sensitive to information that from that point can lead to a change (transmutation) in the direction of healthier functioning and appropriate structure. Moser also describes this as the moment and place when all rhythms show a synchronization, for example during deep relaxation and sleep.
Homeodynamics, homeorhesis and transmutation
Life is not static but dynamic like Sutherland wrote and maintaining health is a dynamic process so it is better to speak about homeodynamics and no about homeostasis [31]. There is not one control centre in the human body, it is the whole that does the regulation. The whole contains knowledge about what is normal and uses this knowledge to balance the health in the body. It guides bodily processes towards some fixed points. These fixed points are also referred to as Attractor [31].
To maintain people's health, it is important to strengthen their homeodynamic properties. On the edge of chaos, a person must be able to optimally deal with what is asked of him. For this, the human system must be regularly emphasized. And if desired, Osteopathy (BOCF) can focus on improving the information structures and thus the homeodynamic possibilities.
In time the setpoint of attractors may change. This is published by Waddington and he named this process Homeorhesis [49]. For future research focused on biological processes like primary respiration concerning treatment, it can be important to check this at about the same time of the day as the intervention was carried out. Otherwise, you could come to the wrong conclusion because many attractors are periodic. That means the subsequent states of a system then show a repeating pattern, i.e. a state cycle. Many states in biological systems have repeating patterns because they are subject to all kinds of internal and external clocks. An important clock is the circadian biological clock. Another important constatation is that attractors change during life (homeorhresis) and because of this it is useless to compare PRM at different ages [49].
Transmutation is a term used in BOCF and described by Jealous. He describes an osteopathic treatment in which the system, the body, suddenly undergoes a major change. Jealous refers to such an abrupt change of state or phase as a Transmutation [43]. What exactly happens in a Transmutation is clarified by looking at it from a dynamical systems viewpoint.
A system can have one attractor for a group of variables, but it is also possible that there is more than one. In that case, there are several so-called attractor basins. For example, it can be imagined that there is a basin with healthy states and a basin with pathological states. If there is a pathological state, one can try to realize a shift to a healthier state through treatment as demonstrated in figure 3.
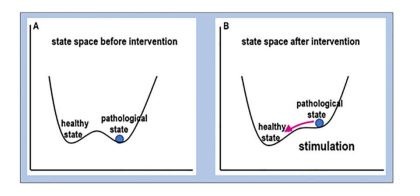 Figure 3: By stimulation, a pathological state can become instable and the system is driven towards a health state [50,51].
Figure 3: By stimulation, a pathological state can become instable and the system is driven towards a health state [50,51].
It can also happen that a system abruptly jumps from one attractor basin to another. In case of trauma, it can happen that very suddenly a change of state takes place from a more or less healthy state to a pathological one, but the opposite is also possible. Such a rapid change of state or phase is sometimes referred to as transmutation. This is consistent with the view of Jealous that a Transmutation refers to an osteopathic treatment in which the system, the body, suddenly undergoes a major change.
Searching for health
The goal of Cranial OMM is to find the problem, the dysfunction. This is based on the more mechanical view on the body which was described by Sutherland in his first period till 1943 [11]. The goal of the Biodynamic model in Osteopathy in the Cranial field (BOCC) is to look at the polyrhythms of the system and to see where health lies. Subsequently, the goal of the osteopath is to strengthen these rhythms so that the self-healing capacity of the body is enhanced [36]. There is significant and growing scientific support for this theory [52].
Conclusion
Cranial-OMM should implement the “five model” concept. The use of another exclusive model for the cranium is in contradiction with Still’s holistic principle. Dysfunction disrupts the self-healing ability and function of the cranium with its mechanical, neurological, respiratory, circulatory, metabolic, endocrine, and biopsychosocial aspects. Cranial research will have to clearly define which aspects of the cranium are investigated. For this purpose, the “five model” concept and the somatic dysfunction are clearly defined principles. In contrast, the “five model concept” is not a base for research of what primary respiration is.
That is the field of biodynamics. Biodynamics is difficult to comprehend because its properties and observed processes do not obey the linear laws of classical physics, but rather the laws of chaos and complex systems. Yet biodynamics is an essential part of osteopathy. Osteopathy is not osteopathy without it. It represents Still’s and Sutherland’s observations that the body has a self-healing ability inherent to life. The primary respiratory mechanism, the "Breath of Life", is a property of a body that has chaotic and complex adaptive properties. Searching for the foundation of these properties in the parts of the system makes no sense; they originate in the totality, in holism. Concepts as wholeness, neutral, synchronization, working with the health, and transmutation are explained by recent scientific insights from various disciplines.
Evidence-Based Practice, also in osteopathy, is based on 5 basic principles. 1) interaction between patient and osteopath, they jointly determine the best path to healing, 2) the approach must be multidisciplinary, 3) the healing method must be open to improvement, have a critical self-image, and eliminate cognitive dissonance, 4) Primum non nocere, 5) use technical insights and techniques to improve the treatment method.
Osteopathy should invest more in research, not least in the area of BOCF. It is clear that primary respiration and related terms can be scientifically substantiated and that there is room for future research. Research should not be limited to the anatomy and physiology of the cranium and its related structures. This is because the five-model concept is not sufficient for a good understanding. After all, attention must also be paid to the biodynamics aspects of osteopathy. In the latter it should be noted that research and support, and this may sound strange to osteopaths, will have to come from the field of mathematics, artificial intelligence, chaos theory, and complex systems thinking.
Osteopathy should start to communicate with these disciplines and discuss the possibilities for research. But we have to be humble and realize that we should not ask questions that we cannot answer, such as: “what is life?”. As stated in a statement attributed to Niels Bohr, one of the founders of quantum theory: "It is wrong to think that the task of physics is to find out how Nature is. Physics concerns what we can say about Nature.
References
- Jakel A, Hauenschild P (2012) A systematic review to evaluate the clinical benefits of craniosacral therapy. Complement Ther Med 20: 456-465.
- Magoun HI (1966) Osteopathy in the cranial field. Produced under the auspices of the Sutherland Cranial Teaching Foundation, teaching unit of the Cranial Academy. Journal Printing Co, Kirksville, USA.
- Upledger JE (1984) The Cranio-Sacral System: Clinical Applications and Research. Concepts and Mechanisms of Neuromuscular Functions 66-70.
- Hayden EC, Lumly A (2008) Osteopathy for children. Elizabeth C Hayden, England, UK.
- Guillaud A, Darbois N, Monvoisin R, Pinsault N (2016) Reliability of Diagnosis and Clinical Efficacy of Cranial Osteopathy: A Systematic Review. PLoS One 11: 0167823.
- Cerritelli F, Pizzolorusso G, Renzetti C, D'Incecco C, Fusilli P, et al. (2013) Effectiveness of osteopathic manipulative treatment in neonatal intensive care units: protocol for a multicentre randomised clinical trial. BMJ Open 3: 002187.
- King HH (2012) Cranial osteopathic manipulative medicine's growing evidence base. J Am Osteopath Assoc 112: 9.
- Jakel A, Hauenschild P (2011) Therapeutic effects of cranial osteopathic manipulative medicine: a systematic review. J Am Osteopath Assoc 111: 685-693.
- Rasmussen TR, Meulengracht KC (2020) Direct Measurement of the Rhythmic Motions of the Human Head Identifies a Third Rhythm. Journal of Bodywork and Movement Therapies 26: 24-29.
- Bordoni B (2019) The Benefits and Limitations of Evidence-based Practice in Osteopathy. Cureus 11: 6093.
- McPartland JM, Skinner E (2005) The biodynamic model of osteopathy in the cranial field. Explore (NY) 1: 21-32.
- Sutherland WG, Gregory MK (1948) The cranial bowl : a treatise relating to cranial articular mobility, cranial articular lesions and cranial technic. Free Press Company, USA.
- Bordoni B, Walkowski S, Ducoux B, Tobbi F (2020) The Cranial Bowl in the New Millennium and Sutherland's Legacy for Osteopathic Medicine: Part 2. Cureus 12: 10435.
- Moskalenko YE, Frymann V, Weinstein GB, Semernya VN, Kravchenko TI, et al. (2001) Slow Rhythmic Oscillations within the Human Cranium: Phenomenology, Origin, and Informational Significance. Human Physiology 27: 171-178.
- Nelson KE, Sergueef N, Lipinski CM, Chapman AR, Glonek T (2001) Cranial rhythmic impulse related to the Traube-Hering-Mayer oscillation: comparing laser-Doppler flowmetry and palpation. J Am Osteopath Assoc 101: 163-173.
- Mills MV, Henley CE, Barnes LLB, Carreiro JE, Degenhardt BF (2003) The use of osteopathic manipulative treatment as adjuvant therapy in children with recurrent acute otitis media. Arch Pediatr Adolesc Med 157: 861-866.
- Becker RE, Brooks RE (2000) The stillness of life: the osteopathic philosophy of Rollin E Becker DO. Stillness Press, Portland, USA.
- Chila A (2012) Foundations of Osteopathic Medicine. Wolters Kluwer, Netherlands.
- Hruby RJ, Tozzi P, Lunghi C, Fusco C (2017) The five osteopathic models: rationale, application, integration: from an evidence-based to a person-centered osteopathy. Handspring Publishing, Scotland, UK.
- Kuchera ML, Kuchera WA (1994) Osteopathic considerations in systemic dysfunction. Greyden Press, Columbus, Ohio, USA.
- Kales S (2017) Osteopathie in het craniaal gebied: 1 minuut voor 12. de osteopaat 2017:1-6.
- Bordoni B, Walkowski S, Ducoux B, Tobbi F (2020) The Cranial Bowl in the New Millennium and Sutherland's Legacy for Osteopathic Medicine: Part 1. Cureus 12: 10410.
- Nelson KE, Sergueef N, Glonek T (2006) Recording the rate of the cranial rhythmic impulse. J Am Osteopath Assoc 106: 337-341.
- Jealous J (1997) Jim Jealous, DO. Healing and the natural world. Interview by Bonnie Horrigan. Altern Ther Health Med 3: 68-76.
- Jealous JS, Trafeli RM (2000) The biodynamics of osteopathy. James Jealous, Farmington, USA.
- England JL (2013) Statistical physics of self-replication. J Chem Phys 139: 121923.
- Langton C (1992) Life at the edge of chaos Artificial life 2: the proceedings of an interdisciplinary workshop on the synthesis and simulation of living systems held February, 1990 in Santa Fe, New Mexico / editors Christopher G. Langton ... [et al.].
- Waldorf MM (1992) Complexity - The emerging science at the edge of order and chaos. Simon Schuster, USA.
- Rickles D, Hawe P, Shiell A (2007) A simple guide to chaos and complexity. J Epidemiol Community Health 61: 933-937.
- Swanson LT, Prasad T, Conboy L (2019) Complex Adaptive Systems Theory and Inter-Rater Reliability: Proposed Answers to Challenging Questions. J Altern Complement Med 25: 1074-1076.
- Lloyd D, Aon MA, Cortassa S (2001) Why homeodynamics, not homeostasis? Scientific World Journal 1: 133-145.
- Ewen HH, Kinney J (2014) Application of the model of allostasis to older women's relocation to senior housing. Biol Res Nurs 16: 197-208.
- Moser M, Fruhwirth M, Penter R, Winker R (2006) Why life oscillates--from a topographical towards a functional chronobiology. Cancer Causes Control 17: 591-599.
- Terzis G, Arp R (2011) Information and Living Systems. The MIT Press, USA.
- Moser M, Fruhwirth M, Kenner T (2008) The symphony of life. Importance, interaction, and visualization of biological rhythms. IEEE Eng Med Biol Mag 27: 29-37.
- Liem T, Moser M (2016) Biologische Rhythmen und ihre Bedeutung für die Osteopathie. Osteopathische Medizin 17: 22-26.
- Koepchen HP, Abel HH, et al. (1987) Integrative neurovegetative and motor control: phenomena and theory. Funct Neurol 2: 389-406.
- Fultz NE, Bonmassar G, Setsompop K, Stickgold RA, Rosen BR (2019) Coupled electrophysiological, hemodynamic, and cerebrospinal fluid oscillations in human sleep. Science 366: 628-631.
- George J (2019) ‘Waves of CSF Flow Into the Brain During Sleep’. MedPage Today, USA.
- Stankovski T, Pereira T, McClintock PVE, Stefanovska A (2019) Coupling functions: dynamical interaction mechanisms in the physical, biological and social sciences. Philos Trans A Math Phys Eng Sci 377: 20190039.
- Koestler A (2016) The Ghost in the machine. Erscheinungsort nicht ermittelbar: Last Century Media.
- Martin A, Mora GG, Méndez GD, Alba A, Méndez MO (2015) Non-linear analysis of EEG and HRV signals during sleep. Conf Proc IEEE Eng Med Biol Soc 2015: 4174-4177.
- Jealous J (2015) An osteopathic Odyssey. Tame Prepress, USA.
- Cerritelli F, Chiacchiaretta P, Gambi F, Ferretti A (2017) Effect of Continuous Touch on Brain Functional Connectivity Is Modified by the Operator's Tactile Attention. Front Hum Neurosci 11:
- Beseme S, Bengston W, Radin D, Turner M, McMichael J (2018) Transcriptional Changes in Cancer Cells Induced by Exposure to a Healing Method. Dose Response 16: 1559325818782843.
- Moran RW, Gibbons P (2001) Intraexaminer and interexaminer reliability for palpation of the cranial rhythmic impulse at the head and sacrum. J Manipulative Physiol Ther 24: 183-190.
- Bechtel W (2010) How can philosophy be a true cognitive science discipline? Top Cogn Sci 2: 357-366.
- Liem T, Heede PVD (2017) Foundations of Morphodynamics in Osteopathy: an Integrative Approach to Cranium, Nervous System, and Emotions. Handspring Publishing Limited, UK.
- Gare A (2017) Chreods, homeorhesis and biofields: Finding the right path for science through Daoism. Prog Biophys Mol Biol 131: 61-91.
- Ros T, Baars BJ, Lanius RA, Vuilleumier P (2014) Tuning pathological brain oscillations with neurofeedback: a systems neuroscience framework. Front Hum Neurosci 8: 1008.
- Pfister JP, Tass PA (2010) STDP in Oscillatory Recurrent Networks: Theoretical Conditions for Desynchronization and Applications to Deep Brain Stimulation. Front Comput Neurosci 4: 22.
- Petersen A (1963) The Philosophy of Niels Bohr. Bulletin of the Atomic Scientists 19: 8-14.
Citation: Zweedijk RJ, Oosten DV (2021) Osteopathy in the Cranial Field from a Systems Theory Perspective. J Altern Complement Integr Med 7: 197.
Copyright: © 2021 Rene J Zweedijk, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.