Ovarian Remnant Syndrome: A Case Report
*Corresponding Author(s):
Leila Cristina SoaresDepartment Of Gynecology, Pedro Ernesto University Hospital, Rio De Janeiro State University, Rio De Janeiro, Brazil
Tel:+55 88564796,
Email:lcs1507@yahoo.com.br
Abstract
Keywords
INTRODUCTION
We report an unusual case of ORS successfully treated with Gonadotropin-releasing Hormone agonist (GnRHa) in association with gabapentin.
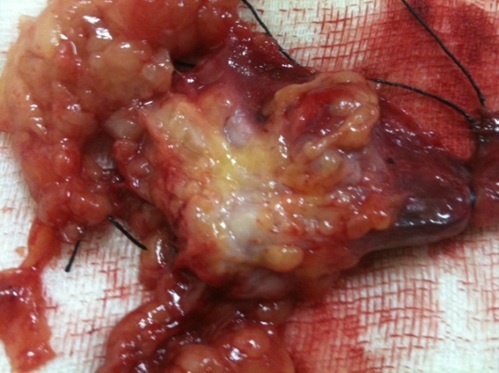
CASE REPORT
DISCUSSION
Ovarian remnant syndrome results from an unintentionally incomplete oophorectomy. In most patients, it seems that ORS results from an incidental implantation of ovarian tissue rather than an incomplete excision of a lesion [2].
Symptoms most often occur within the first 5 years of a previous surgery, although reports have shown patients whose initial surgeries were more than 20 years ago [1].
Dense periovarian adhesions and ovarian enlargement can make the identification of ovarian tissue difficult, and they are considered the predisposing factors of this disease. Both of those factors are present in severe endometriosis, the most typical preexisting disease [1]. The risk factors include pelvic inflammatory disease and adhesion [2].
The recurrence of pelvic symptoms is associated with the development of a hormonally functional follicular or corpus luteum cyst within the ovarian fragment, or with reactivation of endometriosis [3].
When the remaining ovary continues to produce sex steroids, the FSH levels remain low. Although the absence of this finding does not rule out the diagnosis, FSH levels <40 IU/dL indicate the presence of an ovarian remnant. A definitive diagnosis involves histologic confirmation of ovarian tissue obtained from the subsequent surgery [1].
The main treatment is surgery. Moreover, excision of remnant tissue requires retroperitoneal dissection [1]. Ovarian fragments may be difficult to localize, and reappearance of new fragments is possible. Ovulation-inducing drugs administered before surgery have been successful in stimulating the enlargement of such fragments, facilitating their location and removal [3].
Most clinical treatments do not seem to relieve symptoms and are often directed toward ovarian suppression. These include oral contraceptives such as danazol, GnRHa, and progestins [1].
Clinical treatments may increase the risk of ovarian cancer. There are controversies about the value of prophylactic oophorectomy in women with no increased risk for ovarian cancer. Epidemiological evidence suggest that annually about 1,000 cases of ovarian cancer are prevented for every 300,000 oophorectomies performed at the time of an elective hysterectomy in women over 40 years [4]. However, the risk of a woman with BRCA-1/BRCA-2 mutations developing ovarian cancer over a lifetime ranges from 16% to 54% [5]. If some ovary tissue is left in this population, there is a significant risk of ovarian cancer and clinical treatment is not indicated.
Gabapentin, a synthesized form of gamma-aminobutyric acid, an inhibitory neurotransmitter, is being increasingly prescribed for chronic pelvic pain and requires titration to achieve an efficacious dose [6]. Chronic gabapentin exposure reduces calcium currents because it binds to the α2δ-1 subunit of calcium channels. As voltage-gated calcium channels regulate various actions in the body, subtypes modulating pain are reduced [7]. In this case, it was used in association with a GnRHa with appreciable pain relief.
A medline search with the terms “remnant ovarian syndrome and gabapentin” revealed no previous reports about the use of gabapentin for ovarian remnant syndrome.
CONCLUSION
REFERENCES
- Kho RM, Abrao MS (2012) Ovarian remnant syndrome: etiology, diagnosis, treatment and impact of endometriosis. Curr Opin Obstet Gynecol 24: 210-214.
- Chao HA (2008) Ovarian remnant syndrome at the port site. J Minim Invasive Gynecol 15: 505-507.
- Rana N, Rotman C, Hasson HM, Redwine DB, Dmowski WP (1996) Ovarian remnant syndrome after laparoscopic hysterectomy and bilateral salpingo-oophorectomy for severe pelvic endometriosis. J Am Assoc Gynecol Laparosc 3: 423-426.
- Shoupe D, Parker WH, Broder MS, Liu Z, Farquhar C, et al. (2007) Elective oophorectomy for benign gynecological disorders. Menopause 14: 580-585.
- Finch A, Beiner M, Lubinski J, Lynch HT, Moller P, et al. (2006) Salpingo-oophorectomy and the risk of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1 or BRCA2 Mutation. JAMA 296: 185-192.
- Horne AW, Critchley HO, Doust A, Fehr D, Wilson J, et al. (2012) GaPP: a pilot randomised controlled trial of the efficacy of action of gabapentin for the management of chronic pelvic pain in women: study protocol. BMJ Open 2.
- Yan PZ, Butler PM, Kurowski D, Perloff MD (2014) Beyond neuropathic pain: gabapentin use in cancer pain and perioperative pain. Clin J Pain 30: 613-629.
Citation: Soares LC, de Souza RJ, Brollo JLA (2016) Ovarian Remnant Syndrome: A Case Report. J Reprod Med Gynecol Obstet 1: 002.
Copyright: © 2016 Leila Cristina Soares, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.