Post Hematopoietic Stem Cell Transplant Revaccination Compliance
*Corresponding Author(s):
Enela AliajDepartment Of Pharmacy Practice, University Of Illinois At Chicago, Chicago, IL, United States
Tel:+1 6309014539,
Email:ealiaj3@uic.edu
Abstract
Purpose: The University of Illinois Hospital & Health Sciences System performs an average of 80 hematopoietic stem cell transplants each year. Several organizations throughout Europe and North America have established guidelines for preventing infectious complications after Hematopoietic stem cell transplant (HSCT). Consensus between these guidelines recommend revaccination of all HSCT recipients. The aim of this study is to define the appropriate vaccine schedule in the post-transplant setting based on current guidelines and review the vaccination compliance at UI Health through a retrospective chart review.
Methods: A retrospective chart review will be conducted on patients who received an HSCT at the University of Illinois Hospital & Health Sciences System between July 1st, 2015 to September 1st 2018. The study subjects’ immunization records will be compared to an immunization schedule created by study investigators. Current immunization guidelines were used to create this immunization schedule. The primary endpoint of this study is to analyze the percent compliance to current immunization guidelines. The secondary endpoints are to analyze the percent compliance to our ideal immunization schedule, explore reasons for non-compliance to vaccination recommendations, and evaluate the number of appointments needed to complete the patient’s vaccination course.
Results: There were 121 patients that met all inclusion and exclusion criteria. Only 40 patients received the full regimen of recommended vaccines recommended by the IDSA guidelines, giving a compliance rate of 33%. The average number of appointments to achieve full compliance was four. When compare to the author generated ideal immunization schedule there was 45% compliance with the average time between the first and second found of vaccines at 2.2 months and 6.3 months for the second and third round of vaccines. Analysis of why patients missed immunizations showed it was due to current immunosuppressive therapy, missed in clinic, or referral to primary care physician.
Conclusion: Despite guideline recommendations for vaccination of HSCT recipients, many institutions find this task to be problematic. The overall vaccination compliance rate for UIH was determined to be 33% with a majority of the missed vaccinations due to current immunosuppressive therapy, referral to PCP, or simply missed in clinic.
Keywords
Hematopoetic immunizations, Infectious disease, Stem cell transplant, Vaccination
ABBREVIATIONS
CDC Center for Disease Control and Prevention
DTap Diptheria, Tetanus, Pertusis
GVHD Graft-versus-host disease
Hep B Hepatitis B
HIPAA Health Insurance Portability and Accountability Act
HSCT Hematopoietic Stem Cell Transplant
IDSA Infectious Diseases Society of America
MRN Medical Record Number
PCV13 Pneumococcal 13 valent
PPSV23 Pneumococcal 23 valent
PCP Primary Care Physician
PHI Protected Health Information
UIH University of Illinois Hospital & Health Sciences System
INTRODUCTION
The risk of preventable infectious diseases has greatly decreased with the introduction of vaccines. Vaccination induces active immunity through the development of antibodies in the recipient and is expected to withstand over a period of time. [1,2] However, Hematopoietic stem cell transplant (HSCT) recipients are unique in that they experience a loss of immunity after transplantation.
A HSCT involves the transfusion of stem cells to reestablish hematopoietic function in patient whose immune system is damaged or defective. This procedure is often performed as part of therapy to eliminate a bone marrow infiltrative process, such as leukemia, or it can be used to correct congenital immunodeficiency disorders. Patients who have received a HSCT are immunocompromised for at least 6-12 months post-transplant making them vulnerable to preventable infectious disease. Even after immune reconstitution has occurred these patients often do not have continued immunity to pathogens for which immunizations have been previously given. Several factors can affect the severity of immunity loss including the patient’s pre-transplant immunity, the patient’s underlying hematological condition, and the chemotherapeutic and immunosuppressive regimens that the patient has undergone [2]. Therefore, in order to decrease the risk of preventable infectious diseases it is vital that HSCT recipients are re-immunized.
Several organizations throughout Europe and North America established guidelines for preventing infectious complications after HSCT. These published guidelines replaced the guidelines from the CDC recommending earlier vaccinations for these patients. Unfortunately, these guidelines made no recommendations regarding dosing intervals and only stated the optimal time to initiate each vaccine. However, in 2005, the European guidelines did state recommendations regarding dosing intervals. In an effort to standardize recommendations for immunizations, recent guidelines from IDSA endorsed specific recommendations for vaccination of immunocompromised hosts, specifically including HSCT recipients [3-5].
Despite the actuality of these guidelines, execution is far from perfect and many HSCT recipients still remain unvaccinated or receive an incomplete schedule of vaccinations. A study group from the MD Anderson Cancer center conducted a three-part survey to assess physician compliance and execution of current guideline recommendations. The first part of the study was a physician survey assessing the clinicians’ knowledge toward vaccination guidelines after HSCT and asking them about their own practices. Of the physicians that responded, 96% stated that they were familiar with post-HSCT vaccination protocols. Part 2 of the study looked at the institution’s pharmacy database to see the number and type of vaccines administered after the patient’s stem cell transplant. Of all the patients analyzed, only 38% of patients received the first series of vaccinations by the 6-month post-HSCT period. Part 3 of the study performed a retrospective chart review of the non-vaccinated cases in order to see what some of the reasons were for non-compliance. The study found that the non-vaccination was partially due to relapse of disease, hospitalization around the time the vaccines were due, and recent immunosuppressive therapy restricting vaccine administration [6].
Currently at UIH we perform about 80 HSCT per year but there are no established guidelines for post-HSCT re-vaccination. Compliance continues to be a problem in many institutions. Through this quality improvement study, we hope to find out the vaccination compliance to current guidelines at UIH for our post-HSCT recipients.
METHODS
This project was a single-center retrospective chart review that included patients that received a HSCT at UIH between July 1st, 2015 to September 1st, 2018. A patient list was generated from Cerner, the electronic medical database at our institution. Patients were included in the study if they met the following inclusion criteria: age ≥ 18 years old, HSCT at UIH after July 1st, 2015, and patient receives their follow-up care at UIH. Patients who met any of the following exclusion criteria were not enrolled in the study: age ≤ 18 years old, patients who were incarcerated throughout the study period, patient who are or become pregnant throughout the study period, patients that have experienced a failure of HSCT or death, or patients with acute Graft versus host-disease (GVHD).
The following data points were collected on eligible patients and entered into REDCap: patient’s medical record number, date of birth, gender, race, date of HSCT, type of HSCT, type and date of immunizations, number of appointments where immunizations were administered, and insurance type. Reasons for missed immunizations such as hospitalization when the vaccine was due, relapse of disease, immunosuppressive therapy, or any exclusionary lab values were also collected.
An ideal immunization schedule (Table 1) was created using current immunization guideline recommendations. Each study subjects’ immunization records were collected and compared to the ideal immunization schedule seen in table 1 and the IDSA guidelines. The primary endpoint of this study will be to analyze the percent compliance of our institution to the IDSA immunization guidelines. The secondary endpoints will include analyzing the percent compliance to the ideal immunization schedule described in table 1, explore reasons for non-compliance to vaccination recommendations, and evaluate the number of appointments needed to complete the patient’s vaccination course.
|
Months after HSCT |
|||
|
6 Months |
8 Months |
10 Months |
12 Months |
|
· PCV13 |
· PCV13 |
· PCV13 |
· PPSV23 |
|
· Haemophilus Influenzae |
· Haemophilus Influenzae |
· Haemophilus Influenzae |
|
|
Type B |
Type B |
Type B |
|
|
· DTaP |
· DTaP |
· DTaP |
|
|
· Hep B |
· Hep B |
· Hep B |
|
|
· Polio |
· Polio |
· Polio |
|
|
· Flu (annually) |
|||
Table 1: Ideal Immunization Schedule
Data will be assessed for normality, analyzed and characterized using descriptive statistics. All of the data analysis was performed utilizing excel.
RESULTS
There were 260 patients that received an HSCT at UIH during the study period. Of those patients, only 185 patients did not have relapse of disease or death. Further analysis showed that only 121 patients of those patient’s follow-up at UIH and will be included in the analysis of this study. The average age was 53 years old and 54% of the patients were male. The study group had a diverse population with only 27% Caucasian while 34% was African American, 5% Asian and 34% listed as other (including Hispanic). Autologous HSCT recipients accounted for 53% of the study group while 47% received allogeneic HSCT. The baseline demographic data can be seen broken down in table 2.
|
Characteristic |
% of pts (n=121) |
|
Age, years |
53.3 |
|
Gender |
|
|
Male |
54 |
|
Female |
46 |
|
Race |
|
|
Caucasian |
27 |
|
African American |
34 |
|
Asian |
5 |
|
Other |
34 |
|
Type of HSCT |
|
|
Autologous |
53 |
|
Allogeneic |
47 |
Table 2: Baseline Demographics
Of the 121 patients analyzed, only 40 individual patient records showed compliance to IDSA guidelines and had received the full regimen of recommended vaccinations. This means that UIH had a 33% compliance rate (Figure 1). When analyzing these patients, the average time to first vaccine was 11.3 months and the average number of appointments needed to complete the full vaccine regimen was four appointments. When looking at the individual years of vaccination compliance, a trend was discovered showing that guideline compliance was improving each year. In 2018, vaccination percent compliance was as high as 50%, as can be seen in Figure 2.
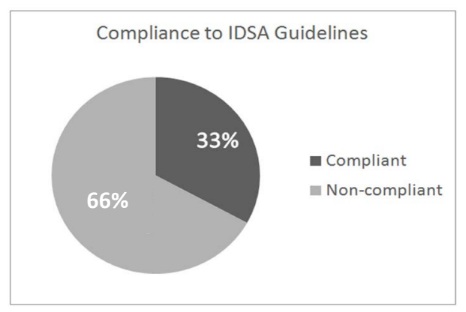 Figure 1: UIH Compliance to IDSA Guidelines
Figure 1: UIH Compliance to IDSA Guidelines
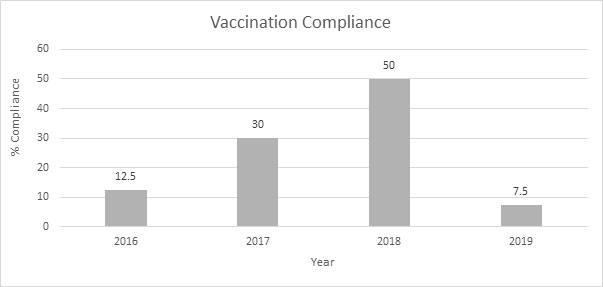 Figure 2: Vaccination Compliance throughout the Years
Figure 2: Vaccination Compliance throughout the Years
The patients that completed the full regimen of recommended vaccinations were compared to the ideal immunization schedule described in Table 1. Compliance rate to the ideal immunization schedule was 45% (Figure 3). Further analysis of this data showed that the average time between the first and second round of vaccines was 2.2 months. The average time between the second and third round of vaccines was 6.3 months.
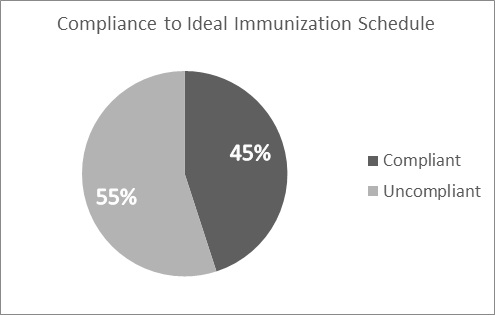 Figure 3: Compliance to Ideal Immunization Schedule
Figure 3: Compliance to Ideal Immunization Schedule
A majority of missed immunizations were due to immunosuppressive therapy (35.5%), missed in clinic (15.7%), referral to primary care physician (PCP) (14.9%), or insurance coverage (6.6%). A full summary of reasons for missed immunizations is depicted in Table 3. The vaccination compliance rate was also analyzed for patients that were referred to their PCP for re-immunization. Analysis of information obtained from the Illinois Immunization Registry showed a compliance rate of 38.9% (Figure 4).
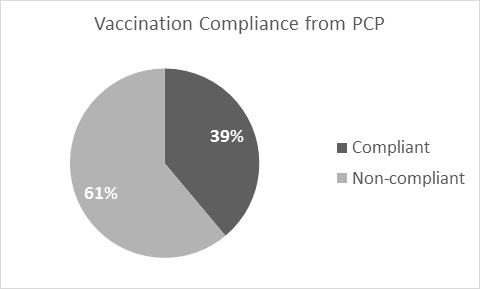 Figure 4: Vaccination Compliance from PCP
Figure 4: Vaccination Compliance from PCP
Table 3
|
Reasons for Missed Immunizations |
% of pts (n=121) |
|
Immunosuppressive Therapy |
35.5 |
|
Chronic GVHD |
14 |
|
Maintenance Chemotherapy |
21.5 |
|
Lab Values |
0.8 |
|
Insurance Coverage |
6.6 |
|
Hospitalization |
3.3 |
|
Other |
|
|
Referred to PCP |
14.9 |
|
Missed in Clinic |
15.7 |
DISCUSSION
Out of the 121 patients that met full inclusion criteria, only 40 patients received the full regimen of recommended vaccines by IDSA, resulting in a 33% compliance rate for UIH. The average time to first vaccine was on average 11.3 months. However, IDSA guidelines state that a patient is eligible for their first vaccine up to 6 months post-HSCT. Many factors could have affected the physicians’ decision to delay the start of re-immunization such as current immunosuppressive therapy. Patient chart review showed that 35.5% of patients missed immunizations due to immunosuppressive therapy; 14% were on immunosuppression for chronic GVHD and 21.5% were on maintenance chemotherapy. Physician vaccination noncompliance may also be due to uncertainty when it comes to vaccine effectiveness in post-HSCT patient, especially for those who are on maintenance immunosuppressive therapy. Many immunosuppressant agents contain the warning that the therapeutic effect of various vaccines many be diminished with concurrent use.
As seen in Figure 2, vaccination compliance is improving. However, 2019 only has a rate of 7.5% due to the study period and design. Throughout this study we did not analyze how many patients had received their first round of immunizations and were only looking at who complete the full immunization regimen. As a result, a majority of patients who received vaccinations in 2019 have yet to complete their full regimen and were not captured within the dataset. Furthermore, the average time to first vaccine was about one year, consequently a lot of the patients that received a HSCT toward the end of the study period have likely not even received their first round of vaccines yet and were not included in the dataset.
Patients that met compliance required an average of four appointments to complete the full vaccine regimen. This is the same number of appointments required for the ideal immunization schedule (Table 1). The average time between the first and second round vaccine was 2.2 months and the average time between the second and third vaccine round of vaccines was 6.3 months, again similar to the timeline described in the ideal immunization schedule (Table 1). This ensures that all the vaccines are being administered at one time and optimal patient convenience has been achieved.
There were a majority of reasons for missed immunizations discovered through the study. When it came to PCP referral, utilizing the Illinois Immunization Registry, patient’s immunization records could be accessed through the patients’ medical chart. Therefore, it can be seen if the patient’s PCP completed the full immunization schedule. However, delayed upload and vaccinations outside the state of Illinois could easily be missed and marked as non-compliance. The Illinois Immunization Registry was the only way to obtain patient immunization records outside of UIH and clear limitations of the registry lead to further limitations in this study. Furthermore, a large number of patients were lost to follow-up after the initiation of their vaccines. Thus, we were unable to see if these patients completed their vaccines at outside institutions, other than the data available through the Illinois Immunization Registry.
Over 15.7% of the missed immunization in the study were simple due to being missed in clinic. The implementation of a vaccine order set that will import all of the vaccine orders and schedule future appointments will hopefully improve the medical provider adherence to the vaccine schedule. Furthermore, only 6.6% of patients missed their immunizations due to insurance coverage. A majority of these patients experienced a delay in vaccine administration due to the requirement of prior authorization from the insurance company. There was no difference seen in insurance approval of vaccines between public and private insurance.
CONCLUSION
Despite guideline recommendations for vaccination of HSCT recipients, execution continues to be a problem for many institutions and many patients remain unvaccinated or receive an incomplete schedule of immunizations. The overall vaccination compliance rate for UIH was determined to be 33% with a majority of the missed vaccinations due to current immunosuppressive therapy, referral to PCP, or simply missed in clinic. Further immunization studies are needed to truly determine the efficacy of immunizations in patients receiving maintenance immunosuppressive therapy after transplantation. Increased provider and patient education on the importance of re-immunization to prevent fatal infections can expectantly lead to better adherence to immunization guidelines. Phase 2 of this project will be to implement a vaccine order set at UIH for the post-HSCT patient and see if that will improve immunization compliance.
REFERENCES
- Carpenter PA, Englund JA (2016) How I vaccinate blood and marrow transplant recipients. Blood 127: 2824-2832
- Chong PP, Avery RK (2017) A comprehensive review of immunization practices in solid organ transplant and hematopoietic stem cell transplant recipients. Clin Ther 39: 1581-1598.
- Rubin LG, Levin MJ, Ljungman P, et al. (2014) 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis 58: 309-318
- Ljungman P, Engelhard D, de la Camara R, et al. (2005) Vaccination of stem cell transplant recipients: recommendations of the infectious diseases working party of the EBMT. Bone Marrow Transplant 35: 737-746
- Ljungman P, Cordonnier C, Einsele J, et al. (2009) Vaccination of hematopoietic cell transplant recipients. Biol Blood Marrow Transplant 15: 1143-1238
- Ariza-Heredia EJ, Gulbis AM, Stolar KR, et al. (2014) Vaccination guidelines after hematopoietic stem cell transplantation: practitioners’ knowledge, attitudes, and gap between guidelines and clinical practice. Transpl Infect Dis 16: 878-886.
Citation: Aliaj E, Fleming PJ (2020) Post Hematopoietic Stem Cell Transplant Revaccination Compliance. J Pharmacol Pharmaceut Pharmacovig 4: 012.
Copyright: © 2020 Enela Aliaj, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.