Pott's Puffy Tumor: A Rare Diagnosis
*Corresponding Author(s):
Maria Ventura NogueiraPediatrics Department, Hospital De Braga, Portugal
Email:mj.ventura.nogueira@gmail.com
Abstract
Pott’s puffy tumor consists of subperiosteal abscess of the frontal sinus wall associated with underlying osteomyelitis, which can appear as a rare complication of frontal sinusitis. We report the case of an 11-year-old girl who presented with a headache and sudden forehead swelling. Imaging evaluation revealed soft tissue abscess in the surroundings of the anterior plate of the frontal sinus and, later, osteomyelitis of the frontal bone, with no signs of intracranial complications. The patient was submitted to functional sinus surgery and surgical drainage of the abscess as well as prolonged antibiotic therapy, with good clinical recovery. Pott’s puffy tumor may be a result of an underdiagnosed or not adequately treated frontal sinusitis. This case highlights the importance of its earliest diagnosis, in order to prevent eventual life-threatening complications.
Keywords
CT scan; Drugs; Puffy tumor; Tumor
Introduction
Acute bacterial sinusitis is a relatively common diagnosis in the pediatric population, and, when properly diagnosed and treated, complications are rare [1]. It is defined by inflammation and secondary bacterial infection of the paranasal sinuses with clinical symptoms during less than 12 weeks [2]. Untreated or partially treated bacterial sinusitis can result in orbital, intracranial, systemic, or local complications - one of them is the Pott’s puffy tumor [1].
Pott’s puffy tumor was first described in the 18th century, by Sir Percival Pott, as a possible consequence of frontal head trauma. A few years later it was established its relationship with frontal sinusitis. Rarely can it also occur in association with drug use or frontal surgeries [3]. It consists of subperiosteal abscess of the frontal sinus wall with underlying osteomyelitis [4]. Clinically it can manifest as a forehead swelling, fever and headaches; with the current use of antibiotics, it’s a rare diagnosis nowadays [3]. Once Pott’s puffy tumor is suspected, an imaging study should be performed, as early as possible, since it is crucial to exclude potential life-threatening intracranial complications [3].
Case Description
A previously healthy 11-year-old girl was admitted to the pediatric emergency room for a three-week history of gradually increasing headache and a sudden-onset left forehead swelling since that day (Figure 1). No history of trauma or fever was reported. She was on a daily nonsteroidal anti-inflammatory drugs regimen with poor response.
 Figure 1: Left forehead swelling.
Figure 1: Left forehead swelling.
The physical examination revealed a tender left forehead swelling, with 5 cm of maximum diameter, soft to firm consistency with no fluctuation and a slight erythema but no other signs of skin inflammation (Figure 2). She also presented left periorbital edema that compromised the eye opening but did not affect the visual acuity. Nasal endoscopy revealed generalized nasal congestion, and once vasoconstrictors were applied, a purulent discharge from the left middle meatus was seen. The neurologic examination was normal.
 Figure 2: Left forehead swelling.
Figure 2: Left forehead swelling.
Investigations revealed leukocytosis (total white blood cells: 20,4 x109/L) with neutrophilic predominance (16,7 x109/L) and a C-reactive protein of 71,2 mg/L. A cranial and paranasal sinuses Computed Tomography (CT) scan with intravenous contrast was performed: extensive sinusitis of the left maxillary (Figure 3), ethmoidal and frontal sinus with diffuse soft-tissue swelling of the forehead and a soft tissue abscess in the surroundings of the anterior plate of the frontal sinus, with no signs of intracranial complications. The patient was admitted to the otorhinolaryngology department and started empirical antibiotic treatment with intravenous ceftriaxone (2 g/day, q12hr) and clindamycin (30 mg/kg/day, q8hr), intravenous corticosteroids and topical nasal treatment with corticoid, vasoconstrictors, and saline irrigations.
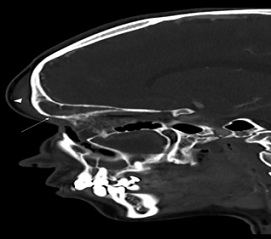 Figure 3: Sagittal CT of the paranasal sinuses demonstrating an opacified frontal sinus, erosion of the anterior table of the frontal sinus (arrow) and contiguous soft tissue swelling of the forehead (arrowhead).
Figure 3: Sagittal CT of the paranasal sinuses demonstrating an opacified frontal sinus, erosion of the anterior table of the frontal sinus (arrow) and contiguous soft tissue swelling of the forehead (arrowhead).
After 48 hours of treatment there were no signs of clinical improvement, and a re-evaluation CT scan of the paranasal sinus confirmed the growth of the abscess with a notorious liquid component (Figure 4), as well as osteomyelitis of the frontal bone, with no intracranial extension. These findings confirmed the diagnosis of Pott’s Puffy tumor. The patient underwent functional endoscopic sinus surgery: antrostomy, anterior ethmoidectomy and frontal sinus recess approach Draf I type with drainage of purulent content from the left maxillary sinus which culture revealed multi sensible streptococcus intermedius growth. The histologic exam reported an inflammatory process.
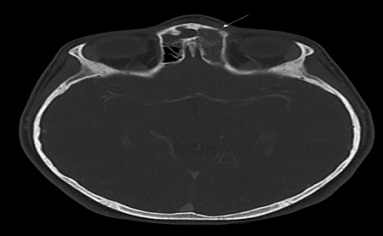 Figure 4: Axial CT demonstrating erosion of the anterior table of the frontal sinus (arrow) and no intracranial complications.
Figure 4: Axial CT demonstrating erosion of the anterior table of the frontal sinus (arrow) and no intracranial complications.
The patient had a full recovery and was discharged home after 14 days of intravenous ceftriaxone and clindamycin. The treatment was complemented at home with six weeks of oral amoxicillin 500 mg/clavulanic acid 125 mg, as well as corticosteroid withdrawal. On the three-months follow-up visit, the patient was asymptomatic and had no sequelae.
Discussion
Pott’s Puffy Tumor is a rare complication of misdiagnosed frontal sinusitis and consists of subperiosteal abscess overlying osteomyelitis of the frontal bone [5-7]. Although there are case reports in all age groups, this entity is more prevalent in adolescents [8], since at that age the flow rate of the diploic veins - which drain the frontal sinus - increases, facilitating the hematogenous spread of infections [9]. Frequently these infections are polymicrobial, with isolation of streptococci, staphylococci, and anaerobic bacteria, which demands antibiotic coverage for gram-positive and anaerobes [3]. In this case, empirical treatment with ceftriaxone and clindamycin was started, and later it was adjusted to the isolated microorganism, streptococcus intermedius.
Clinically this entity typically manifests with progressive frontal swelling, associated with headaches and eventually fever [3]. Other symptoms typical of bacterial sinusitis such as nasal discharge may be present [4]. Our patient mentioned a sudden-onset frontal swelling, which may indicate a misperception of the symptoms by the patient. Also, fever may not have been perceived, as she was taking nonsteroidal anti-inflammatory drugs on a daily fixed dose treatment regimen.
After clinical suspicion, the diagnosis is based on CT scan findings [5,9]. Intracranial or intraorbital suppurative complications should be excluded with a contrast-enhanced CT scan of the head, orbits, and sinuses [4]. The intracranial complications of Pott’s Puffy Tumor comprise meningitis, subdural and brain abscess, and are the most dangerous, so early diagnosis and prompt treatment are essential to avoid them [5,10]. Orbital complications may also occur if the inferior wall of the frontal sinus is involved [7]. In this case, re-evaluation CT already showed osteomyelitis of the frontal bone. There were no intracranial or orbital complications, since it was possible to avoid them with prompt intravenous antibiotics.
The standard of care consists of long-term broad-spectrum antibiotics in addition to surgical drainage [5,9]. Magnetic resonance (MRI) has greater ability to exclude possible intracranial complications and is particularly helpful in follow-up after medical or surgical management [3,7]. In our case, the patient’s full clinical recovery dismissed the need for a follow-up MRI.
Conclusion
A benign and common infection such as acute bacterial sinusitis can sometimes result in serious complications, if not properly diagnosed and treated. Pott’s puffy tumor, although rare, should not be forgotten. The early diagnosis and the exclusion of intracranial complications are of utmost importance. Empirical broad-spectrum antibiotics in addition to surgical drainage are the standard of care for this entity.
References
- Leung AK, Hon KL, Chu WC (2020) Acute bacterial sinusitis in children: An updated review. Drugs Context 9: 1-11.
- Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, et al. (2020) Executive summary of EPOS 2020 including integrated care pathways. Rhinology 58: 82-111.
- Silva ACV, Lins CM, Mendes RFA, Silva MHS, Alencar Neto JF, et al. (2022) Case report: Pott’s edematous tumor: Complicated frontal sinusitis-an unremembered diagnosis. Front Surg 9: 889463.
- Wald ER, Applegate KE, Bordley C, Darrow DH, Glode MP, et al. (2013) Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics 132: e262-80.
- Koltsidopoulos P, Papageorgiou E, Skoulakis C (2018) Pott’s puffy tumor in children: A review of the literature. Laryngoscope 130: 225-231.
- Heale L, Zahanova S, Bismilla Z (2014) Pott puffy tumour in a five-year-old girl. Can Med Assoc J 187: 433-435.
- Sharma P, Sharma S, Gupta N, Kochar P, Kumar Y, et al. (2017) Pott puffy tumor. Bayl Univ Med Cent Proc 30: 179-181.
- Brown TR, Campbell AJ, Blyth CC, Bowen AC (2017) Pott’s puffy tumour. J Paediatr Child Health. 53: 197.
- Kühn JP, Linsler S, Nourkami-Tutdibi N, Meyer S, Becker SL, et al. (2022) Pott’s puffy tumor: A need for interdisciplinary diagnosis and treatment. HNO 70: 8-13.
- Osei-yeboah C, Neequaye J, Bulley H, Darkwa A (2010) Osteomyelitis of the frontal bone. Ghana Med J 41: 88-90.
Citation: Nogueira VM, Ribeiro C, Miranda SB, Vilaça J, Abreu A, et al. (2023) Pott's Puffy Tumor: A Rare Diagnosis. J Med Stud Res 5: 021.
Copyright: © 2023 Maria Ventura Nogueira, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.