Preoperative Transarterial Embolization in the Treatment of Plexiform Neurofibroma: A Case Report and Literature Review
*Corresponding Author(s):
Reinaldo Tovo FilhoDepartment Of Dermatology, Institute Of Education And Research, Hospital Sírio Libanes, Sao Paulo, Brazil
Tel:+ 55 11 987441111,
Email:tovoclinic@uol.com.br
Abstract
Neurofibromatosis type 1 (NF1) is an autosomal dominant multisystem genodermatosis resulting from a mutation on chromosome 17q11.2, characterized by diverse clinical expression with involvement of the skin, nervous system, bones, eyes and other systems. Neurofibromas are tumors located along nerve bundles; when they become large, they are called plexiform neurofibromas. Complications of neurofibromas are rare, but include malignant transformation and potentially life-threatening hemorrhages. A comprehensive perioperative management, including arterial embolization of feeding vessels, is required in order to perform a safe surgical procedure and to reduce potential surgical complications. We report a case of a large plexiform neurofibroma on the right flank, treated in a two-stage approach: first, embolization with polyvinyl alcohol particles of the inferior epigastric, lumbar and superior gluteal arteries on the right and, second, 24 hours after embolization, exeresis of the lesion, which weighed 2.5 kg. Two years after surgery, the patient was asymptomatic, without tumor recurrence and with an important improvement in self-esteem and quality of life.
Keywords
Embolization; Neurofibromatosis; Plexiform neurofibromas; Surgery
Introduction
Neurofibromatosis type 1 (NF1), also known as Von Recklinghausen’s disease is an 40 autosomal dominant multisystem genodermatosis resulting from a mutation on chromosome 17q11.2, which encodes neurofibromin [1]. It is one of the most comom autosomal dominant disorders, with an estimated incidence of 1 in 2500 to 3300 live 43 births [2].
It is characterized by diverse clinical expression with involvement of the skin, nervous system, bones, eyes and other systems. The main cutaneous manifestations are Café-au-Lait spots, axillary freckles and neurofibromas [1]. Neurofibromas occurs in 26.7% of the cases, they are defined as tumors located along nerve bundles; when they become large, 48 they are called plexiform neurofibromas [1,3]. They often lack function and aesthetic value, thereby negatively impacting quality of life. Cases of lower extremity are less frequent than the ones located on the face and neck, and are extremely vascular [3].
Complications of neurofibromas are rare, but include malignant transformation in 2% of the cases and potentially life-threatening hemorrhages [2,3].
There is no specific treatment for NF1, and clinical manifestations are treated individually. Surgery is the preferred treatment for plexiform neurofibromas, but the significant vascularization of the tumor and the consequent possibility of large intraoperative hemorrhages make the procedure difficult [3]. Thus, preoperative embolization becomes useful to reduce potential surgical complications.
Case Report
We report the case of a 34-year-old female patient with NF1 with a large plexiform neurofibroma (39.5 x 20 x 15.7 cm) on the right flank, impairing appearance and mobility (Figure 1). High-frequency ultrasound (24 MHz) with Doppler flowmetry demonstrated a hyperechoic solid mass with irregular borders with multiple 64 hypoechogenic nodules and permeating large-caliber vascular pedicles. Due to the intense vascularization, angiotomography of the abdomen and pelvis was performed to characterize the arterial supply, and vascularization with multiple intercostal, lumbar, iliac and gluteal branches was observed. According to the clinical-radiological findings, a two-stage approach was planned: first, embolization with polyvinyl alcohol particles of the inferior epigastric, lumbar and superior gluteal arteries on the right (Figure 2), second, 24 hours after embolization, exeresis of the lesion, which weighed 2.5 kg (Figure 71 3). Arteriography performed before (A) and after (B) the embolization, demonstrating devascularization of the embolized region with preservation of the other non-target arterial branches. Anatomopathological examination and immunohistochemistry confirmed a non-malignant neurogenic tumour with degenerative atypia, confirming the diagnosis of neurofibroma. Intraoperative blood loss was moderate, but the haemoglobin drop from 14.2 g/dL to 8 g/dL on the day after the procedure, requiring transfusion of two packed red blood cell units. The patient was managed by a multidisciplinary team that included individuals from the Dermatology, Plastic Surgery and Interventional Radiology departments. Two years after surgery, the patient was asymptomatic, without tumor recurrence and with an important improvement in self-esteem and quality of life (Figures 3&4).
 Figure 1: Large plexiform neurofibroma (39.5 51 x 20 x 15.7 cm) on the right flank.
Figure 1: Large plexiform neurofibroma (39.5 51 x 20 x 15.7 cm) on the right flank.
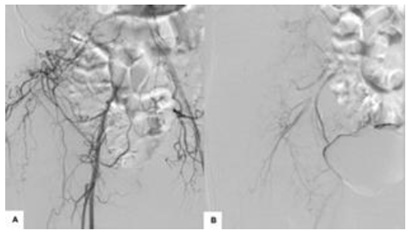 Figure 2: Intra operatory: embolization with polyvinyl alcohol particles of the inferior epigastric, lumbar and superior gluteal arteries on the right.
Figure 2: Intra operatory: embolization with polyvinyl alcohol particles of the inferior epigastric, lumbar and superior gluteal arteries on the right.
 Figure 3: Large plexiform neurofibroma (39.5 51 x 20 x 15.7 cm), which weighted 2.5kg.
Figure 3: Large plexiform neurofibroma (39.5 51 x 20 x 15.7 cm), which weighted 2.5kg.
 Figure 4: Plexiform neurofibroma. Patient before (A) and after two years (B) the treatment with surgery and embolization.
Figure 4: Plexiform neurofibroma. Patient before (A) and after two years (B) the treatment with surgery and embolization.
Discussion
Plexiform neurofibromas have variable clinical presentations, ranging from asymptomatic to invasive and disfiguring superficial lesions. In some cases, transformation to malignant tumors is observed [1]. Surgical intervention is important for histopathological diagnosis as well as for therapeutics, restoring appearance and function [3]. The intense vascularization and characteristic capillary fragility of the disease predisposes patients to a high risk of potentially fatal intraoperative haemorrhages. Therefore, preoperative embolization can be performed in an attempt to devascularize the area, reduce intraoperative bleeding and, consequently, achieve rapid haemostasis [4]. In the literature reports there are 9 cases of preoperative embolization followed by surgery in patients aged 15 to 55 years, 5 males and 4 females with plexiform neurofibromas, mainly located in the trunk. To minimize complications, it is important to properly select the material that will be used for embolization based on safety, efficacy, polymerization properties and ease of use [4]. Different embolization techniques were used by the authors [5-10], lyophilized dura mater strips, fascia lata strips, coil embolization, gelatine sponge, microsprings and an ethylene-vinyl alcohol copolymer. In the present case, polyvinyl alcohol was chosen as the embolizable particle, also used by Cavallaro, et al. and Vélez, et al. which was found to be safe and effective [5,6]. There is no consensus on the ideal interval between embolization and surgical resection. Littlewood et al. embolized a plexiform neurofibroma 3 weeks prior to surgery [7], with significant blood loss and the need for transfusion of 11 units of packed red blood cells. In our case, we performed selective embolization followed by surgery after 24 hours. This approach is important for reduction of flow in the vascular pedicles at the level of dissection and lowering the risk of adjacent tissue necrosis. Resection of plexiform neurofibromas is a difficult procedure due to the rich vascular proliferation, infiltration of deep planes and reconstruction of large areas. Therefore, adequate preoperative planning using new technologies combined with a multidisciplinary approach is important for achieving satisfactory results through functional restoration and improved appearance.
Conclusion
We describe our experience with a two-stage approach in the treatment of a large plexiform neurofibroma, using current technologies; preoperative embolization, ultracision scapel and high frequency ultrasound. The adequate preoperative management and a multidisciplinary collaboration are important in reducing life threatening complications during the surgical exeresis of the tumor and in ensuring a safe surgical procedure. This patient was successfully treated, without any recurrence after two years of follow-up, and with an important improvement in self-esteem and quality of life.
References
- Antônio JR, Goloni-Bertollo EM, Trídico LA (2013) Neurofibromatose: Histórico cronológico e aspectos atuais. An Bras Dermatol 88: 333-347.
- Chen L, Guo C, Song X, Yan C, Hu X (2018) Long-Term Results for a One-Stage Surgery Technique for Patients With Craniofacial Plexiform Neurofibroma. J Craniofac Surg 29: 746-750.
- Kolker S, Wunder JS, Roche-Nagle G (2015) Hybrid resection of a giant thigh plexiform neurofibroma. Int J Surg Case Rep 8: 1-4.
- Tomei KL, Gupta V, Prestigiacomo CJ, Gandhi CD (2013) Spontaneous Hemorrhage of a Facial Neurofibroma: Endovascular Embolization Before Surgical Intervention. J Craniofac Surg 24: 514-517.
- Cavallaro G, Pedullà G, Crocetti D, Giustini S, Calvieri S, et al. (2012) Vacuum-assisted closure treatment of leg skin necrosis after angiographic embolization of a giant plexiform neurofibroma. G Chir 33: 239-242.
- Vélez R, Barrera-Ochoa S, Barastegui D, Pérez-Lafuente M, Romagosa C, et al. (2013) Multidisciplinary Management of a Giant Plexiform Neurofibroma by Double Sequential Preoperative Embolization and Surgical Resection. Case Reports in Neurological Medicine 2013: 987623.
- Littlewood AHM, Stilwell JH (1983) The vascular features of plexiform neurofibroma with some observations on the importance of pre-operative angiography and the value of pre-operative intra arterial embolization. Br J Plast Surg 36: 501-506.
- Jones RG, Kiatisevi P, Morris DC, Munket PL, Clarkson PW, et al. (2010) Intravascular embolisation and surgical resection of a giant neurofibroma with intratumoural haemorrhage. The British Journal of Radiology 83: 225-229.
- Tanaka J, Kuramochi A, Nishi N, Yuasa M, Heshiki A (2005) Preoperative Transarterial Embolization Enhances the Surgical Management of Diffuse Plexiform Neurofibroma: A Case Report. Cardiovasc Intervent Radiol 28: 686-688.
- D’Arpa S, Tuttolomondo A, Melloni C, Cordova A, Moschella F (2014) Management of large dorsal diffuse plexiform neurofibroma. Eur J Plast Surg 37: 349-352.
Citation: Filho RT, Carnevale FC, Curi TZ, Tovo FM, Cestari SCP, et al. (2020) Preoperative Transarterial Embolization in the Treatment of Plexiform Neurofibroma: A Case Report and Literature Review. J Clin Dermatol Ther 6: 063.
Copyright: © 2022 Reinaldo Tovo Filho, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.