Preparing Surgical Residents for the Fundamentals of Laparoscopy Surgery (FLS) Skills Examination Using Gamification: The March Madness Method
*Corresponding Author(s):
Luv HajirawalaLouisiana State University School Of Medicine, New Orleans, Louisiana, United States
Email:lhajir@lsuhsc.edu
Abstract
Objectives
The purpose of this study is to assess any progress of General Surgery residents on the Fundamentals of Laparoscopic Surgery (FLS) skills while participating in a competitive tournament and to determine their satisfaction in participating in the tournament.
Methods
General Surgery residents at a single academic center were scheduled to participate in a competition, based on the five FLS manual skills. Five months prior to the competition, residents recorded baseline times for each FLS skill. Residents were notified of the competition and encouraged to practice.
The tournament was structured akin to and timed to coincide with the NCAA Men’s basketball “March Madness” tournament. It was structured as a single elimination tournament, with two residents competing against one another in all five of the FLS manual skills. The times were tabulated and then combined at the conclusion for one total time. The resident with the fastest total time advanced in the tournament. One round of matches was performed each week.
Results
Individual resident times improved from baseline in all five events. Resident’s times improved in every event. First year residents, with little prior exposure to laparoscopic surgery demonstrated the greatest improvement.
Conclusion
Using an internal competition, resident times on FLS tasks improved significantly and the incorporation of gamification was well received by the residents.
Keywords
Competition; Fundamentals of Laparoscopic Surgery (FLS); Gamification; Simulation
Introduction
It is well established that simulation helps novice learners develop surgical skills. Simulation is especially well suited to laparoscopic or robotic techniques, where the operation is viewed on a screen, looking at a site that is different from where the action is occurring. This requires the surgeon to perform actions with greater visual feedback coupled with decreased haptic sensation. Simulation enables practicing and learning some of the realities of laparoscopic procedures such as working with altered depth and using the longer instruments that are required for laparoscopic surgery. It is preferable for novice trainees to learn basic techniques in a structured, supervised environment outside of the operating suite, prior to attempting on patients.
Since the introduction of the Fundamentals of Laparoscopic Surgery (FLS) program in 2004, it has become the gold standard for both the education and the assessment of surgical trainees for basic laparoscopic skills [1]. It has been validated in numerous studies and is a required part of the curriculum for surgical training and mastery is required prior to obtaining certification by the American Board of Surgery [2,3]. There are multiple simulation devices and simulation products that have been brought to the marketplace. These have demonstrated additional expense, but there is no evidence that any additional educational benefit is gained with this added cost. A simple box-training tool remains the standard for practicing FLS Skills [4,5].
The time available to trainees is limited and there are numerous competing interests and demands placed upon them. Despite the benefits of simulation, there is difficulty for the trainee to find either the time or the motivation to regularly participate in simulation activities. Gamification is the use of game design elements in non-game contexts [6]. Games are enjoyable and by incorporating some of the enjoyable aspects of games into non-game contexts such as education, these activities can be more enjoyable and could theoretically stimulate increased time in the activity. The addition of games into education has been evaluated with inconsistent results, however [7].
The purpose of this study is to assess the progress of general surgery residents on FLS skills while participating in a competitive tournament to evaluate if the addition of gamification techniques to FLS improves performance. In addition, the residents were queried regarding the amount of time they spent practicing as well as their thoughts on any influence that the gamification elements had on their desire to practice simulation as well as any perceived influence on their laparoscopic skills.
Methods
General Surgery residents at a single academic center were scheduled to participate in a competition based on the five FLS manual skills. Five months prior to the competition, all residents recorded baseline times for each of the FLS skills. Residents were notified of the competition and encouraged to practice.
The tournament was designed as single elimination for all rounds. FLS rules were posted in the simulation room and were reviewed prior to every match. Two residents were scheduled to compete for the best time in each of the five FLS manual skills. Cumulative time for all five events, including penalty time for mistakes, was used to determine the winner. The winning resident advanced in the tournament. Residents were seeded by year level, so that more senior trainees were matched against more junior ones. One full elimination round was completed each calendar week to allow residents to schedule their match at a mutually conducive time, as well as to allow any time to practice between each round. An attending staff surgeon or an impartial observing resident proctored each match with one proctor per competitor to allow for accurate timing and evaluation of tasks.
Minor deviations from the standard FLS rules were required to create a more balanced competition and to assess accuracy as well as speed. Deviations occurred in Circle Cut and the intracorporeal knot tying tasks. For the circle cut exercise, the “practice gauze” with two solid circles with an area of 0.5 cm in between the circles was used, instead of the single circle used in the actual FLS examination. For the intracorporeal knot exercise, residents were not required to pass the needle between hands to tie. Participants were allowed to hold the needle in the same hand for all three throws of the knot. Penalties of 10 seconds were added for deviations or errors during the competition in each event consistent with the standard FLS rules.
The FLS tournament brackets were initially posted on the Monday following the release of the men’s NCAA “March Madness” basketball schedule. The FLS tournament then roughly mirrored the basketball schedule. As the tournament progressed, the evolving brackets were updated. After the competition, an anonymous survey was given to all participants inquiring about their opinion of the tournament and whether the experience was positive, and if it should be continued in the future.
Results
17 general surgery residents participated in the FLS March Madness competition. At baseline, PEG transfer, circle cut, endoloop placement, extra-corporeal suture, and intra-corporeal suture, took 71, 225, 93, 215 and 261 seconds, respectively. Time to complete each given task decreased through the first three rounds across all categories (Figure 1). Time improvement from baseline to first round in percent for PEG transfer, circle cut, endoloop placement, extra-corporeal suture and intra-corporeal suture, were 14%, 52%, 32%, 37% and 46%, respectively. The maximum time improvement from baseline was seen during round three for each activity (Figure 1). The maximum time improvement from baseline for PEG transfer, circle cut, endoloop placement, extracorporeal-suture and intra-corporeal suture, was 39%, 73%, 53%, 64% and 70%, respectively. Maximum improvement from previous recorded time was seen between the baseline and the first round. The time to complete the exercises did not improve between the third and fourth rounds.
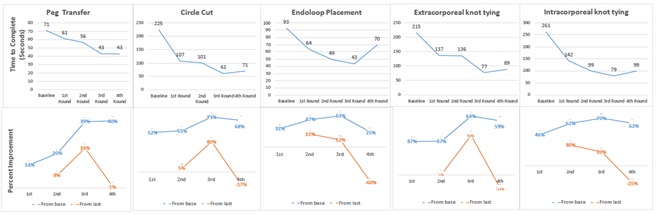 Figure1: (Top) Average time to complete task at baseline and each round of competition in seconds. (Bottom) Improvement in time (in percent) from baseline, as well as from previous round of the competition.
Figure1: (Top) Average time to complete task at baseline and each round of competition in seconds. (Bottom) Improvement in time (in percent) from baseline, as well as from previous round of the competition.
At baseline, the residents performed each task faster than the interns, with the exception of endoloop placement. Interns experienced a greater time improvement from baseline to round one in all activities, except endoloop placement (Figure 2).
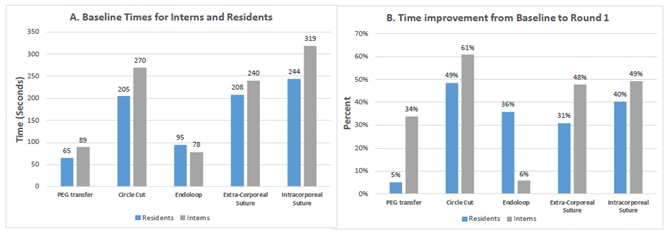 Figure 2: 2a: Time to complete FLS task at baseline for the interns and residents. 2b: Percent time improvement from baseline to round 1 for the interns and the residents.
Figure 2: 2a: Time to complete FLS task at baseline for the interns and residents. 2b: Percent time improvement from baseline to round 1 for the interns and the residents.
Ten out of seventeen (58.8%) residents responded to the survey. All respondents noted the competition to be a positive experience in their surgical education and that it should be continued as part of their curriculum. 90% of the responding respondents reported additional 3.8 hours per week practice on average. 70% of the residents reported improvement in their laparoscopic skills after practicing for and participating in the competition.
Discussion
There is no debate that practice of any skill improves the ability to perform that skill. This study shows that participation in a tournament, using gamification elements, leads to improvement in FLS skills. While it is certainly not novel that practice improves performance, it is new that the application of gamification principles to surgical tasks improves performance, since previously gamification has led to inconsistent results in medical education.
It has been demonstrated that technical laparoscopic skills are learned at different rates, but as long as learners continue to practice, they will improve [8,9]. It is difficult for surgical educators to effectively incorporate simulation training into any surgical training curriculum due to the difficulty in finding time for the trainees to practice. Any addition to educational training must likely be faced with a zero-sum gain, as another activity likely must be eliminated or curtailed to make room for any additional simulation use.
When it is left solely to the learner, practice often occurs sparingly or not at all. In one study of surgical trainees, 95% believed that simulation training improved their laparoscopic skills. Despite this, voluntary use occurred infrequently, with the lack of time cited as the largest hurdle [10]. There have been numerous attempts to encourage the use of the simulation centers in the residency programs. One novel method used social networking to increase participation in FLS training. This method requires a website moderator to send motivational messages and reminders and is most likely too labor intensive to incorporate into most curriculums [11].
Gamification attempts to increase the motivation of the learner to practice without adding cost of or equipment. A curriculum designed using principles of gamification hopes to sustain a learner’s interest to practice without becoming bored [6]. In one study, the introduction of gamification into robotic education among residents boosted the use of robotic simulation. However, the winning residents were offered prizes that could be construed as an increased motivation to practice [12]. The argument could be made that even though there were no prizes offered in our study, the competitive nature of surgeons and surgical residents serves as a motivation for the learners. There is evidence that this is not the case, however. In one study looking specifically at whether competitive training affects laparoscopic surgical performance, competitiveness did not have a profound effect on laparoscopic novices [13]. The incorporation of gamification provided our participants with the stimulus to practice more simulation. Residents reportedly incorporated additional four hours of weekly practice on the simulator in anticipation of the tournament. This is a significant amount of time considering the time commitment required in a general surgery residency.
One of the positives found in this study is that laparoscopic neophytes gained early exposure to laparoscopic skills and therefore gained the largest advantage from the practice. This is expected and has been demonstrated by others that the early exposure to a surgical simulation curriculum enhances surgical intern performance [14]. Cost reporting in simulation research is infrequent and often incomplete [15]. In our study, we used the existing box trainers and equipment that was already set up for simulation. The addition of gamification simply increases the amount of time that the residents practice and there was no additional cost.
This study has several limitations. It is a small single academic institution study and it is impossible to see if the logistics of the competition or the results are transferrable to other training environments. Like all gamification techniques used in medical education, these need validation, as to this point in time, there is no definitive proof that games are an effective teaching strategy for health professionals [16,17]. Finally, there are significant limitations in using time alone as a surrogate for overall competency in the operating room. FLS scoring is already weighted more toward speed than precision and may not significantly address less adroit tissue handling skills [18]. Further evaluation using holistic assessment models is needed to evaluate transferability of specific task to the operating room setting. Despite these limitations, this study shows that the addition of gamification is very successful in encouraging residents to practice on FLS simulation and improve their time to complete the FLS tasks.
Surgical educators must continue to look for innovative ways to educate the trainees. Using gamification technique is a good place to start.
Conclusion
The addition of gamification techniques to FLS skills improved resident times on all FLS tasks and resident feel that gamification techniques were valuable for their education.
Authors Contribution
Luv Hajirawala: Data analysis and interpretation, drafting the article, critical revision for Intellectual content, final approval of the manuscript.
Gregory Peirce: Data acquisition, Data analysis and interpretation, critical revision for intellectual content, final approval of the manuscript.
William V Rice: Data analysis and interpretation, critical revision for intellectual content, final approval of the manuscript.
Kurt G Davis: Study conception design, drafting the article, critical revision for intellectual content, final approval of the manuscript.
Declaration of Interest
None.
Disclosure
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
References
- Peters JH, Fried GM, Swanstrom LL, Soper NJ, Sillin LF, et al. (2004) Development and validation of a comprehensive program of education and assessment of the basic fundamentals of laparoscopic surgery. Surgery 135: 21-27.
- Zendejas B, Ruparel RK, Cook DA (2016) Validity evidence for the Fundamentals of Laparoscopic Surgery (FLS) program as an assessment tool: A systematic review. Surg Endosc 30: 512-520.
- Okrainec A, Soper NJ, Swanstrom LL, Fried GM (2011) Trends and results of the first 5 years of Fundamentals of Laparoscopic Surgery (FLS) certification testing. Surg Endosc 25: 1192-1198.
- Steigerwald SN, Park J, Hardy KM, Gillman LM, Vergis AS (2015) Does laparoscopic simulation predict intraoperative performance? A comparison between the Fundamentals of Laparoscopic Surgery and LapVR evaluation metrics. Am J Surg 209: 34-39.
- Pitzul KB, Grantcharov TP, Okrainec A (2012) Validation of three virtual reality Fundamentals of Laparoscopic Surgery (FLS) modules. Stud Health Technol Inform 173: 349-355.
- Yunyongying P (2014) Gamification: Implications for curricular design. J Grad Med Educ 6: 410-412.
- Ahmed M, Sherwani Y, Al-Jibury O, Najim M, Rabee R, et al. (2015) Gamification in medical education. Med Educ Online 20: 29536.
- Buckley CE, Kavanagh DO, Nugent E, Ryan D, Traynor OJ, et al. (2014) The impact of aptitude on the learning curve for laparoscopic suturing. Am J Surg 207: 263-270.
- Rivard JD, Vergis AS, Unger BJ, Gillman LM, Hardy KM, et al. (2015) The effect of blocked versus random task practice schedules on the acquisition and retention of surgical skills. Am J Surg 209: 93-100.
- Shetty S, Zevin B, Grantcharov TP, Roberts KE, Duffy AJ (2014) Perceptions, training experiences, and preferences of surgical residents toward laparoscopic simulation training: A resident survey. J Surg Educ 71: 727-733.
- Petrucci AM, Kaneva P, Lebedeva E, Feldman LS, Fried GM, et al. (2015) You have a message! Social networking as a motivator for FLS training. J Surg Educ 72: 542-548.
- Kerfoot BP, Kissane N (2014) The use of gamification to boost residents’ engagement in simulation training. JAMA Surg 149: 1208-1209.
- Hashimoto DA, Gomez ED, Beyer-Berjot L, Khajuria A, Williams NN, et al. (2015) A randomized controlled trial to assess the effects of competition on the development of laparoscopic surgical skills. J Surg Educ 72: 1077-1084.
- Buckarma EH, Gas BL, Pandian TK, Abdelsattar JM, El Khatib MM, et al. (2016) Catch me if you can…early simulation efforts affect fundamental surgical skill assessment scores. Am J Surg 211: 583-588.
- Zendejas B, Wang AT, Brydges R, Hamstra SJ, Cook DA (2013) Cost: The missing outcome in simulation-based medical education research: A systematic review. Surgery 153: 160-176.
- Graafland M, Schraagen JM, Schijven MP (2012) Systematic review of serious games for medical education and surgical skills training. Br J Surg 99: 1322-1330.
- Akl EA, Kairouz VF, Sackett KM, Erdley WS, Fiander M, et al. (2013) Educational games for health professionals. Cochrane Database Syst Rev 1: 006411.
- Kowalewski TM, White LW, Lendvay TS, Jiang IS, Sweet R, et al. (2014) Beyond task time: Automated measurement augments fundamentals of laparoscopic skills methodology. J Surg Res 192: 329-338.
Citation: Hajirawala L, Peirce G, Rice WV, Davis KG (2021) Preparing Surgical Residents for the Fundamentals of Laparoscopy Surgery (FLS) Skills Examination Using Gamification: The March Madness Method. Archiv Surg S Educ 3: 014.
Copyright: © 2021 Luv Hajirawala, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.