Prevalence and Socio - Demographic Determinants of Sexual Dysfunction among Married Women of Reproductive Age Group in South West Nigeria
*Corresponding Author(s):
Olugbenga-Bello AIDepartment Of Community Medicine, Faculty Of Clinical Sciences, College Of Health Sciences, Ladoke Akintola University Of Technology (LAUTECH), Osogbo, Osun State, Nigeria
Tel:+234 8033839282,
Email:nike_bello@yahoo.com
Abstract
Background information: Healthy sexual functioning is an important contributor to women's sense of well-being and quality of life. Sexual Dysfunction (SD) refers to a problem during any phase of the sexual response cycle that prevents the individual from experiencing satisfaction from the sexual activity. It affects the self-esteem, quality of life and has threatened homes, therefore imperative to study this aspect of human life so as to improve the stability of families in our society.
Aim: To determine the prevalence and determinant of sexual dysfunction among married women in Osogbo metropolis.
Method: This is a descriptive cross sectional study in which 500 interviewer administered pre-tested, semi-structured questionnaires were analysed using SPSS statistical software version 23.
Results: Majority of respondents 306 (61.2%) are within the ages of 30-44 with the mean age of 34.8+2 years. Majority of respondents 63% were married. Of all the 500 respondents, 338(67.6%) have heard about sexual dysfunction before the study, The prevalence of one form of sexual dysfunction among the respondents was 444 (89%), and was found to be associated with fear, sadness and guilt in 6.4%, 8.8% and 17% of respondents respectively. Majority of the respondents 316 (63.2%) were desirous of change in their love life due to sexual dysfunction. Monogamous family setting, professionals and women within the ages of 30-44 years were significantly more likely have sexual dysfunction. However, there was no significant association between, a low family income, being overweight or obese, being diabetic or hypertensive with sexual dysfunction.
Conclusion: This study shows high prevalence of one form or the other of sexual dysfunction among the respondents. It is therefore recommended that awareness about sexual dysfunctions through health education interventions should be scaled among women of reproductive age in Nigerian.
Keywords
Determinants; Married women; Prevalence; Sexual dysfunction; Socio-demographic characteristics; Southwest; Women of reproductive age
INTRODUCTION
Sexual intercourse is as old as humanity itself and is necessary for the propagation of human beings [1]. A large component of sexual desire in women is responsive rather than spontaneous, therefore, motivation and ability of women to find and respond to sexual arousal and subsequent sexual desire is crucial but complex [1]. Healthy sexual functioning is an important contributor to women's sense of well-being and quality of life [2]. It correlate well with how mentally exciting she finds the sexual stimulus and its context and poorly with objective genital blood flow changes [1]. Sexual dysfunction refers to a problem during any phase of the sexual response cycle that prevents the individual from experiencing satisfaction from the sexual activity [3]. The sexual response cycle has four phases which are the excitement, plateau, orgasm and resolution [3]. The categories of sexual dysfunction are sexual desire disorder, sexual arousal disorder, sexual orgasmic disorder and sexual pain disorder [3,4]. About 22-43% of women all over the world experience sexual dysfunction [4]. The result showed that prevalence of sexual problem was higher in East Asia and South-east Asia than in other regions of the world [5]. Study have shown that lack of interest in sex and inability to reach orgasm were the most common sexual problems in women across the world regions ranging from 26-43% and 18-41% respectively [5]. In USA 30-50% of their women have sexual dysfunction [4]. In Ghana Kumasi metropolis prevalence of sexual dysfunction was 72.8% among sexually active women [6]. In Nigeria the prevalence of sexual dysfunction was found to be 63% [1]. The ranges of dysfunctions across USA includes lack of interest in sex, unable to achieve orgasm, pain during sex, sex not pleasurable constituting 27-32%, 22-28%, 8-21%, 17-27% respectively [7]. Sexual dysfunction is more prevalent in women than men, 43% compared to 31% [7]. Female sexual function is complex and affected majorly by physical, psychological and social factors [8]. The prevalence of female sexual dysfunction is high, ranging from 43% to 88% [5,7]. In Nigeria the ranges of sexual dysfunction includes disorder of desire, disorder of arousal, disorder of orgasm and painful coitus constituting 8.3%, 5.4% ,63.6%, 22.7% respectively [1].
Sexual dysfunction significantly affect self-esteem, quality of life and has threatened home, harm relationship leading to frustration, anguish, anxiety, depression and cause problems in other aspects of life [8,9]. The reason for unsatisfactory sexual life mainly included Medical illness, aging, smoking, excessive domestic duties, lack of adequate foreplay, previous sexual abuse, guilt feeling of previous pregnancy termination among infertile women, competition among wives in a polygamous family setting, lifestyle and culture have been associated with female sexual dysfunction [1,10-12]. Several studies [13-15] have linked sexual dysfunction to existence of uterine fibroids. Women with fibroids report higher frequency of mild dyspareunia and an 80% higher frequency of moderate to severe dyspareunia than women without fibroid. The peak age of sexual dysfunction occur among the age group of 26-30 years which are the productive age group of the society thereby leading to decrease output which also lead to a significant economic loss in our community [1].
Sexual dysfunction severely affects the quality of life of women with many consequences such as inhibition of sexual desire, painful intercourse and infidelity among spouses leading to increase prevalence of sexually transmitted infections and broken homes [1,16]. Although sexual dysfunction among women is an important public-health problem in Nigeria, few works has been done in this area in Nigeria. Female sexual dysfunction is a highly prevalent and often underestimated problem in the general community; however, it has not been studied as extensively as male sexual dysfunction. Furthermore, there is paucity of research on this topic globally, in Nigeria, Osun State and Osogbo metropolis in particular. Sexual dysfunction is a real social and psychological problem in our society demanding urgent attention, it is therefore imperative to study this aspect of women’s life so as to improve the stability of families in our society [1]. Hence, this study aimed to determine the prevalence and determinants of sexual dysfunction among married women in Osogbo metropolis.
MATERIALS AND METHODS
Description of study area
The study was carried out in Osogbo metropolis, which is the capital of Osun State, one of the 36 states in the South western part of Nigeria. Osogbo lies along Latitude 7046’N 4034’E and Longitude 7.7670N 4.5670E51. Osogbo has a total land area of 47km2 (18square meters) [17]. The Population of Osogbo according to the 2006 Census was 156,694.14. Osogbo has 3 Local Government Area namely Osogbo, Olorunda, Egbedore LGAs with Osogbo, Igbona and Awo serving as the headquarter respectively [18]. Osogbo has health care facilities that offer mental health services such as Lautech Teaching Hospital Osogbo and some other private facilities.
Study population
The study included women of reproductive age group between the ages of 15-49 who are sexually active residing within Osogbo metropolis.
Inclusion and exclusion criteria
The study included all married women of reproductive age group between 15-49 who are sexually active. Married women within this age group who are not living with their partners were excluded as well as pregnant women or women within two weeks post-partum.
Study design
The study was a descriptive cross sectional study.
Sample size determination
The sample size was calculated using the Leslie Fischer’s formula for population greater than 10,000 with a prevalence of sexual dysfunction among women of reproductive age group, which in this case is 63% [1]. The sample size calculated was 358 and it was eventually approximated to 500 to give room for non-respondents.
Sampling techniques
A multi- stage sampling technique was used for this study.
Stage 1: simple random technique was used to select 3 of the 10 wards in each of the three local governments in Osogbo metropolis.
Stage 2: simple random technique was used to select 3 streets in each ward.
Stage 3: systematic random sampling technique was used to select houses in such a way that every 3rd house in a clockwise direction was selected for the study. The first house was chosen by balloting and every 3rd house thereafter selected. Only eligible respondents in all the houses were selected for the study and if the house is not inhabited, the next house to it was selected while the interval thereafter was maintained.
Instrument of data collection
A pre-tested, semi- structured questionnaire was used as instrument for data collection.
Data collection
Data was collected over a period of two months at the various houses in the selected street and wards.
Data management
Statistics Package for Social Sciences (SPSS) version 16.0 was used for the analysis. Questions on knowledge were scored with 0 awarded to wrong answers and 1 awarded to right answer. Total score computed was 6 and mean score was 4.5. Those with mean score and above is said to have adequate knowledge while those with less than mean score is said to have inadequate knowledge. Questions on prevalence and pattern of sexual problems were scored with 2 awarded to always 1 to occasionally and 0 to never on related questions. Total score is 12 and mean score is 6.1. Those with 0 is said to have no sexual dysfunction while those with 1 and above is said to have sexual dysfunction. Questions on medical and social determinants of sexual dysfunction were scored with 2 awarded to yes, 0 to no and 1 for not sure. Score ranges from 0-12 with mean score of 1.4.
Ethical consideration
Ethical approval was obtained from the ethical committee of Lautech Teaching Hospital, Osogbo. Also verbal informed consent was sought and obtained from each correspondent and were informed of their freedom to withdraw at any point without any penalty.
Study limitation
Some of the respondents were unwilling to volunteer information due to the sensitive nature of the study but we overcame this by maintaining good rapport and ensuring strict confidentiality.
RESULTS
A total of 500 questionnaires were completed and used in analysis giving a response rate of 100%. Table 1 shows the socio-demographic characteristics of the respondents. Majority of respondents 61.2% were found between the ages of 30-44. The mean age of respondents was 34.8 years. Majority of respondents were married and of the Christian faith, 63% and 95.4%respectively. Only 0.2% of respondents had no form of education at all while about half of the respondents (51.6%) were professionals. The study also showed a predominantly Yoruba population of 93.6% and 56.2% of respondents earn below 18,000 Naira monthly (50$).
|
Characteristics |
Frequency |
Percentage |
|
Age (years) 15-29 30-44 45-59 |
131 306 63 |
26.2 61.2 12.6 |
|
Religion Christian Islam Traditional |
315 182 3 |
63 36.4 0.6 |
|
Marital status Married Widowed Separated Cohabiting |
477 10 9 4 |
95.4 2 1.8 0.8 |
|
Occupation Trading Artisan Professional |
150 92 258 |
30 18.4 51.6 |
|
Level of education Primary Secondary Tertiary None |
29 132 338 1 |
5.8 26.4 67.6 0.2 |
|
Ethnicity Yoruba Igbo Hausa Others |
468 22 4 6 |
93.6 4.4 0.8 1.2 |
|
Duration of marriage 1_9 10_18 >19 |
288 140 72 |
57.6 28 14.4 |
Table 1: Socio-demographic characteristics of respondents.
Table 2 shows respondents’ knowledge of sexual problems, of all the 500 respondents, 67.6% have heard about sexual dysfunction before, and of the 67.6%, their sources of information were medical personnel (34.6%), Friends (26.9%), Radio (16.0%), Magazine (11.5%) and Television (11.0%). Majority, 58.6% of respondents, do not have adequate knowledge of SD (Table 2 and Figure 1) less than halve of the respondents (44.6%) reported finding sex pleasurable over a 2 month period, as shown in table 3 below, while majority of the respondents 333 (66.2%) occasionally lacked interest in sex, 283(56.6%) occasionally experienced vaginal dryness during sex, 197 (39.4%) were unable to reach orgasm in the last 2 months (Table 3). The prevalence of sexual dysfunction among respondents was, 444 (89%), (Figure 2). Majority of respondents, 93% and 94.4% had no past medical history of hypertension and diabetes respectively, this was confirmed with the measured values of blood pressure and random blood glucose during the survey. Only few of respondents 18.4%, 4.2%, 11.4% and 4.6% had history of genital mutilation, hysterectomy, episiotomy and perineal surgery respectively. Very few, 1.4%, of respondents who were sexually abused admitted to have contributed to their sexual dysfunction. Health status survey showed that majority of respondents 92.0% and 99.4% had normal blood pressure and random blood glucose values respectively (Table 4).
|
Variable |
Frequency |
Percentage |
|
Have you heard about sexual dysfunction |
||
|
Yes |
338 |
67.6 |
|
No |
162 |
32.4 |
|
Respondents Knowledge of sexual dysfunction |
||
|
Disorder of Desire |
242 |
48.4 |
|
Disorder of Arousal |
230 |
46.0 |
|
Vaginal Dryness |
303 |
60.6 |
|
Disorder of Orgasm |
244 |
48.8 |
|
Painful Sex |
310 |
62.0 |
|
Sexual Satisfaction |
211 |
42.2 |
|
Can sexual dysfunction be managed |
|
|
|
Yes |
260 |
52.6 |
|
No |
240 |
48 |
|
Management options |
||
|
Use of drugs |
45 |
17.3 |
|
Counselling |
132 |
50.8 |
|
Use of herbs |
5 |
1.9 |
|
Don't know |
78 |
30 |
|
Source of information |
||
|
Friends |
91 |
26.9 |
|
Magazine |
39 |
11.5 |
|
Radio |
54 |
16 |
|
Television |
37 |
11 |
|
Medical personnel |
117 |
34.6 |
Table 2: Respondents knowledge of sexual problem, management and source of information n=500.
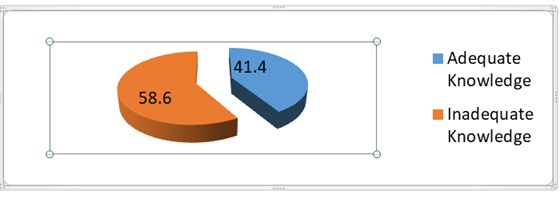
Figure 1: Knowledge status of respondents on Sexual dysfunction.
|
Variable |
Frequency (Percentage) |
||
|
Always |
Never |
Occasionally |
|
|
Lacked interest in sex |
43 (8.6) |
126 (25.2) |
331 (66.2) |
|
Find sex pleasurable over 2 month period |
223 (44.6) |
51 (10.2) |
226 (45.2) |
|
Vaginal dryness over 2 month period |
22 (4.4) |
195 (39.0) |
283 (56.6) |
|
Experienced pain during sex over 2 months |
31 (6.2) |
202 (4.4) |
267 (53.4) |
|
Unable to reach orgasm over past 2 months |
32 (6.4) |
197 (39.4) |
271 (54.2) |
|
Reached orgasm quickly over the past 2months |
30 (6.0) |
195 (39.0) |
275 (55.0) |
Table 3: Patterns of sexual dysfunction among respondents.
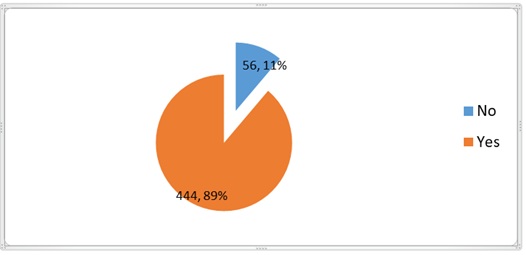
Figure 2: Showing the prevalence of sexual dysfunction.
|
Variable |
Frequency (Percentage) |
||
|
Yes |
No |
Don't Know |
|
|
Diagnosed Diabetic |
19 (3.8) |
472 (94.4) |
9 (1.8) |
|
Diagnosed Hypertensive |
28 (5.6) |
465 (93.0) |
7 (1.4) |
|
Diagnosed with heart disease |
12 (2.4) |
479 (95.8) |
9 (1.8) |
|
Diagnosed with depression |
19 (3.8) |
465 (93.0) |
16 (3.2) |
|
Diagnosed with stroke |
4 (8) |
490 (98.0) |
6 (1.2) |
|
Diagnosed of perineal injury |
15 (3.0) |
479 (95.8) |
6 (1.2) |
|
Diagnosed with urinary tract infection |
71 (14.2) |
414 (82.8) |
15 (3.0) |
|
Genital mutilation |
92 (18.4) |
408 (81.6) |
|
|
Hysterectomy |
21 (4.2) |
479 (95.8) |
|
|
Episiotomy |
57 (11.4) |
443 (88.6) |
|
|
Perineal surgery |
23 (4.6) |
477 (95.4) |
|
|
Victim of sexual abuse |
25 (5.0) |
475 (95.0) |
|
|
Sexual abuse contributes to sexual problem |
7 (1.4) |
493 (98.6) |
|
|
Drug intake affecting sexual performance |
6 (1.2) |
494 (98.8) |
|
Table 4: Respondents’ past medical history.
Despite the revelation of a huge prevalence of sexual dysfunction, (88.8%), among the respondent, table 5, and figure 3 shows that the effects of sexual dysfunction on quality of life was not as pronounced. Only 3.6% of the respondents frequently quarrel with their partners, while a third of the respondents, 31%, occasionally do so. Majority of respondents (63.2%) were desirous of change in their love life, only 6.4%, 8.8% and 17% of the respondents expressed fear, sadness and guilt respectively as a result of SD. In addition, 86% of the respondents had high expectations about the future, only a few of the respondents (7.8%) claimed that sexual dysfunction affected their productivity, while majority (80.4%) believed that their present relationship with their partner does not predispose him to infidelity. Majority of respondents (92.0%) had normal blood pressure values below 140/90mmHg while almost all of respondent (99.4%) had normal random blood glucose values between 7.0-11.1mmol/l as shown below. This study shows a significant association between family setting and SD with higher proportion of respondents in a monogamous relationship. In the same vein, there is significant association between occurrence of SD and being a professional, in the age range 20-44 years, and having a tertiary education with P value >0.05. However, no significant association between experiencing SD and the respondent’s present medical conditions (Tables 5-7).
|
|
Yes (%) |
No (%) |
DON'T KNOW (%) |
|
Creating a form of fear in respondent |
32 (6.4) |
417( 83.4) |
51 (10.2) |
|
Affecting the frequency of sexual relationship of respondent with partner |
41 (8.2) |
418 (83.6) |
41 (8.2) |
|
Causing a feeling of sadness |
44 (8.8) |
416 (83.2) |
40 (8.0) |
|
Causing a feeling of guilt for not being able to |
|||
|
Satisfy sexual partner |
85 (17.0) |
379 (75.8) |
36 (7.2) |
|
Satisfaction with present sexual relationship |
415 (83.0) |
58 (11.6) |
27 (5.4) |
|
Partner satisfaction with sexual relationship |
410 (82.0) |
32 (6.4) |
58 (11.6) |
|
Happiness with marriage |
456 (91.2) |
37 (7.4) |
7 (1.4) |
|
High expectations about the future |
430 (86.0) |
59 (11.8) |
11 (2.2) |
|
Low expectations about the future |
41 (8.2) |
441 (88.2) |
18 (3.6) |
|
Affectation of productivity by sexual dysfunction |
39 (7.8) |
443 (88.6) |
18 (3.6) |
|
Partner’s predisposition to infidelity due to |
|||
|
respondents’ sexual dysfunction |
26 (5.2) |
402 (80.4) |
72 (14.4) |
|
Thought of extramarital relationship by respondent |
27 (5.4) |
456 (91.2) |
17 (3.4) |
|
Desirous of a change in love life |
316 (63.2) |
137 (27.4) |
47 (9.4) |
Table 5: Showing the effects of sexual dysfunction(SD) on quality of life.

Figure 3: frequency of quarrel over sex between respondents and their sex partners.
|
Variables |
Sexual dysfunction |
No sexual dysfunction |
X2 |
df |
P value |
|
Family setting Monogamous Polygamous |
85.8 14.2 |
14.2 85.8 |
7.732 |
1 |
0.005 |
|
Occupation Trading Artisan Professional |
28.8 20.3 50.9 |
71.2 79.7 49.1 |
9.724 |
2 |
0.008 |
|
Religion Christian Islam Traditional |
63.5 36 0.5 |
36.5 64 99.5 |
1.345 |
2 |
0.51 |
|
Age (years) 15-29 30-44 45-59 |
27.5 58.8 13.7 |
72.5 41.2 86.3 |
10.331 |
2 |
0.006 |
|
Level Of education Primary Secondary Tertiary None |
4.7 27.7 67.6 0 |
95.3 72.3 32.4 100 |
13.149 |
3 |
0.004 |
|
Income <minimum wage >minimum wage |
56.3 43.7 |
43.7 56.3 |
0.018 |
1 |
0.893 |
Table 6: Association between respondents’ Socio-demographic characteristics and sexual dysfunction status.
|
Variables |
Sexual dysfunction |
No sexual dysfunction |
X2 |
df |
P value |
|
body mass index Less than 18 Between 18.5 -29.9 Greater than 30 |
0.5 82.9 16.7 |
99.5 17.1 83.3 |
1.558 |
2 |
0.459 |
|
Random body sugar Normal Abnormal |
99.3 0.7 |
0.7 99.3 |
0.381 |
1 |
0.537 |
|
Blood pressure Normal below 140/90mmhg Abnormal above 140/90mmhg |
92.3 7.7 |
7.7 92.3 |
0.112 |
1 |
0.738 |
Table 7: Association of Health status with Sexual dysfunction.
DISCUSSION
The age range of the respondents is between the 15-59 years, the mean is 34.8 years with majority of the respondents being between the ages of 30-44 years, and the prevalence of sexual dysfunction was found to be significantly higher in this age group. This is similar to the study conducted in Ghana [6] in which the major age group of the respondents affected was found to be between 38-44 years but differs from the result of a study done in Ife [1] which shows higher prevalence in lower age group, 26-30 years. It also confirms the observations from other studies that female sexual dysfunction increases with increasing age [7,8]. The prevalence of sexual dysfunction among women of reproductive age in this study was found to be 88.8% this show that sexual dysfunction is relatively high among Nigerian women which is not too far from the prevalence found in the study conducted in USA and Ghana which was 76% [19] and 73% [6] respectively but higher than various studies done in other part of the world like Brazil, [20] Peru, [21] Enugu [22] in Nigeria with prevalence of 35.9%, 35.2%, 53.5% and 68.3% in Ife [1]. The reasons for this high prevalence are not known but various reasons may be adduced for this high prevalence in Nigeria, many obstacles prevent women from expressing their views about sex and sexual matters, culture of male dominance often makes them afraid of rejection and threats of divorce if they ever complain about sex-related matters; hence, many women suffer in silence [1]. In this study, well over half of the respondents reported lack of interest in sex and vaginal dryness as the most form of sexual dysfunction they experienced. This is similar to the studies done in Iran where low-sex drive and inability to reach orgasm were the most prevalent domains of sexual dysfunction in the area [6,23]. Half of the respondents experienced pain during sex in this study which was a little bit lower than the study done in Ghana [24] and Iran [25] which was found to be higher. In this community based study, sexual dysfunction was highest among women with tertiary education and lowest among women with no education which is similar to the study done in Jos [26]. This is different from other studies conducted in Iran and Colombia where low education level was found to have a significant effect on the manifestations of sexual dysfunction, and this finding was confirmed by another study in this regard, which identified low education level as a predictor for sexual complaints [23,26]. The higher prevalence of sexual dysfunction among the highly-educated women may be as a result from the fact that they are bolder to discuss sexual matters openly. In short, it has been documented that the higher the level of female education the higher the probability that they can discuss reproductive health issues with men [5,26]. The fear of social consequences (being beaten, divorced/abandoned, neglected, etc.,) tend to take priority over the fears of the health consequences of such ill-timed sexual acts [27,28]. Present illness, previous history of sexual abuse, living in polygamous family type, and emotionally-unstable individuals are significantly at increased risk of sexual dysfunction, this was totally in contrast to this study. This study observed that very few of the respondents had abnormally high random blood pressure and sugar.
RECOMMENDATION AND CONCLUSION
This study showed a high prevalence, (89%), of Sexual dysfunction among women of reproductive age in Osogbo metropolis, with low level of knowledge on sexual dysfunction. Lack of interest in sex, vaginal dryness and inability to reach orgasm constitute the most common forms of sexual dysfunction among the study group. Age group 20-44 years, monogamous family setting, attainment of tertiary education and being a professional were significantly associated with sexual dysfunction. The measured parameters of blood pressure, random blood glucose and body mass indices however had no statistically significant association with sexual dysfunction.
It is therefore recommended that awareness about sexual dysfunctions through health education interventions should be scaled up among Nigerian women. Government should made policy that will remove obstacles that prevent women from expressing their views about sex and sexual matters by encouraging gender equity and equality so that women do not suffer in silence. In addition, appropriate counseling and sexual health education for women and their partners could potentially decrease the burden and prevalence of sexual problems. Sexual disorder clinics should be established where professional inputs of various professionals like Sex therapists, Psychiatrists, Clinical Psychologists, Gynecologists and Community Physicians will be made easily accessible to women.
DISCLOSURE
The authors report no conflicts of interest in this work.
REFERENCES
- Fajewonyomi BA, Orji EO, Adeyemo AO (2007) Sexual dysfunction among female patients of reproductive age in a hospital setting in Nigeria. J Health Popul Nutr 25: 101-106.
- Salonia A, Zanni G, Briganti A, Fabbri F, Rigatti P, et al. (2004) The role of the urologist in the management of female sexual dysfunctions. Curr Opin Urol 14: 389-393.
- The Cleveland clinic foundation (2015) Sexual dysfunction in females. The Cleveland clinic foundation, Ohio, USA.
- Julie AE, Yvone B (2015) Female sexual dysfunction. Cleveland Clinic, Ohio, USA.
- Laumann EO, Nicolosi A, Glasser DB, Pai KA, Gingell C, et al. (2005) Sexual problems among women and men aged 40-80yr: Prevalence and correlate identified in the global study of sexual attitude and behaviours. Int J Impot Res 17: 39-57.
- Nafiu A, William KB, Eric W, Otchere AM, Lawrence Q, et al. (2010) Incidence of sexual dysfunction: A prospective survey in Ghanaian females. Reprod Biol Endocrinol 8: 106.
- Sarit OA, Roger PG (2014) Female sexual function and pelvic floor.
- Kaiser FE (2006) Sexual function and the older woman. Clin Geriatr Med 19: 463-472.
- Dennerstein L, Lehert P, Burger H, Guthrie J (2005) Sexuality. Am J Med 118: 59-63.
- Nappi RE, Verde JB, Polatti F, Genazzani AR, Zara C (2002) Self-reported sexual symptoms in women attending menopause clinics. Gynecol Obstet Invest 53: 181-187.
- Basson R (2000) The female sexual response: A different model. J Sex Marital Ther 26:51-65.
- Nappi RE, Veneroni F, Verde JB, Polatti F, Fingnon A, et al. (2001) Climacteric complaints, female identity, and sexual dysfunctions. J Sex Marital Ther 27: 567-576.
- Zimmermann A, Bernuit D, Gerlinger C, Schaefers M, Geppert K (2012) Prevalence, symptoms and management of uterine fibroids: An international internet-based survey of 21,746 women. BMC Womens Health 12:6.
- Ertunc D, Uzun R, Tok EC, Doruk A, Dilek S (2009) The effect of myoma uteri and myomectomy on sexual function. J Sex Med 6: 1032-1038.
- Lippman SA, Warner M, Samuels S, Olive D, Vercellini P, et al. (2003) Uterine fibroids and gynecologic pain symptoms in a population-based study. Fertil Steril 80: 1488-1494.
- https://www.webmd.com/women/guide/sexual-dysfunction-women#1
- https://osun.gov.ng/
- Murphy JM, Sanford (2001) Reviewed work: Osun across the waters: A Yoruba goddess in Africa and the Americas. The International Journal of African Historical Studies 34: 666-667.
- Weigel M, Meston C, Rosen R (2005) The Female Sexual Function Index (FSFI): Cross-validation and development of clinical cutoff scores. J Sex Marital Ther 31: 1-20.
- Valadares ALR, Pinto-Neto AM, Osis MJ, Sousa MH, Costa-Paiva L, et al. (2008) Prevalence of sexual dysfunction and its associated factors in women aged 40-65 years with 11 years or more of formal education: A population-based household survey. Clinics 63: 775-782.
- Mezones-Holguin E, Córdova-Marcelo W, Lau-Chu-Fon F, Aguilar-Silva C, MoralesCabrera J, et al. (2011) Association between sexual function and depression in sexually active, mid-aged, Peruvian women. Climacteric 14: 654-660.
- UI Nwagha, TC Oguanuo, K Ekwuazi TO Olubobokun, TU Nwagha, et al. (2014) Prevalence of sexual dysfunction among females in a university community in Enugu, Nigeria. Niger J Clin Pract 17: 791-796.
- Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, et al. (2005) Sexual problems among women and men aged 40-80 y: prevalence and correlates identified in the global study of sexual attitudes and behaviors. Int J Impot Res 17: 39-57.
- Esfehani RJ, Fazel N, Dashti S, Moshkani S, Hasanabad FH, et al. (2016) Female Sexual Dysfunction and its Associated Risk Factors: An Epidemiological Study in the North-East of Iran. Journal of Midwifery & Reproductive Health 4: 498-505.
- Tayebi N, Ardakani SMY (2009) Incidence and prevalence of the sexual dysfunctions in infertile women. Eur J Gen Med 6: 74-77.
- Kevin G, Raquel G, Cornelia G, Nicholas H (2015) Female sexual dysfunction.
- Salomei A, Zanni G, Briganti A, Fasbri F, Rigatti P, et al. (2004) The role of the urologist in the management of female sexual dysfunctions. Curr opin Urol 14: 389-393.
- Echeverry MC, Arango A, Castro B, Raigosa G (2010) Study of the prevalence of female sexual dysfunction in sexually active women 18 to 40 years of age in Medellín, Colombia. J Sex Med 7: 2663-2669.
Citation: Olugbenga-Bello AI, Adebayo KO, Goodman OO, Oke OS, Olukunle TO (2020) Prevalence and Socio - Demographic Determinants of Sexual Dysfunction among Married Women of Reproductive Age Group in South West Nigeria. J Reprod Med Gynecol Obstet 5: 046.
Copyright: © 2020 Olugbenga-Bello AI, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.