Pattern of Patients Presenting As Vertigo to the Opd Services at a Tertiary Care Hospital in Kashmir: A Hospital Based Cross-Sectional Study
*Corresponding Author(s):
Rouf Hussain RatherCommunity Medicine Specialist, Directorate Of Health Services, Kashmir, India
Tel:7006826153,
Email:rouf.rather86@gmail.com
Abstract
Background: Vertigo is a symptom of vestibular dysfunction with a sensation of motion (most commonly rotational motion). It is one of the common presenting complaints in primary care institutions and emergency departments. Different words are used by different patients about the type of motion being perceived. Vertigo affects both men and women & all age groups. Diagnosis of the underlying disease demands that the complaint of vertigo be analyzed correctly.
Objectives: To determine the 1. Associated presenting symptoms, 2. Pattern of diseases & 3. Risk factors of Vertigo among patients attending the OPD services at a Tertiary Care Hospital in Kashmir. METHODS: A cross-sectional Study was conducted among the patients attending the OPD services of the Post Graduate Department of Otorhinolaryngology and Head and Neck surgery (ORL AND HNS), Government SMHS Hospital Srinagar for a period of 18 months from May 2020 up to October 2021. All the patients of peripheral vertigo attending the ENT OPD in the age group of 21 to 70 years of age of either sex were included. Patients of Central vertigo, Severe Cervical Spinal disease, Uncontrolled Hypertension and active Heart ailments were excluded.
Results & Discussion: 68 patients (61.8%) were females while as 42 patients (38.2%) were males. Majority of patients presented as Vertigo associated with change in position (41.8%) followed by Vertigo associated with change in position & Nausea vomiting (20.9%); Vertigo & Tinnitus (10.9%) & Vertigo & Nausea vomiting (9.1%). Vertigo associated with Change in position was the most common symptom present in 62.7% followed by Nausea/Vomiting (30%). Mean age of participants was 43.4 years with an SD of 10.2 years. The minimum age was 22 years & maximum age was 70 years. Out of 110 patients in this study 75 Patients (68.2%) had BPPV, 30 Patients (27.3%) had Meniere's disease & only 5 Patients (4.5%) had Vestibular neuritis. The mean age was highest among patients of Meniere's disease (49.50 Years), followed by patients of Vestibular neuritis (44.80 Years) & BPPV (40.85 Years); and this difference was statistically significant as the p value was less than 0.05. Vertigo with change in position was specifically associated with BPPV, while as Vertigo with Tinnitis/ Aural Fullness/ Fluctuating hearing was specifically associated with Meniere's disease. Vertigo with Nausea and vomiting was specifically associated with Vestibular neuritis. All these associations were statistically significant with a p value of <0.001. The Vertigo of BPPV presented for Seconds, the Vertigo of Meniere's disease presented for Minutes and Hours; & the Vertigo of Vestibular Neuritis presented for days.
Conclusion: This study was devised to determine the pattern of patients presenting as vertigo to the OPD services at government SMHS hospital Srinagar. A total of 110 patients aged 22 to 70 years of age of either sex presenting with the complaint of vertigo were included in the study. Vertigo associated with change in position was the most common presentation & BPPV was the most common diagnosis (68.2%) followed by Meniere's disease (27.3%). Vertigo with change in position was specifically associated with BPPV, while as Vertigo with Tinnitis/ Aural Fullness/ Fluctuating hearing was specifically associated with Meniere's disease. The Vertigo of BPPV usually presented for Seconds, the Vertigo of Meniere's disease for Minutes to Hours & that of Vestibular Neuritis for days.
Keywords
BPPV; Meniere’s disease; Presenting Symptoms; Vertigo
Introduction
Vertigo is a symptom of vestibular dysfunction with a sensation of motion (most commonly rotational motion). It is one of the common presenting complaints in primary care institutions and emergency departments [1]. Vertigo is defined as the hallucination of movement, either of self (subjective) or the environment (objective). Different words are used by different patients about the type of motion being perceived which include Bouncing, Oscillating, Staggering, Swimming, Twisting Rolling, Spinning, Rocking, Lightheadedness, Imbalance, Floating, Fainting, Falling [2].
In a healthy person spatial orientation is largely an automatic but complex process. Continued sensory monitoring assesses the position of the body in space in relation to the surrounding environment. The five sensory modalities (vision, vestibular sensation, proprioception, touch and pressure, and hearing) constantly sample position and motion around the body. Normally the brain integrates the input from each of these sensory modalities giving a comprehensive image of position and motion in the space. This process enables us to maintain balance, move around and interact with other objects. When the orienting image is not reliable, we become uncertain of the position and the result is a sensation of spinning or vertigo. For the most part they are benign but always there is a possibility that they signal a neurological disorder [3].
Vertigo affects both men and women but is about two to three times more common in women than men [1]. It affects all age groups. In younger people the most common cause is middle ear pathology while as in case of elderly people a specific assessment is needed. It has been associated with various co-morbid conditions, including depression and cardiovascular disease as well. Prevalence of vertigo increases with increase in age and varies depending on the underlying diagnosis. It is estimated that 1-year prevalence of vertigo is about 5% and an annual incidence is 1.4%. Dizziness including vertigo affects about 15% to over 20% of adults yearly [4]. For benign paroxysmal positional vertigo, the one-year prevalence is about 1.6%, and it is less than 1% for vestibular migraine. The impact of vertigo should not be underestimated as majority of affected people have an interruption in daily activities, including employment and the need for additional medical attention.
Any central or peripheral lesion caused by a dysfunction in the vestibular system leads to vertigo. The Benign Paroxysmal Positional Vertigo [BPPV] and Meniere’s disease result from calcium deposits or debris in the posterior semicircular canal and cause frequent transient episodes of vertigo lasting a few minutes or less. The patients with BPPV only experience vertigo but the patients with the Meniere’s disease often experience tinnitus, hearing loss and aural fullness in addition to vertigo [1].There is an increased volume of endolymph in the semicircular canals that causes symptoms in Meniere’s disease.
Acute labyrinthitis and vestibular neuritis are two distinct causes of peripheral vertigo. Some other causes include Herpes zoster opticus, Cholesteatomas peri lymphatic fistula, etc. [1].
Central etiologies of vertigo should always be considered in the differential diagnoses. Ischemic or hemorrhagic strokes are life-threatening and must be ruled out by history, physical and other diagnostic tests if warranted. Others include tumors, such as brainstem glioma, medulloblastoma, and a vestibular schwannoma, which can lead to sensorineural hearing loss as well as vertiginous symptoms. Vestibular migraines are a common central cause of vertigo. Finally, multiple sclerosis has been associated with both central and peripheral causes of vertigo. [1-5].
Other causes include medication-induced vertigo and psychologic disorders, including mood, anxiety, and somatization [1].
Aims and Objectives
- To determine the associated presenting symptoms of vertigo among patients presenting as vertigo to the OPD services at a Tertiary Care Hospital in Kashmir.
- To determine the pattern of diseases in vertigo among patients presenting as vertigo to the OPD services at a Tertiary Care Hospital in Kashmir.
- To determine the risk factors of Vertigo among patients attending the OPD services at a Tertiary Care Hospital in Kashmir.
Materials and Methods
The present study was conducted in the Post Graduate Department of Otorhinolaryngology and Head and Neck surgery (ORL AND HNS), Government SMHS Hospital Srinagar, which caters patients from whole of the Kashmir division.
Study Design
This cross-sectional Study was conducted among the patients attending the said hospital.
Study Period
The study was done for a period of 18 months from May 2020 up to October 2021.
Study Participants
All the patients of peripheral vertigo attending ENT OPD of Unit 3 of the Department during the study period.
Inclusion Criteria
- Patients 21 to 70 years of age of either sex presenting with peripheral vertigo.
Exclusion Criteria
- Patients of Central vertigo.
- Patients of vertigo with Severe Cervical Spinal disease, Uncontrolled Hypertension and active Heart ailments.
Sample Size
A minimum of 100 patients were planned to be taken for the study. All the patients presenting with vertigo to the OPD services of the concerned Unit of Department during the study period were considered for study. After taking an informed written consent, such cases were screened for inclusion and exclusion criteria. Only those patients who gave the consent & fulfilled the criteria were taken into the study. Thus a total of 110 patients were taken for the study.
Observations And Results
68 patients (61.8%) were females while as 42 patients (38.2%) were males. Mean age of participants was 43.4 years with an SD of 10.2 years (Tables 1 &2). The minimum age was 22 years & maximum age was 70 years
|
Gender |
Frequency |
Percent |
|
Female |
68 |
61.8 |
|
Male |
42 |
38.2 |
|
Total |
110 |
100.0 |
Table 1: Distribution of patients according to gender.
|
Clinical Presentation |
Frequency |
Percent |
|
Vertigo associated with change in position |
46 |
41.8 |
|
Vertigo associated with change in position & Nausea vomiting |
23 |
20.9 |
|
Vertigo & Tinnitus |
12 |
10.9 |
|
Vertigo & Nausea vomiting |
10 |
9.1 |
|
Vertigo, Aural Fullness & Tinnitus |
9 |
8.2 |
|
Vertigo, Fluctuating hearing & Tinnitus |
5 |
4.5 |
|
Vertigo & Aural Fullness |
4 |
3.6 |
|
Vertigo, Tinnitus & Decrease Hearing during vertigious sensation |
1 |
0.9 |
|
Total |
110 |
100.0 |
Table 2: Distribution of patients according to their clinical presentation.
Majority of patients presented as Vertigo associated with change in position (41.8%) followed by Vertigo associated with change in position & Nausea vomiting (20.9%); Vertigo & Tinnitus (10.9%) & Vertigo & Nausea vomiting (9.1%). Vertigo was present in all the patients (Figure 1).
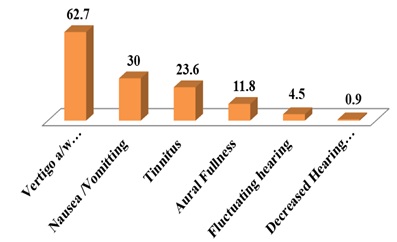 Figure 1: Bar Chart depicting distribution of symptoms in percentages.
Figure 1: Bar Chart depicting distribution of symptoms in percentages.
Vertigo associated with Change in position was the most common symptom present in 62.7% followed by Nausea/Vomiting (30%), Tinnitis (23.6%) & Aural Fullness (11.8%) (Figure 2).
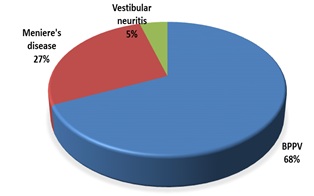 Figure 2: Pie Chart depicting distribution of Diagnosis.
Figure 2: Pie Chart depicting distribution of Diagnosis.
Out of 110 patients in this study 75 Patients (68.2%) had BPPV, 30 Patients (27.3%) had Meniere's disease & only 5 Patients (4.5%) had Vestibular neuritis (Table 3).
|
Gender |
Diagnosis |
Total |
||
|
BPPV |
Meniere's disease |
Vestibular neuritis |
||
|
Female |
49 (71.1%) |
17 (25%) |
2 (2.9%) |
68 (100%) |
|
Male |
26 (61.9%) |
13 (31%) |
3 (7.1%) |
42 (100%) |
|
Total |
75 (68.2%) |
30 (27.3%) |
5 (4.5%) |
110 (100%) |
Table 3: Relationship between Diagnosis and Gender.
Chi square: 1.74 P Value : 0.4
Among females 71.1% had BPPV, 25% had Meniere’s disease and 2.9% had Vestibular neuritis, while as among males 61.9% had BPPV, 31% had Meniere’s disease and 7.1% had Vestibular neuritis. This difference in the distribution of various diseases between females & males was statistically insignificant with a p value of 0.4 (Table 4).
|
Parameter |
Diagnosis |
||
|
BPPV (75) |
Meniere's disease (30) |
Vestibular neuritis (05) |
|
|
Mean Age in Years |
40.85 |
49.50 |
44.80 |
|
St Deviation |
9.86 |
9.24 |
5.36 |
Table 4: Age distribution among study participants according to final diagnosis.
p Value < 0.001
The mean age was highest among patients of Meniere's disease (49.50 Years), followed by patients of Vestibular neuritis (44.80 Years) & BPPV (40.85 Years); and this difference was statistically significant as the p value was less than 0.05 (Table 5).
|
Gender |
N |
Mean Age in Years |
Std. Deviation |
Mean Difference in Age in Years |
p Value |
|
Females |
68 |
42.94 |
11.02 |
-1.18 |
.539 |
|
Males |
42 |
44.12 |
8.85 |
Table 5: Age distribution among study participants according to gender.
The mean age of Males (44.12 Years) was more than that of females (42.94 Years), though this difference was statistically not significant because p Value was more than 0.05 (Table 6).
|
Presenting Symptoms |
Diagnosis |
Total |
||
|
BPPV |
Meniere's disease |
Vestibular neuritis |
||
|
Vertigo associated with change in position |
46 |
0 |
0 |
46 |
|
Vertigo associated with change in position & Nausea vomiting |
23 |
0 |
0 |
23 |
|
Vertigo & Nausea vomiting |
5 |
0 |
5 |
10 |
|
Vertigo & Aural Fullness |
1 |
3 |
0 |
4 |
|
Vertigo & Tinnitus |
0 |
12 |
0 |
12 |
|
Vertigo, Aural Fullness & Tinnitus |
0 |
9 |
0 |
9 |
|
Vertigo, Fluctuating hearing & Tinnitus |
0 |
5 |
0 |
5 |
|
Vertigo, Tinnitus & Decrease Hearing during vertigious sensation |
0 |
1 |
0 |
1 |
|
Total |
75 |
30 |
5 |
110 |
Table 6: Relationship between Diagnosis and Presenting Symptoms.
Chi square: 157.5; P Value: < 0.001
Vertigo with change in position was specifically associated with BPPV, while as Vertigo with Tinnitis/ Aural Fullness/ Fluctuating hearing was specifically associated with Meniere's disease. Vertigo with Nausea and vomiting was specifically associated with Vestibular neuritis. All these associations were statistically significant with a p value of < 0.001 (Table 7).
|
Characteristic |
Type |
Diagnosis |
p Value |
||
|
BPPV |
Meniere's disease |
Vestibular neuritis |
|||
|
Vertigo |
Present |
75 |
30 |
5 |
*** |
|
Fluctuating hearing |
Present |
0 |
5 |
0 |
0.003 |
|
Absent |
75 |
25 |
5 |
||
|
change in position |
Present |
69 |
0 |
0 |
0.000 |
|
Absent |
6 |
30 |
5 |
||
|
Aural Fullness |
Present |
1 |
12 |
0 |
0.000 |
|
Absent |
74 |
18 |
5 |
||
|
Tinnitus |
Present |
0 |
26 |
0 |
0.000 |
|
Absent |
75 |
4 |
5 |
||
|
Decrease Hearing during vertigious sensation |
Present |
0 |
1 |
0 |
0.32 |
|
Absent |
75 |
29 |
5 |
||
|
Nausea /Vomitting |
Present |
28 |
0 |
5 |
0.000 |
|
Absent |
47 |
30 |
0 |
||
Table 7: Relationship between different symptoms & Diagnosis.
Fluctuating hearing & Tinnitus were present exclusively in 5 cases & 26 cases of Meniere's disease, while as Aural Fullness in 12 cases of Meniere's disease. Similarly, change in position was present exclusively in 69 cases of BPPV. Nausea /Vomiting were more prevalent in Vestibular neuritis. All these associations were statistically significant with a p value of
|
Nystagmus |
Diagnosis |
Total |
||
|
|
||||
|
BPPV |
Meniere's disease |
Vestibular neuritis |
||
|
|
|
|
||
|
Present |
75 |
0 |
5 |
80 |
|
Absent |
0 |
30 |
0 |
30 |
|
Total |
75 |
30 |
5 |
110 |
Table 8: Relationship between Diagnosis and Nystagmus.
Chi square: 95.4, P Value < 0.001
Nystagmus was present in all the 75 cases of BPPV & in all the 5 cases of Vestibular neuritis; while as it was absent in all the 30 cases of Meniere's disease. These associations were statistically significant with a p value of less than 0.001 (Table 9).
|
Duration of Vertigo |
Diagnosis |
Total |
||
|
BPPV |
Meniere's disease |
Vestibular neuritis |
||
|
Seconds |
73 |
0 |
0 |
73 |
|
Minutes |
2 |
19 |
0 |
21 |
|
Hours |
0 |
11 |
0 |
11 |
|
Days |
0 |
0 |
5 |
5 |
|
Total |
75 |
30 |
5 |
110 |
Table 9: Relationship between Diagnosis and Duration of symptoms.
Chi square: 210.7 P Value < 0.001
The Vertigo of BPPV presented for Seconds in 73 patients and for minutes in 2 patients, the Vertigo of Meniere's disease presented for Minutes in 19 patients and for Hours in 11 patients; & the Vertigo of Vestibular Neuritis presented for days in all the 5 patients. This pattern of duration of symptoms was statistically significant with a p value of less than 0.001.
Discussion
Gender Distribution
Among the study participants 68 patients (61.8%) were females while as 42 patients (38.2%) were males. Vertigo is usually found more commonly among females than males and many studies across the globe have found similar results. The mean age of Males (44.12 Years) was more than that of females (42.94 Years), though this difference was not statistically significant. Among females 71.1% had BPPV, 25% had Meniere’s disease and 2.9% had Vestibular neuritis, while as among males 61.9% had BPPV, 31% had Meniere’s disease and 7.1% had Vestibular neuritis. This difference in the distribution of various diseases between females & males was statistically insignificant. Jan Bermeister et al [6] conducted a study titled “Prevalence, demographics, and clinical characteristics of vertigo disorders in a specialized multidisciplinary outpatient clinic” to determine clinical features and demographic factors characteristic of specific diagnoses and their specific subjective burden. From March 2010 till December 2013, 8182 patients were included in the study. They found that out of 8182 patients, 5659 patients were females (69.2), while as 2523 patients were males (30.8); which are quite similar to our findings. Bas Donmesi et al [7] conducted a study titled “Etiological and Demographic Characteristics of Patients with Vestibular Symptoms, Retrospective Analysis” which was published in Journal of Ankara University Faculty of Medicine in the year 2020. This study aimed to understand etiological and demographic characteristics of patients with vestibular symptoms. A Retrospective analysis of medical profiles of patients who suffered from vertigo and/or dizziness and sought medical advice from Ankara University ?bn-i Sina Hospital otorhinolaryngology Department, Hearing, Speaking and Balance Disorders Center between September 2018 and September 2019 was performed. A total of 444 patients between the age of 6 and 89 years were included in the study. Disregarding age groups and underlying cause, it was observed that women were more frequently affected by vertigo/dizziness than men. Thus the results of these studies are very similar to our results.
Age Distribution
Mean age of participants was 43.4 years with an SD of 10.2 years. The minimum age was 22 years & maximum age was 70 years. The mean age was highest among patients of Meniere's disease (49.50 Years), followed by patients of Vestibular neuritis (44.80 Years) & BPPV (40.85 Years); and this difference was statistically significant with a p Value of less than 0.001. [6] Conducted a study titled “Prevalence, demographics, and clinical characteristics of vertigo disorders in a specialized multidisciplinary outpatient clinic” to determine clinical features and demographic factors characteristic of specific diagnoses and their specific subjective burden. From March 2010 till December 2013, 182 patients were included in the study. They found that the Mean age of patients was 56.3 years (range 10 to 96 years) with an SD of 17.6 years. They also found that there was a considerable variation of mean age between different types of diagnoses which was statistically significant. These results are quite similar to our findings. The mean age of our study was 43.4 years which is lower than the mean age which Jan Bermeister et al [6] found (56.3 years). The reason could be the fact that our study was conducted during the Pandemic of COVID-19 and old aged people were reluctant to visit the OPDs of our hospital for the fear of contracting the COVID-19. Thus the mean age of patients has been lower than the expected & also lower than some other studies.
Presenting Symptoms
Majority of patients presented as Vertigo associated with change in position (41.8%) followed by Vertigo associated with change in position & Nausea vomiting (20.9%); Vertigo & Tinnitus (10.9%) & Vertigo & Nausea vomiting (9.1%). Vertigo was present in all the patients. Vertigo associated with Change in position was the most common symptom present in 62.7% followed by Nausea/Vomiting (30%), Tinnitis (23.6%) & Aural Fullness (11.8%). Vertigo with change in position was specifically associated with BPPV, while as Vertigo with Tinnitis/ Aural Fullness/ Fluctuating hearing was specifically associated with Meniere's disease. Vertigo with Nausea and vomiting was specifically associated with Vestibular neuritis. All these associations were statistically significant with a p value of <0.001. Fluctuating hearing & Tinnitus were present exclusively in 5 cases & 26 cases of Meniere's disease respectively, while as Aural Fullness in 12 cases of Meniere's disease. Similarly, change in position was present exclusively in 69 cases of BPPV. Nausea /Vomiting were more prevalent in Vestibular neuritis. All these associations were statistically significant with a p value of <0.001. Christopher W Cooper et al [8] mentioned in their article titled “Vestibular neuronitis: a review of a common cause of vertigo in general practice” published in the British Journal of General Practice in the year 1993, that Vestibular neuritis is characterized by the acute onset of vertigo, nausea and vomiting, in the absence of hearing loss or tinnitus. The disease follows a benign course of two days to six weeks & following the acute attack, mild transitory episodes of dizziness may recur over a period of 12 to 18 months. Two-third of patients (66.4%) presented with duration of Vertigo in seconds, 19.1% presented with duration of Vertigo in minutes, while as 10% presented with duration of Vertigo in Hours & only 4.5% in days. The Vertigo of BPPV presented for Seconds in 73 patients and for minutes in 2 patients, the Vertigo of Meniere's disease presented for Minutes in 19 patients and for Hours in 11 patients; & the Vertigo of Vestibular Neuritis presented for days in all the 5 patients. This pattern of duration of symptoms was statistically significant with a p value of less than 0.001. Elaine K. Luo et al [9] published an article titled “How Long Does Vertigo Last?” in which they found that the vertigo of BPPV lasts for less than a minute (that is for seconds), while as the vertigo of Meniere’s disease lasts for minutes, sometimes up to hours. These observations are much similar to our observations in the study. Nystagmus was present in 72.7% of patients. Nystagmus was present in all the 75 cases of BPPV & in all the 5 cases of Vestibular neuritis; while as it was absent in all the 30 cases of Meniere's disease. These associations were statistically significant with a p value of less than 0.001. Johkura et al [10] published their study titled “Positional nystagmus in patients with chronic dizziness” in the Journal of Neurology, Neurosurgery and Psychiatry. They found that 61% of their participants with chronic dizziness had positional nystagmus. This result of 61% is quite comparable with our result of 72.7%.
Distribution of different Diagnoses of Vertigo
Out of the 110 patients included in the study, 75 (68.2%) had BPPV, 30 (27.3%) had Meniere's disease and 05 (4.5%) had Vestibular neuritis. Many studies have shown similar distribution of different diagnosis among patients of Vertigo with BPPV being the most frequent diagnosis. Lee AT et al [11] mentioned in their article titled “Diagnosing the cause of vertigo: a practical approach” that for peripheral vertigo, the most common cause is benign paroxysmal positional vertigo. Bas Donmesi et al [7] conducted a study titled “Etiological and Demographic Characteristics of Patients with Vestibular Symptoms, Retrospective Analysis” where in a total of 444 patients between the age of 6 and 89 years were included in the study. The most frequent cause of vertigo/dizziness was benign paroxysmal positional vertigo (59.23%) followed by unilateral/bilateral vestibular hypofunction (20.72%), central pathologies (14.63%), Meniere’s disease (3.60%) and vestibular neuritis (1.80%). They concluded that the most common diagnosis was benign paroxysmal positional vertigo. Jan Bermeister et al [6] found in their study titled “Prevalence, demographics, and clinical characteristics of vertigo disorders in a specialized multidisciplinary outpatient clinic” that the five most common diagnoses were phobic postural vertigo, benign paroxysmal positional vertigo, vestibular neuritis, psychogenic vertigo and Ménière’s disease. Thus the results of both these studies are very much similar to the results of our study with respect to the relative proportion of different diagnoses of Vertigo.
Conclusion
Vertigo is a symptom of vestibular dysfunction with a sensation of motion, whose underlying cause needs to be elucidated so that proper management is planned. It is one of the common presenting complaints in primary care institutions and emergency departments. Diagnosis of the underlying disease demands that the complaint of vertigo be analyzed correctly.
This study was devised to determine the pattern of patients presenting as vertigo to the OPD services at government SMHS hospital Srinagar. A total of 110 patients aged 22 to 70 years of age of either sex presenting with the complaint of vertigo were included in the study.
Vertigo associated with change in position was the most common presentation & BPPV was the most common diagnosis (68.2%) followed by Meniere's disease (27.3%). Vertigo with change in position was specifically associated with BPPV, while as Vertigo with Tinnitis/ Aural Fullness/ Fluctuating hearing was specifically associated with Meniere's disease
The Vertigo of BPPV usually presented for Seconds, the Vertigo of Meniere's disease usually presented for Minutes to Hours & the Vertigo of Vestibular Neuritis usually presented for days.
References
- Labuguen RH (2006) Initial evaluation of vertigo. Am Fam Physician 15: 244-251.
- Walter G, Robert B, Fenichel DGM, Jankovic J (2004) neurology in clinical practice. 18: 233-246.
- Allan HR, Brown RH (2005) Adams and Victor’s principles of neurology 15: 246-268.
- Vitte E, Sémont A (1995) Assessment of Vestibular Function by Video-nystagmoscopy. Journal of Vestibular Research 5: 377-383.
- Pula JH, Newman-Toker DE, Kattah JC (2013) Multiple sclerosis as a cause of the acute vestibular syndrome. J Neurol 260: 1649-1654.
- Burmeister J, Bock E, Gerwig M, Frings M, Harbeck DA, et al. (2015) Prevalence, demographics, and clinical characteristics of vertigo disorders in a specialized multidisciplinary outpatient clinic. Neurology 84: 322.
- Dönmesi B, Olan S, Demografik HE (2020) Etiological and Demographic Characteristics of Patients with Vestibular Symptoms, Retrospective Analysis. Journal of Ankara University Faculty of Medicine 73: 270-275.
- Cooper CW (1993) Vestibular neuronitis: A review of a common cause of vertigo in general practice. British Journal of General Practice 43: 164-167.
- Elaine K, Kimberly H (2019) How Long Does Vertigo Last. Healthline com.
- Johkura K, Momoo T, Kuroiwa Y (2008) Positional nystagmus in patients with chronic dizziness. Journal of Neurology Neurosurgery and Psychiatry 12: 1324-1326.
- Lee AT (2012) Diagnosing the cause of vertigo: A practical approach. Hong Kong Med J 18: 327-332.
Citation: Faroq N, Khan I, Iqbal H, Qazi SM, Hussain Dar N, et al. (2022) Pattern of Patients Presenting As Vertigo to the Opd Services at a Tertiary Care Hospital in Kashmir: A Hospital Based Cross-Sectional Study. J Community Med Public Health Care 9: 109.
Copyright: © 2022 Nisar Hussain Dar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.