Pyostercoral Phlegmon: A Rare and Historical Complication of Strangulated Hernia
*Corresponding Author(s):
Ayadi MFSurgery Department, Monji Slim Hospital, Marsa, Tunis, Tunisia
Email:medfirasayadi26591@gmail.com
Abstract
Pyostercoral phlegmon is a rare complication of strangulated hernias. It is mostly seen in developing countries within female patient with femoral hernia. It is the natural course a non-operated strangulated hernia. We present the case of a 84 years old female patient presented to our emergency department for a pyostercoral phlegmon and treated successfully.
Introduction
Pyostercoral phlegmon is a rare complication of strangulated hernias even in developing countries where it can be present within 4% of all strangulated hernias [1]. This is the natural course of a non-surgically treated hernia with digestive contents. The fear of any doctor is to miss this diagnosis and confuse it with adenophlegmon, especially in the case of a femoral hernia [2]. We report the case of a patient who presented to our department for a pyostercoral phlegmon.
Case Report
It was an 84-year-old patient, with a history of senile dementia, and a stroke with left hemiplegia as sequelae. She presented to the emergency for general state deterioration, vomiting and abdominal distention. Laboratory tests results showed hyperkalemia at 8.5mmol/l and a renal failure with kreatinin level of 720mmol/l it also revealed an inflammatory syndrome with white blood cells account of 14300/ml and a CRP>200mg/l. Faced with menacing hyperkalemia, the patient was hospitalized in the emergency room to correction those disorders. The examination showed a distended abdomen but with no guarding or rigidity. We also noticed an inflammatory and painful swelling in the right groin. The diagnosis of a strangulated femoral hernia complicated by a pyostercoral phlegmon was made. The patient was operated. Intraoperatively it was a sphaceleic small bowel content (Figure 1). We proceeded to a resection of the necrotic small bowl with ileo-ileal anastomosis, a hernia repair using the McVay technique and drainage in the inguinal region. Postoperatively, the patient was kept on antibiotic therapy with correction of renal function and kalemia. The outcomes were simple and she was discharged ten days after the surgery.
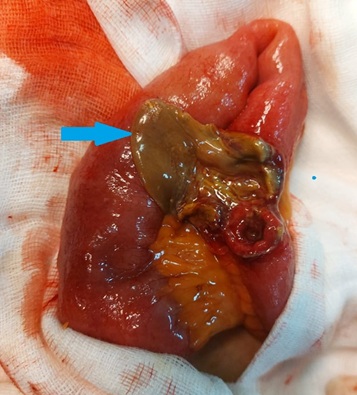 Figure 1: Sphaceleic small bowel (blue arrow).
Figure 1: Sphaceleic small bowel (blue arrow).
Discussion
Abdominal wall hernia consists of the exit of viscera covered with peritoneum through a natural or acquired opening in the abdominal wall [3]. This benign pathology can be life-threatening in case of strangulation. This term refers to the sudden, permanent and tight necking of the organs contained in the hernia sac. Its frequency is estimated at 5% in the case of inguinal hernia and 35 to 40% in the case of a femoral hernia [4]. Not treated in time, it can evolve to content necrosis and a pyostercoral phlegmon such as the case of our patient. It is a complication that mostly seen within women with a femoral hernia. This can be explained by the high frequency of necrosis in femoral hernia which is most frequent within women [5]. The diagnosis of pyostercoral phlegmon is clinical. The clinical examination is done in a standing position, or in the dorsal decubitus position with the leg hanging. This last position facilitates the examination in cases of femorall hernia, particularly in obese patients [6]. The strangulated hernia appears as a tense, painful, hard, irreducible, and not impulsive or expansive mass. The presence of local redness, skin edema or blister is sufficient to suspect pyostercoral phlegmon [7]. Once the diagnosis is suspected, the operative indication is retained. The particularity of pyostercoral phlegmon is that once it is suspected it is preferable to pass first by abdominal route [8]. That permits a resection of the necrotic content without contaminating the peritoneal cavity. The latter is kept in place. Then we go through the elective route where we carry out an exteriorization of the contents and a hernial repair. During this repair the use of mesh is prohibited because of the risk of infection [9]. Outcomes are usually simple but they are depending on the patient comorbidities. In our case they were simple and the patient was discharged ten days after surgery.
Conclusion
Pyostercoral phlegmon is a rare entity even in developing countries. It is a hernia complication that can be life-threatening, hence the value of the rapid management of any hernia even if it is not complicated.
References
- Dumitresco D (2009) Incarcerated umbilical hernia complicated by pyo-stercoral phlegmon. Technical details. Chirurgia 104: 597-599.
- Pierra C (1952) Four cases of surgical intervention in pyo-stercoral phlegmon after crural strangulation. Mem Acad Chir (Paris) 78: 906-907.
- Öberg S, Andresen K, Rosenberg J (2017) Etiology of inguinal hernias: A comprehensive review. Front Surg 4: 52.
- Oberlin O (2010) Evolution of medical thinking in the surgical treatment of male inguinal hernias. E-Mem Acad Natl Chir 9: 30-35.
- Dahlstrand U, Wollert S, Nordin P, Sandblom G, Gunnarsson U (2009) Emergency femoral hernia repair: A study based on a national register. Ann Surg 249: 672-676.
- Beck M, Simeu-Tamnou B (2013) Examen clinique des hernies de l'aine clé de voûte de l'indication opér Le journal de Cœlio-chirurgie 85: 1-4.
- Dieng M, El Kouzi B, Ka O, Konaté I, Cissé M, et al. (2008) Les hernies étranglées de l’aine de l’adulte: une série de 228 observations. Mali Med 23: 12-16.
- Walle KA, Greenberg JA (2018) Strangulated Inguinal Hernia: Options and Strategies. In The SAGES Manual of Hernia Surgery. Springer, Berlin, Germany.
- Hentati H, Dougaz W, Dziri C (2014) Mesh repair versus non-mesh repair for strangulated inguinal hernia: Systematic review with meta-analysis. World J Surg 38: 2784-2790.
Citation: Ayadi MF, Medhioub F, Atallah A, Omrani S, Mestiri H, et al. (2022) Pyostercoral Phlegmon: A Rare and Historical Complication of Strangulated Hernia. Archiv Surg S Educ 4: 037.
Copyright: © 2022 Ayadi MF, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.