Postpartum Pubic Symphysis Diastasis and the Role of Physiatry in Restoring Function: A Case Report
*Corresponding Author(s):
Anna MarkhDepartment Of Physical Medicine And Rehabilitation, Montefiore Medical Center, Bronx, NY, United States
Tel: +1 6463392303,
Email:abushkan@montefiore.org
Abstract
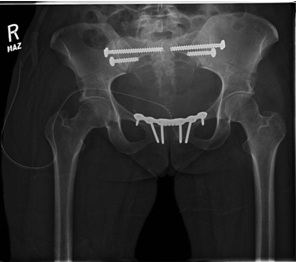
This case report demonstrates the course of a 36 year old Gravida4Parity3 (G4P3) female with no past medical history who sustained a pubic Symphysis Diastasis (SPD) after a vaginal delivery. Her initial postpartum pelvic X-ray showed a pelvic diastasis measuring approximately 2.3 cm wide. There was also a 5 mm vertical offset in the alignment of the pubic bones.
The patient was initially treated by orthopedics with an external fixator, however, after 6 weeks, the patient’s pain and disability did not improve. She was subsequently admitted for an elective ORIF of the pubic symphysis. The patient was admitted to acute rehabilitation for a comprehensive Physical Therapy/Occupational Therapy (PT/OT) program to improve her mobility, transfers, and ambulation. On physical examination, the patient had weakness in hip flexors and had limited strength in her quadriceps and hamstrings due to pain. Her range of motion in hip flexion was also limited due to pain. There were no neurological deficits. Prior to rehab, the patient needed assistance with transfers and ambulation. On discharge, the patient’s strength in her hip flexors improved and she was able to ambulate 150 feet with a rolling walker.
Postpartum pubic symphysis diastasis is a rare but potentially disabling condition. There is little information in the literature regarding the benefit of comprehensive rehabilitation in improving the clinical outcome. A therapy program tailored to address the pelvic floor muscles as well as core and lower extremity muscles may provide the most amount of benefit to improve the patient’s clinical outcome.
INTRODUCTION
Complete separation of the symphysis pubis during vaginal delivery is rare; reported prevalence ranges from one in 521 to one in 20,000 [2]. Causes for symphysis pubis diatasis include a difficult labor, cephalopelvic disproportion; multiparity; or an abnormal presentation of the infant. Symptoms may include pain and swelling. In some cases there is a visible deformity in the pelvic region or a clicking sound when the patient walks. Diagnosis can be made with an anteroposterior X-ray of the pelvis. Historically, most women were treated conservatively with bed rest and pelvic binders. More recently, invasive orthopedic treatments have been used if pain is significant or the diastasis fails to resolve [3]. There is limited literature available regarding the benefit of rehabilitation to treat this condition.
CASE DESCRIPTION

DISCUSSION
There are a number of variables thought to contribute to development of symphyseal separation. These include multiparity, fetal macrosomia, precipitous labor or rapid second stage of labor, intense uterine contractions, and previous pelvic pathology or trauma to the pelvic ring.
Clinical symptoms may be noted antepartum, during labor, or 24 to 48 hours postpartum and can include suprapubic pain with or without radiation to the legs, hips, or back, swelling, and difficulty walking. The physical exam may reveal tenderness at the symphysis pubis, edema, voluntary splinting of the legs, pain during hip flexion, a waddling or duck-like gait, and occasionally a palpable groove at the level of the symphysis pubis. These findings are not consistent and severity can vary from mild to disabling. Although the diagnosis can be made on clinical presentation and exam findings alone, radiological evaluation can be useful. However, the amount of symphyseal separation on X-ray does not always correlate with severity of symptoms or the degree of disability. In addition, it is quite difficult to draw meaningful conclusions from radiological separations because the true amount of physiologic separation and vertical movement of pubic rami during pregnancy is not clearly defined. Therefore, treatment is based on the severity of symptoms rather than the degree of separation as measured by imaging studies.
Treatment is often conservative management including pelvic support with a brace or girdle, ambulation with assistance or devices such as walkers, and graded exercise protocols [5]. Symptoms usually resolve in 6-8 weeks. Surgical intervention is rarely required but may be utilized in cases of inadequate reduction, recurrent diastasis, or persistent symptoms.
In 1997, Snow and Neubert performed a retrospective chart review of cases with a symptomatic pubic symphysis separation who had a therapeutic intervention including physical therapy, assistive devices, pelvic binders, and analgesics. The review suggested that nearly all cases resolved with conservative measures by 6 to 8 weeks postpartum. Among the patients undergoing orthopedic procedures, nearly all had separations of 4 cm or greater.
In 2011, Nitsche and Howell conducted a literature review and found 28 articles documenting 42 cases of peripartum pubic symphysis diastasis. They found that the clinical course can be quite variable. Time to ambulation ranged widely from as soon as 2 days to as long as 56 days (median 7 days). There was similar variability in the time to resolution of pain and disability, ranging from 6 weeks to more than 16 months (median 12 weeks). A substantial number of patients, 36%, underwent orthopedic interventions (external fixation or ORIF). Nearly all of the patients undergoing these orthopedic procedures had separations of 4 cm or greater (93%). Although many of the patients undergoing these procedures after failed conservative management experienced rapid improvement in their symptoms, it is difficult to assess the efficacy of these interventions due to the small numbers of cases. In fact, several of the patients undergoing internal or external fixationas a primary therapy experienced prolonged disability as well.
Physical therapy has been shown to be beneficial in some women suffering from SPD. Shim and Oh demonstrated a case report in which a 32 year old woman with SPD during labor underwent a therapeutic exercise program which consisted of abdominal stabilization and strengthening of the pelvic floor muscles, hip adductors, and extensors; training for bed mobility; and walking training with suitable aids [6]. The program was performed for 1-hour sessions, twice a day, for 2 weeks. Before the intervention, the patient was dependent on others for performing her daily activities owing to severe pain in the pelvic region. After the 2-week intervention, the interpubic distance was reduced by 36% (from 22 mm to 14 mm), and pain and functional disability were remarkably improved. The specific exercise protocol used can be found in Appendix 1.
APPENDIX 1
1.1. Exercise protocol
- Abdominal hollowing exercise:
- Starting position: Crook-lying position. Draw the navel gently toward the spine while maintaining a neutral pelvic position.
- Repetitions: Twenty repetitions of a 10-second hold
- Hip adductor and extensor muscles:
- Starting position: Supine with knees extended or Crook-lying position. For strengthening the hip adductor muscles, put a small, soft pillow between both knees, and then press the pillow with the knees together. To strengthen the hip extensor muscles, squeeze both buttocks at the same time.
- Repetitions: Twenty repetitions of a 10-second hold
- Pelvic floor muscles:
- Starting position: Crook-lying position. Squeeze to close around the openings.
- Repetitions: Twenty repetitions of a 10-second hold
- Rolling over:
- Starting position: Crook-lying position. Roll over to the right and left sides alternately, maintaining abdominal hollowing and contraction of the pelvic floor muscles. Keep knees together.
- Repetitions: Twenty repetitions for each side
- Getting up and down:
- Starting position: Supine with knees extended. Lie in the Crook-lying position with both knees bent, and then roll over to the right side. Lift the upper body using the arms, and sit on the edge of the bed with relaxed legs, keeping the knees close together. Reverse this procedure to lie down in bed. Repeat it on the left side.
- Repetitions: Twenty repetitions for each side
- Standing up from a chair:
- Starting position: Sitting in a chair. The patient wears a pelvic corset to support the weight loading to the pelvic ring. Place a walker in front of the patient. Ask the patient to hold the grips of the walker, and lean the trunk forward to stand up. Stand up with pushing the grips and then hold the standing position for 10 seconds, keeping the knees close together. Sit down.
- Repetitions: Twenty repetitions
- Walking training with a walker:
- Starting position: Standing. The patient wears a pelvic corset. Perform 10-m of walking training with a walker, taking small steps.
- Repetitions: Ten to Twenty repetitions
There have also been studies looking at exercise programs in general pregnancy-related pelvic girdle pain. Stuge et al., conducted a randomized controlled trial that evaluated a treatment program focusing on specific stabilizing exercises for patients with pelvic girdle pain after pregnancy [7]. Eighty-one women with pelvic girdle pain were assigned randomly to two treatment groups for 20 weeks. One group received physical therapy with a focus on specific stabilizing exercises. The other group received individualized physical therapy without specific stabilizing exercises. The specific stabilizing exercises included training of the transversely oriented abdominal muscles with coactivation of the lumbar multifidus at the lumbosacral region, training of the gluteus maximus, the latissimus dorsi, the oblique abdominal muscles, the erector spinae, the quadrates lumborum, and the hip adductors and abductors. After intervention and at 1 year post partum, the specific stabilizing exercise group showed statistically and clinically significant lower pain intensity, lower disability, and higher quality of life compared with the control group. The study concluded that an individualized treatment approach with specific stabilizing exercises appears to be more effective than non-specific physical therapy for women with pelvic girdle pain after pregnancy. More studies need to be done to see whether a similar exercise program with specific stabilizing exercises would benefit women with SPD as well.
There are several limitations in this case report. Although our patient showed improvement with a comprehensive rehabilitation program, the physiotherapy protocol accompanied surgical intervention and was not a sole treatment. We did not use an objective quality of life scale to quantify the patient’s improvement. We mainly used the Functional Independence Measure (FIM) scores, muscle strength, and the patient’s subjective assessments of pain to assess her outcome. We do not have long-term follow up of the patient’s outcome after discharge from the rehab unit.
CONCLUSION
REFERENCES
- Pedrazzini A, Bisaschi R, Borzoni R, Simonini D, Guardoli A (2005) Post partum diastasis of the pubic symphysis: a case report. Acta Biomed 76: 49-52.
- Kowalk DL, Perdue PS, Bourgeois FJ, Whitehill R (1996) Disruption of the symphysis pubis during vaginal delivery. A case report. J Bone Joint Surg Am 78: 1746-1748.
- Nitsche JF, Howell T (2011) Peripartum pubic symphysis separation: a case report and review of the literature. Obstet Gynecol Surv 66: 153-158.
- Snow RE, Neubert AG (1997) Peripartum pubic symphysis separation: a case series and review of the literature. Obstet Gynecol Surv 52: 438-443.
- Depledge J, McNair PJ, Keal-Smith C, Williams M (2005) Management of symphysis pubis dysfunction during pregnancy using exercise and pelvic support belts. Phys Ther 85: 1290-1300.
- Shim JH, Oh DW (2012) Case report: Physiotherapy strategies for a woman with symphysis pubis diastasis occurring during labour. Physiotherapy 98: 89-91.
- Stuge B, Laerum E, Kirkesola G, Vøllestad N (2004) The Efficacy of a Treatment Program Focusing on Specific Stabilizing Exercises for Pelvic Girdle Pain After Pregnancy: A Randomized Controlled Trial. Spine 29: 351-359.
Citation: Markh A, Stern M (2015) Postpartum Pubic Symphysis Diastasis and the Role of Physiatry in Restoring Function: A Case Report. J Phys Med Rehabil Disabil 1: 005.
Copyright: © 2015 Anna Markh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.