Quality of Life and Health-Related Quality of Life Among End-Stage Kidney Disease Patients: Testing the Concepts and Assessing the Measures
*Corresponding Author(s):
Issa Al SalmiThe Renal Medicine, The Royal Hospital, Muscat, Oman
Tel:96892709000,
Email:isa@ausdoctors.net
Abstract
Background
Little is known about how patients with End-Stage Kidney Disease (ESKD) view their life quality, yet this is an outcome of increasing importance. Most research in this area has been conducted within a certain Western countries’ context using measures that have not been validated within our region context.
Method
Patients were randomly selected from a dialysis unit center in Oman. The understanding of Quality of Life (QoL) concept was explored using an individualized QoL instrument (SEIQoL-DW). A cognitive interviewing method was used to explore patients’ interpretations of the Arabic versions of two standardized measures of HRQoL, SF36v2 and QoLI-Dialysis, measures’ items, and report any difficulties they might have in answering these items.
Results
Mean patient age was 53 years and 78% were male. All patients completed the SEIQoL-DW, (mean time 16.08 minutes). Patients appear to understand the notion of QoL. Fifty-nine cues were identified and categorized. The most important/common aspects of life that determined individual QoL were spiritual life, family, personal health, social life, and leisure activities. A full (100%) good completion response rate was obtained by SF36v2 and QoLI Dialysis. Patients were able to comprehend most of the items. Two items in QoLID measure were identified as sensitive and two items in the SF36v2 also were reported to contain complicated syntax.
Conclusion
SEIQoL-DW was an applicable instrument to explore the meaning of the concept of QoL among this population. Spiritual life aspect should be incorporated in any assessment of QoL and HRQoL in this group of patients. Cognitive interviewing was able to helpfully identify the range and depth of difficulties with items of SF36v2 and QoLI-Dialysis within this context, yet these measures should be tested on a larger group.
Keywords
Cognitive interviewing; Chronic Kidney Disease (CKD); End-Stage Kidney Disease (ESKD); Health-related QoL; Hemodialysis; Methodology; Quality of Life (QoL)
INTRODUCTION
Worldwide, there is a continuous rise of various Non-Communicable Disease (NCD) with obesity as the core of this tsunami of medical problem. Chronic Kidney Disease (CKD) is the resultant of many of these NCD with progresses ion towards end-stage kidney disease, which is a major problem to all heath system across the globe [1-7]. Health-Related Quality of Life (HRQoL) is an essential part of evaluating dialysis treatment effectiveness and assessing health outcomes of patients with End-Stage Kidney Disease (ESKD) [8]. Several measures have been developed to assess HRQoL and can be categorized as generic and condition- or disease-specific measures. Generic instruments attempt to measure a broad range of domains that are related to overall quality of life and HRQoL. These instruments cover a range of areas and can be used across different populations [9].
Disease-specific are designed to address areas of life that are particularly pertinent for patients with a specific condition or disease in a predefined list of items which must be rated in a particular manner [10]. Despite these tools being criticized for having a narrow focus, they have been credited with being more sensitive to changes in health status compared to generic instruments [11]. However, the current methods of measuring HRQoL impose an external value system on individuals, rather than allowing them to describe their lives in terms of those factors which they consider important. Measuring such personal and complex concepts is, therefore, difficult and may miss aspects of life that are important to the individual [12]. These aspects may be captured by an individualized quality of life (QoL) tool.
Individualized measurement tools were developed as an attempt to explore the aspects of life that the individual perceives to be most important and to assess the level of functioning or satisfaction within each aspect [13]. The Schedule for the Evaluation of Individual QoL Direct Weighting (SEIQoL-DW) is one of the individualized Quality of Life (QoL) instruments developed by O’Boyle et al. [14]. The main advantage of such methods of QoL measurement is the ability to address an individual’s own concerns about their life rather than impose standard questions which might be less relevant [15].
There are very few studies that have used a combination of generic HRQoL measures, disease-specific measures and QoL individualized measures. Most studies assessing the QoL of patients with ESKD mainly focus on HRQoL. This is perhaps due to the broad agreement that the concept of positive health is more than the absence of disease or even disability, but rather is about full functioning, efficiency of mind and body and social adjustment [16-19]. HRQoL is, therefore, a concept that includes aspects related to physical, mental, social and role functioning and can be measured using distinct components that can be interpreted separately [20].
Even with available studies that assess HRQoL, the majority have been conducted mainly in a selected country of western cultures. Limited studies have examined HRQoL aspects in ESKD patients in an Arab population [21]. The results of these studies showed low HRQoL among Arab patients with ESKD, but none were conducted in Oman. This phase of the study therefore considers this gap in assessing QoL through exploring the understanding of the concept QoL among our patients using SEIQoL-DW instrument. Besides, a cognitive interviewing method was used to test the readability and relevance of items of HRQoL measures among this group of patients.
Cognitive interviewing is qualitative in nature, with participants asked to explain their interpretations of a measure’s items, elaborate on their responses and report any difficulties they might have in answering these items [22]. It also helps and guides in modification and improvement of the measures, but the major advantage is that the process can be iterative, with further rounds of testing leading to further improvements [22-24]. Previous studies have presented a structured model of cognitive interviewing which consists of a sequential process of: a) comprehension of the item, b) retrieval from memory of relevant information, c) decision process and d) response processes [25-28]. The model tests the participants’ comprehension of terminology used in the measured items, their sensitivity to answering items (e.g. items related to sexual activities, religious items).
The process of cognitive interviewing includes two techniques, think aloud and verbal probing. Think aloud technique is used to ask participants to vocalize their thought processes while responding to questionnaire items [22-24]. The advantage of this technique is that it does not require highly trained interviewers, and there is less bias imposed by the interviewer. However, it might also have the disadvantage of causing a burden on respondents especially among those whose first language is not English.
Verbal probing is a way used to ask respondents to provide additional information related to their answers to questionnaire items either at the time of responding to the question (concurrent probing) or after the completion of the entire questionnaire (retrospective probing). The advantage of this technique is that it maintains a focus and control over the interview, whereas the disadvantage is the potential for interviewer imposed bias [22-24].
The overall aim of this phase is to answer RQ1– What does QoL/HRQoL mean to an Omani population using individualized QoL instrument, SEIQoL-DW; and cognitive interviewing to explore their interpretations of the Arabic versions of two standardized measures of HRQoL, SF36v2 and QoLI-D measures’ items, and report any difficulties they might have in answering these items.
METHODS
Population and sample size
The study population was a subset of the target population from whom a randomized sample was taken over the three-week period of data collection, first three weeks of May 2015, based on study-inclusion criteria. The inclusion criteria were adult patients with ESKD receiving HD; those aged ≥ 18 years; and those who had been on HD for at least three months so that they were adjusted to life on dialysis. Exclusion criteria were: patients who did not being on HD longer than three months; patients with acute kidney injury/failure; patients aged under 18;patients diagnosed with dementia or any other condition that could impair their ability to answer questions; patients who had recently been diagnosed with cancer; and patients who had recovered their kidney function.
This sample size of this phase was informed by literature that used the cognitive interviewing method in data collection as well as studies using individual QoL measures [13,29,30]. Although the sample size determined at this phase was 12 participants, 16patients were approached to avoid any inaccuracy of the list as patients sometime quit dialysis for transplant or personal preferences.
Patients were identified from the Dialysis-Unit Registry which records registered patients with ESKD. Using the Dialysis-Unit Registry, eligible patients were approached by the researcher in the allocated waiting area for their regular HD sessions. An explanation about the objectives of this phase and a related information sheet were provided. Patients had 48 hours in which to indicate their interest in participating in the study to the researcher who was physically available in the dialysis unit when they came for their next HD session. For patients who agreed to participate, interview venue and time were decided based on the participant’s preference.
Ethical consideration
Ethics permission was granted by the Directorate of Research and Ethical Review and Approve Committee, at the Ministry of Health, Oman.
Setting
Participants were recruited from the Nizwa Dialysis Unit. This unit is in central Oman and is one of the country’s largest dialysis units. There are around83 patients regularly attending out-patients’ HD.
Data collection process
Measures: Three measures were used in this phase: an individualized QoL instrument (SEIQoL-DW), generic health status measure (Short Form-36v2), and disease specific measure (QoLI-Dialysis). The details of these measures were published earlier (Al Rajhi et al.). SEIQoL-DW instrument is an individualized QoL instrument. It was administered to test the understanding of the concept of QoL by asking the patients to nominate five areas of life that they value most. SEIQoL-DW is based on an underlying theory of what makes up QoL from an individual’s own perspective and on his/her own perception and understanding of QoL [31]. The main advantage of such methods of QoL measurement is the ability to address an individual’s own concerns about their life rather than impose standard questions which might be less relevant [15,32-34].
The SF36v2 measures eight health concepts: physical functioning, social functioning, physical role limitation, emotional role limitations, bodily pain, mental health, vitality and general heath perceptions. These concepts can also be presented as two summary scores representing physical and mental health. The scoring range of the SF-36v2 is 0-100 for each of the eight domains. Zero indicates poor health status and 100 indicates very good health status. The response options for the SF36v2 are rated on a Likert scale.
QoLI-Dialysis was the second HRQoL measure used to explore patients’ understanding of items related to QoLI-Dialysis. The QoLI-Dialysis is the version that was primarily developed by Ferrans and Power for use with dialysis patients [35-37]. It consists of 68 items and measures four key aspects: health and functioning, social and economic, psychological and spiritual, and family. It consists of two sections assessing participant satisfaction and the relative importance of each aspect, respectively. Six-point ordinal response scales range from “very dissatisfied” or “very unimportant” (1), to “very satisfied” or “very important” (6). Its index scores range from zero to 30, where higher scores indicate a better quality of life [38-40].
Procedure and data analysis
Participants were informed verbally and in writing, using the information sheet developed specifically for this phase of the study. For patients unable to read, an information sheet and consent form were explained verbally to them. The consent form was required to be signed by participants and, for those who could not write, an available witness signed instead. The witness was a family member (husband, wife, sister, brother, or close relative such as a cousin). Their preferences for time and venue for the cognitive interviewing and for completing the SEIQoL-DW instrument were considered.
All the interviews were digitally audio taped along with the taking of abbreviated field notes with the patients’ permission. The recordings included the administration process of the SEIQoL-DW and the interactions between patients and researchers during this process.
Individualized quality of life instrument (SEIQoL-DW): Prior to administration of the SEIQoL-DW, and for the purpose of efficient use of SEIQoL-DW, the researcher translated the SEIQoL-DW instruction manual into Arabic. This process was merely for the purpose of simplifying the use of the manual for the researchers and to avoid any lapses that might occur during the reading of instructions to patients.
Initially, the instruction manual was translated by the researchers into Arabic and then sent to two separate reviewers. Reviewer one is a native Arabic speaker who is a doctorate holder and works as a dean for a nursing institute in Oman. Similarly, Reviewer two is a native Arabic speaker and a doctorate holder working as an English-language teacher in a nursing institute in Oman. Both reviewers reviewed and checked the Arabic translation and commented on it independently.
The updated translated draft was then piloted with three nursing students at their clinical placement at Nizwa Hospital. Students were informed about the aim of this pilot and a consent form was obtained for them to participate willingly. Each interview was audio recorded. The time taken to complete SEIQoL-DW was between 13-18 minutes. The three participants reported no difficulties in understanding the instructions on how to complete the SEIQoL-DW tool, nor did they report fatigue or boredom. The acceptability of the SEIQoL-DW was based on time taken to complete the tool, on the understanding of the method and on the level of fatigue and boredom [41,42].
SEIQoL-DW was then administered to patients in three stages. Stage one was the determination of cues, aspects of life. Patients were asked to think of, and nominate, five areas of life (cues) that determine their own happiness, or QoL, without prompts from the researcher (the glossary of terms relevant to SEiQoL-DW, as shown in table 1. The five cues were elicited by means of a semi-structured interview and are referred to henceforth as “elicited cues”.
|
Cue |
The elicited aspect of life considered most important by each patient in assessing their overall QoL. |
|
Definitions record form |
The form used to record the meaning of the elicited aspect of life and to provide definitions by each patient. |
|
Level record form |
The rate or level of each aspect of life for the patient at that moment. |
|
Cue levels record form |
The form used to record the levels and importance of elicited cues. |
|
Weight of cue |
The rate of importance of each elicited aspect of life for the patient at that moment. |
|
Disc weighing system |
The pi diagram used to rate the importance of each elicited aspect of life. |
Table 1: Glossary of terms relevant to SEiQoL-DW.
In stage two, the patients then ‘levelled’ their functioning status on each cue against a vertical Visual Analogue Scale (VAS), labelled at the upper and lower extremes by the terms “As good as could possibly be” and “As bad as could possibly be” respectively, as shown in figure 1. These ratings were recorded by the researcher as a bar chart, one bar representing each cue nominated by patients. This produced five scores, independent continuous measurements, ranging from zero to 100.
 Figure 1: Cue levels record form of SEIQoL-DW.
Figure 1: Cue levels record form of SEIQoL-DW.
In stage three, for the purpose of weighing the elicited cues, patients were asked to quantify the importance of each aspect, represented by five differently colored areas of a disc weighing system which was produced by the SEIQoL-DW developers specifically for this purpose. The disc consists of five interlocking laminated circular discs of different colors on a percentage base and can be rotated independently, as shown in figure 2.
The weight of each aspect was divided by 100, since the weights, when calculating the SEIQoL-DW Index, range from 0.00-1.00, in order that the overall SEIQoL-DW Index can be calculated by multiplying the level by weight of each aspect and then adding these products across the five aspects [SEIQoL Index =∑ (levels x weights)].
 Figure 2: Disc weighing system of SEIQoL-DW.
Figure 2: Disc weighing system of SEIQoL-DW.
For grouped data presentation, three reviewers (researcher, reviewers 1 and 2) categorized the elicited aspects of life definitions using a prompt list summarized from the literature. The researcher, initially, independently categorized the nominated “cues” and these were then emailed separately to reviewers. Any discrepancies that occurred were resolved by discussion. This process was entirely anonymous. Where participants’ quotes are used to support the results, any personal details will be anonymous.
The time for each interview, for understanding the method of SEIQoL-DW and for possible fatigue/boredom that the patient might experience, and the overall validity of the information obtained (in light of the reported understanding of method and fatigue/boredom) were reported using the Interview Record Form (IRF) suggested by the author of the SEiQoL-DW (Appendix 1).
Health-related QoL measures (SF36v2 and QoLI-Dialysis): The Arabic version of the SF36v2 and QoLI-Dialysis were administered using the cognitive interviewing technique to assess whether they were acceptable and understood by Omani ESKD patients. The assumption is that the respondents interpret the measures’ items in the same way as do the measures’ developers despite cultural differences [38,39,43].
The Tourangeau’s model was adopted and employed to test patients’ understanding of SF36v2 and QoLI-Dialysis by asking them to complete each measure exactly as normal, but also to read aloud each question and to “think aloud” their thoughts as they respond to these items [44]. After each interview, field notes and audio recordings were reviewed to identify any potential problems with the measures so that issues were addressed prior to piloting the QoL measure in a larger sample.
The Question Appraisal System (QAS) coding form of probed interviews was used to record the process. QAS was developed to guide researchers through a systematic appraisal of questionnaire items and to help to identify potential problems in the wording or structure of the items that may lead to difficulties in questionnaire administration or to other failings [45].
Data from the cognitive interviewing process were analyzed using a matrix-based method of data analysis proposed by Knafl et al. [46]. Problems were identified and systematically analyzed to facilitate decisions concerning the measures’ use or modification. The matrix illustrates items in a tabular form in which items appear in a row and participants appear in a column. Possible problems to be identified with items are entered into the appropriate intersecting cells, promoting systematic analysis and decision-making regarding item revisions.
The matrix display approach was then used to construct item summaries, linked to all the patients, including a coding scheme to reflect problem types specific to each item that has been tested. The findings were then aggregated across all participants, producing a summarized, measure-by-question analysis of the results associated with QoL measures (SF36, QoLI-Dialysis). Finally, the item summaries examined across the patients informed the reporting and understanding of the measures of QoL within the Omani context and were used to make decisions about retention, amendment or deletion of individual items.
RESULTS
Characteristics of participants
Twelve participants were recruited from the Dialysis Unit. The mean (SD) of age was 53 (18.9), ranged from 28 to 76 year. Male patients constituted 75% of the total and 25% were female, while 66.7% were married, and 33.3% were single. Their education level status was: 33.3% illiterate, 8.3% low-intermediate level, 8.3% intermediate level, 25% high-intermediate level and 25% were college graduates. About one third of the patients were unemployed (33.3%) and housewives (16.7%), whereas the remainder were employed. The range of dialysis hours was 36-48 hrs/month.
The dialysis efficiency, based on the test of Urea Reduction Rate (URR), was >70 % (n=11) and only one was <70%. Table 2 shows a summary of the characteristics of the participants.
|
Characteristics |
Participants (n=12) |
|
|
Age [mean (range)]
|
Mean 47.58 Frequency |
SD 18.90 Percentage |
|
Gender Male Female |
9 3 |
75% 25% |
|
Marital status Married Single |
8 4 |
66.7% 33.3% |
|
Employment status Employed Unemployed |
8 4 |
66.7% 33.3% |
|
Educational level % High High-intermediate Intermediate Low-intermediate Illiterate |
3 3 1 1 4 |
25% 25% 8.3% 8.3% 33.3% |
Table 2: Characteristics of the sample.
Findings of SEIQoL-DW
Completion of the SEIQoL-DW: The Interview Record Form (IRF), the form used to record information about each participant during the interview, was subjectively analyzed for understanding, fatigue and overall validity. The IRF data, which was completed by the researcher immediately after interviews, indicated an acceptable time to complete the instrument (mean= 16.08 minutes), while the determined time to complete SEIQoL-DW is 10-20 minutes [14,29,41,42]. The least time taken to complete the tool was 12 minutes and the longest time was 21 minutes. The least time taken was scored by a 28-year-old male patient with a high education level and the longest by a 54-year-old illiterate female patient, suggesting that education level might reflect the level of understanding of SEIQoL-DW. Despite the age variation among the participants, low levels of fatigue were observed.
Three respondents had difficulty with rating negatively worded aspects in the y axis of “worst possible” and “best possible” related to the level of these aspects in the IRF. Similar difficulty was observed when participants were asked to mark the bar chart with a horizontal line to draw a box from baseline to the mark. This problem, however, was dealt with immediately by the researcher at the time of chart completion by reminding the respondent that the task was to rate ‘how each of these areas are for you now”.
The last challenge was encountered during the SEIQoL-DW administration with the interpretation of the “importance” of levels of areas of life on the five-weighted colored disk (pie chart). Out of the12 participants, six interpreted this step as “level of functioning” on their nominated cues rather than as“ importance” of cues to them. Here, respondents were reminded that the task was to indicate “how important each of the five aspects is at present, relative to each other”.
Description of frequency of elicited and prompted cues and categories: Fifty-nine cues were reported by patients. These cues were assigned categories by three independent raters (principal researcher, principal supervisor and second supervisor). Sixty per cent of the cues were assigned the same category by the three reviewers, 36% had the agreement of two reviewers and there was no agreement between the reviewers on 5% of the cues. Appendix 2 summaries cues definitions and categorization of cues. Of the 12 patients, nine patients (75%) nominated five cues without prompting, whereas three required prompting, of which one nominated four cues.
Once reviewers had assigned cues to categories, the percentage of patients nominating each category at least once is shown in table 3. The category of religion/spiritual life was mentioned most frequently, 12 times (100%) by 12 patients, whereas the category of family was nominated by nine patients (75%), six patients nominated personal health, social life and leisure activities (50%), five patients nominated work/occupation and role functioning (41.6%), three patients nominated autonomy/independence (25%) and 8.3% nominated each of these: family health, sexuality, finances, relationships, enjoying life and quality of care.
|
Category |
Number of Patients Nominating Categories (%) |
|
Religion/spiritual life |
12 (100) |
|
Family |
9 (75) |
|
Personal health |
6 (50) |
|
Social life |
6 (50) |
|
Leisure activities |
6 (50) |
|
Work/occupation |
5 (41.6) |
|
Role functioning |
5 (41.6) |
|
Autonomy/independence |
3 (25) |
|
Family health |
1 (8.3) |
|
Sexuality |
1 (8.3) |
|
Finances |
1 (8.3) |
|
Relationships |
1 (8.3) |
|
Enjoying life |
1 (8.3) |
|
Quality of care |
1 (8.3) |
Table 3: Number of patients nominating category and their percentages.
The content and variety of categories were as expected from reports in the literature. However, it was unique for this study that religious and spirituality issues were the most frequent and dominant among this group of patients. Having obtained the levels and weights for each of the nominated cues, the SEIQoL-DW index was calculated to provide an overall score, as shown in appendix3.This is a continuous measure ranging from 0 to 100. The minimum score was 33.92 and the maximum score was 79.25 (M=55.60, SD=13.59).
Additionally, respondents indicated their current life satisfaction on a visual analogue scale that ranged from 0=worst life imaginable, to 100=best life imaginable, as shown in table 4. The minimum score was 28 whereas the maximum was 95 (M=66.67, SD=20.61). In an attempt to examine if there is a possible correlation between the SEIQoL-DW index overall score and the visual analogue scale, a Pearson’s (r) test was conducted. The result showed that there was no correlation between the variables [r=0.117, n=12, p=0.358].
|
Instrument |
Participants |
|||||||||||
|
01 |
02 |
03 |
04 |
05 |
06 |
07 |
08 |
09 |
10 |
11 |
12 |
|
|
SEIQoL-DW overall score |
44.5 |
52.5 |
78.4 |
79.2 |
57.9 |
63.3 |
42.5 |
54.5 |
58.5 |
56.4 |
33.9 |
45.4 |
|
SEIQoL-DW linear analogue score |
28 |
84 |
31 |
85 |
76 |
77 |
53 |
95 |
70 |
74 |
63 |
64 |
Table 4: Scores of SEIQoL-DW overall score and SEIQoL-DW linear analogue score.
Example of cues, levels, direct weightings and overall score of SEIQoL-DW: This section provides an example of SEIQoL-DW result-nominated cues, levels and direct weights-of two patients, as shown in figures 3 and 4. The description of illustrated cues was recorded on the Cue definitions record form by the researcher at the time of interview. The descriptions of these cues reflect exclusively the patients’ explanations and not the researcher’s interpretation.
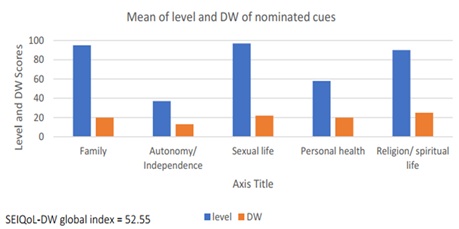 Figure 3: Level and direct weights of nominated cues (Patient One).
Figure 3: Level and direct weights of nominated cues (Patient One).
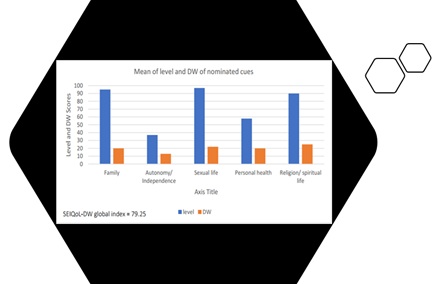 Figure 4: Level and direct weights of nominated cues (Patient Two).
Figure 4: Level and direct weights of nominated cues (Patient Two).
Patient One: A 58 years old married man with a low education level and worked in the private sector with a low income. He was able to nominate all the cues without prompting. The time taken for him to complete the SEIQoL-DW was 15 minutes. Table 5 shows the example of patient one description of cue, cue label and related category.
|
Cue label |
Description of cue |
Categorised in |
|
Cue 1: Family |
"... mixing with people and sitting with them. Sitting with friends, hanging out with them". |
Social life |
|
Cue 2: Body image |
"... physical activity, ability to go... shopping and get groceries. Ability to climb up the stirs". |
Role functioning |
|
Cue 3: Mobility |
"... transportation. Able to drive to places of interest is highly important to me. Also, ability to bank up the money required to this". |
Autonomy/Independence |
|
Cue 4: Self-development |
"I am youth and my future is not clear; the job as well! I don't know if I will find a job that suits my health condition and how my future will be?" |
Role functioning |
|
Cue 5: Religion |
"... going to mosque and praying to Allah 'Gob', fasting and being able to fast is highly important to me". |
Religion/spiritual life |
Table 5: Example of description of cue, cue label and related category (Patient One).
Patient two: A 53 years old married man. He had a high education level and worked for the government with a long-term contract and a good income level. He was able to nominate the five cues without prompting in a time of 15 minutes. Example of the description of cue, cue label and related category for the patient is shown in table 6.
|
Cue label |
Description of cue |
Categorised in |
|
Cue 1: Family |
"... my presence at home is very important to care for my wife and children. They are taking most of my life". |
Family |
|
Cue 2: Mobility |
"... going out from home and coming for dialysis; also getting groceries to home is important. These are all my responsibilities". |
Autonomy/Independence |
|
Cue 3: Sexual relationship |
"... it is important to me to care for my wife. Sexual life, for instance, I consider it as an important aspect in my life". |
Sexuality |
|
Cue 4: Health |
"... diseases; allergies from medications and secondary diseases. Basically, my health". |
Personal life |
|
Cue 5: Worship |
"... being on time for prayers, going to mosque; as well as going to Hajj, are important to me". |
Religion/spiritual life |
Table 6: Example of description of cue, cue label and related category (Patient One).
Findings of cognitive interviewing of the SF36 and QoLI-dialysis SF36v2: The aim for administering SF36v2 using the cognitive interviewing technique was to test the ability of the Omani patients to comprehend and respond to this measure. It was anticipated that, if patients were able to comprehend and respond to the items of the SF36v2, then this would indicate that it is a readable and acceptable HRQoL measure.
All the patients (n=12) completed SF36v2. However, regarding their response to SF36v2 items, six patients reported some difficulty and a lack of clarity with two items (Item-4b and Item-5b). Patients reported that these items were complex and contained complicated syntax, as shown in table 7. For the remaining items, patients were able to supply their answers without any difficulties. A summary of the identified problems across all participants related to SF36 items is presented in Appendix 4.
|
Items |
Question |
Summary of Problems Identified Across Participants |
|
Item 4b |
4. During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of your physical health. b. Accomplished less than you would have like.
|
Clarity: Identify problems related to communicating the intent or meaning of the question to the respondent. |
|
Item 5b |
5. During the past 4 weeks, how much of the time have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (such as feeling depressed or anxious)? b. Accomplished less than you would have like. |
Clarity: Identify problems related to communicating the intent or meaning of the question to the respondent. |
Table 7: Items 4b and 5b and identified problems related to SF36v2.
Item 4b asked respondents if they had “Accomplished less than they would like” in the past four weeks in relation to problems with their work or other regular daily activities as a result of their physical health. Only one patient expressed a lack of language clarity related to this item. He stated that it was “unclear”. However, when the interviewer repeated the question to the respondent, he was then able to comprehend it. Thus, the item appeared to have no problem and was clear to all patients. Similarly, item 5.b asked respondents if they had “Accomplished less than they would like” in the past four weeks in relation to problems with their work or other regular daily activities as a result of their emotional problems (e.g. feeling depressed or anxious). Half of the respondents (50%) expressed issues related to the clarity of the question, such as awkward or complicated syntax.
QoLI-dialysis: QoLI-Dialysis was also administered to patients for the purpose of assessing their ability to understand and read this measure. A summary of the identified problems across all participants related to QoLI-Dialysis items is presented in Appendix5. Patients, in general, appeared motivated to complete the QoLI-Dialysis. Of the 64 items of QoLI-Dialysis, three items were left without answer by three patients (one male, two female). These items were numbers eight and 27 from the“ satisfaction” part and item 12 from both the “satisfaction” and “importance” parts.
When patients were probed regarding their hesitation in answering these items, issues of clarity with item 8 and item 27 and of sensitivity with item 12 were reported. The issues related to clarity were on items that asked patients to indicate their satisfaction on “chances to live the period they wish for’” and chances to “have a happy future”. For example, participant M said: “I don’t know how I will be tomorrow! So how can I know how I am going to be after one or two years? This disease cannot be predictable in future.” The item that was reported to be “sensitive” asked participants to indicate the level of satisfaction and importance of their “sexual life” , as shown in table 8.
|
Items |
QOLI-Dialysis Items |
Summary of Problems Identified Across Participants |
|
Part 1 (satisfaction) |
||
|
Item 8 |
How satisfied are you with: Your chances of living as long as you would like? |
Clarity: Identify problems related to communicating the intent or meaning of the question to the respondent. |
|
Item 12 |
How satisfied are you with: Your sex life? |
Sensitive content (general): The question asks about a topic that is embarrassing, or very private. |
|
Item 27 |
How satisfied are you with: Your chances for a happy future? |
Clarity: Identify problems related to communicating the intent or meaning of the question to the respondent. |
|
Part 1 (importance) |
||
|
Item 12 |
How important to you is: Your sex life? |
Sensitive content (general): The question asks about a topic that is embarrassing, or very private. |
Table 8: Identified problems related to QoLI-Dialysis questionnaires.
To examine further the function of items that have issues with clarity and sensitivity and its variance with the total QoLI-Dialysis score, Cronbach’s alpha test was performed. Results showed that QoLI-Dialysis had good level of reliabilities, Cronbach’s α=0.870. However, if item 8 is deleted, Cronbach's α willlower to 0.859. Similarly, for item 12, if deleted, α will lower to 0.867, whereas for item 27, Cronbach's α remains at a similar level=0.870. Hence, it was decided to retain these items for use in phase two of this study. These findings suggest that these patients with ESKD understand the notion of QoL as evidenced by their ability to nominate five main aspects of life that they value most and to comprehend the measures of QoL.
DISCUSSION
In the present study, patients with ESKD appear to understand the concept of QoL. This understanding was clear from the result of SEIQoL-DW in which patients nominated“ religion/spirituality”, family”, “personal health”, “social life”, and “leisure activities” as the top five aspects of life that determined their QoL. Interestingly, this result is in keeping with findings in the literature that were conducted within Western context using SEIQoL-DW instrument, except for the“ religion/spirituality” aspect.
In a study conducted in Western Pennsylvania, USA, patients with ESKD nominated family, health, work, financial, and leisure as aspects of life they valued most [21]. Another study conducted in the UK among patients with chronic diseases found that family, health, leisure, home, money were the aspects of life that made up patients’ QoL [47]. These comparable findings may suggest that patients with ESKD view the aspects of personal health, socioeconomic, and leisure activities as important determinant of QoL.
Religion and spirituality seem to be an important aspect of life for some western patients and most of the patients in the middle east region. Middle east patients consider religion as the essential reference in dealing with everyday life. It can be said that religion can shape the way these view different aspects of life, including perceptions of health and illness. Muslim patients usually understand that illness, suffering and dying are part of their life and a test from Allah, “God”. Their perception is that no one can control how long they are going to live.
Thus, their perceptions about QoL may be associated with their religion and spiritual lives.This perception may be also associated with the aspect of “personal health” as the Islamic religion encourages individuals to live healthily, care for their families and support each other and such support might extend even to financial support. Such insight is instructed by the Holy book of Muslims (Qur’an): “O mankind we have created you male and female and have made you into nations and tribes so that you may know each other. Lo! The noblest of you in the sight of Allah is the one with piety or the one who is pious” (Al-Hujurat 49:13). However, the degree of religiosity in dialysis patients can be affected by the symptoms of ESKD and related treatment requirements.
The health system in Oman is very good and is highly evaluated by the World Health Organization and all aspect of medical care is provided for free to all the residents [5,6]. The hemodialysis is scheduled thrice weekly at the closet center to the patient’s home location. Yet, the need to attend dialysis sessions for an average of 12-15 hours per week could interrupt their worship schedules. Similarly, their ability to fast during the holy month of Ramadan (the fasting month in Islam) could be interrupted due to the dialysis sessions, medication and dietary requirements. All these factors may have an impact on their level of functional status and satisfaction with their religious practice and consequently on their level of overall QoL.
Patients of middle east live in large families and are considered an introverted type of community. Family, therefore, is vital from their cultural perspective. "The family is the nucleus of the society; whenever the nucleus is healthy and strong, so will be the whole structure" [48].
The main aim of marriage within middle east society is to establish a family and to have children. This creates an equally important role for both wife and husband in forming the family, although the wife will have a different role. Thus, it is not surprising that patients rank“ family” as one of the most important aspects of life which contributes towards their QoL. When sickness occurs, patients first get support from their families and it is the family who usually takes the sick person to hospital. They even work closely with healthcare providers to ensure that their family member gets the best care and the necessary psychological support. With such family support, it can be expected that HD patients consider “family” a high priority when assessing their QoL level.
Social life may be one of the most important aspects that determine QoL for Omani patients. In Oman, gender is likely to have an influence on a patient’s QoL, as men and women have different roles to play. Women, for instance, are not encouraged/expected to live alone and men should always be around to assist and give a hand in normal life activities. It is also highly recommended that women do not meet with a non-relative man due to cultural and religious reasons. The social position of women might affect their QoL as this could influence their feeling of self-value. In contrast to women’s social position, the male gender role might also influence men’s QoL as there are fewer restrictions on them socially. However, male patients with ESKD and on HD could be burdened by poor financial status if they are unemployed or if their job is affected by their health condition. Such changes in their normal life activities could affect their functional role and subsequently lower their level of QoL.
Patients with ESKD experience a number of disease- and treatment-related factors that restrict their lifestyle and undermine QoL. In contrast to transplant patients who perceive their condition to be less chronic [49,50], HD patients reported an uncertain future and limited personal freedom and control [51,52]. Loss of freedom might also cause wider implications in altering marital, family and social relationships [53,54]. Such instability in feelings caused by physical and psychological alterations in ESKD patients may lead to reluctance in predicting the level of their satisfaction with their future. This gets worse when patients attempt to have balance in their lives when trying to maintain their roles of function, worship practice and care of their family.
Patients were able to understand the SF36v2 measures and comprehend most of its items, but with less clarity on items 4b and 5b. Both questions asked patients if they had “Accomplished less than they would like” in the past four weeks in relation to problems with their work or other regular daily activities because of their physical and mental health. Although the question statement of both items (Items 4b and 5b) was similar in the English version, the translated question statement to Arabic was slightly different. The item 4b can be understood, in Arabic, as “Accomplished less than you want”, whereas item 5b translated as“ Accomplished less than you wish”. This convergence in the meaning of both items has perhaps led to issues of clarity. To the researcher’s knowledge, no studies have been conducted within Oman that tested the validity of SF36v2.
There were published studies that translated and validated SF36 into Arabic language such as in Tunisian and Saudi populations [55-59]. Both reported acceptable reliability and equivalence of both versions. It should be noted, however, that the Arabic language contains many dialects which significantly differ across Arabic countries. In North Africa, for instance, spoken Arabic may be incomprehensible to an Arabic speaker from the Levant or the Arab Gulf. Hence, existing variations in dialects of the Arabic language maybe a factor that affects the clarity of items 4b and 5b. Administering the SF36v2 to a larger group of from various countries including Omani patients may further explore the clarity issue.
The QoLI-Dialysis was also an acceptable measure to our patients. Two items, however, were possibly sensitive. These questions asked about sex lives and partnerships. This conclusion was reached when patients refrained from answering three items specifically related to this area of life. Sensitive items might lower the percentage of respondents who respond to the item truth fully. That is, this aspect affects questionnaires or survey outcomes in relation to: (a) overall response rates, (b) participants declining to respond to that particular sensitive item, and (c) also the accuracy of the respondent’s answer [44,60].
From a religious perspective, such as in middle east region, single men and women are forbidden to have any kind of sexual relationship before marriage. Even after marriage, this topic is considered a family secret and it is a taboo to share sexual-activity information outside the confines of the couple. The majority of patients may feel offended if they have been asked to share information about their sexual life, whether they are married or not. This perception is manifested in cognitive interviewing when the female participants are reluctant to answer orally to a male interviewer regarding items related to sexual life. A question can be raised here as to whether such reluctance might have been erased by self-reporting as opposed to an interview.
Different modes of administering QoL measures might affect data quality. Chang& Krosnick [61], in their comparison study between oral interviewing and self-administered measures, reported that self-administration can increase a respondent’s willingness to disclose sensitive information, compared with face to-face or telephone interviews. Greater anonymity offered in surveys has been reported to lead to high item response and more accurate reporting on sensitive topics such as behavior and relationships. These results, however, contradicted an earlier result, reported by researchers, which showed that item response in face-to-face interviews was higher [62,63]. The explanation for this was that interviewers motivate people to respond and interviewers have greater control over the situation, for instance, by ensuring that questions are answered and not missed. Such variance in this set of evidence suggests that certain features, and the choice, of the questionnaire-administration format depends on characteristics of the participants and on the study site.
From a cultural perspective, within a Western context, self-administration seems to improve the quality of reports about sexual behavior in surveys. Bowlingetal found that self-administration eliminated the gap between the results of men and women, decreasing the average number of sexual partners reported by men and increasing the average number reported by women [39,64]. Likewise, self-administration increases the reporting of socially undesirable behavior, such as illegal attitudes or sexual information, usually under-reported in surveys [65]. This, however, might not be the case in Arabic culture where sensitive items be socially unacceptable or socially undesirable. It is believed that, if confidentiality can be ensured when administering the questionnaires in the pilot study, the response rate to sensitive items might be improved. Also, it would be useful to explore the effects of different administration formats of QoL and HRQoL questionnaires on a large sample of patients with ESKD in our region.
There are a number of limitations that can be highlighted in this phase. First, the sample size was relatively small, n=12, which might affect the reliability of the results. Second, for patients waiting to commence their dialysis session, particularly those who are older, participating in such a study could be overwhelming. It was also observed that using “think aloud” technique could create a false milieu when the researcher was present in the room with participants; and also, that the patients have to talk aloud, which they may not normally do. However, overall, the approach used to answer the RQ1 was shown to be applicable and useful.
The cognitive interview method revealed how patients understand the questions of the HRQoL measures. Likewise, SEIQoL-DW appeared to be relevant in exploring the meaning of QoL among this group of patients. In fact, the nominated aspects of life by patients were alike in the domains of the SF36v2 and QoLI-D measures, e.g. psychological and social aspects which may be indicating that the SEIQoL DW is measuring QoL on a subjective level. This result may represent a small step towards validating the SEIQoL-DW in patients with ESKD.
CONCLUSION
Two methods, the individual QoL instrument and cognitive interviewing, were used to explore the understanding of the concept of QoL in the population and to address the potential drawbacks of HRQoL instruments that might limit the factors that comprise participants’ QoL. The nominated aspects of life- Religion and Spiritual Life, Family, Personal Health, Social Life, and Leisure Activities- contribute significantly to the level of QoL in our ESKD patients. Within this group of patients, QoL is a cultural construct that is impacted by social and life events. Findings also show that QoL is an individualized perception and the individual experience is shaped and influenced by the society’s values and culture. Hence, it is recommended that the level of the effect of these aspects on QoL and HRQoL in this group of patients should be measured. Thus, incorporating and considering these aspects in assessing QoL and HRQoL in phases two and three of this project is recommended in order to enrich its outcomes including a separate measure that assesses spirituality domain.
Results suggest that the patients understand the notion of QoL and this is clearly manifested by their ability to nominate the aspects of life that they consider most important. The SEIQoL-DW revealed a reasonable lay definition of QoL in patients with ESKD within this population. Nominated aspects of life by ESKD patients could be a reliable guide to most important priorities for medical interventions by nephrologist, nephrology nurses, as well as policy makers within the healthcare system.
The association between spirituality domain and health related QoL should be considered in the main study. The degree of religiosity in dialysis patients can be affected by the symptoms of ESKD and related treatment requirements. This can be manifested by the frequent attendance at HD treatment (12 to 15 hours per week) which can interrupt their religious rituals such worship and fasting. These are some possible factors that may have an impact on their satisfaction and level of physical and role functioning status.
The influence of religion and spirituality manifested clearly through the cognitive interviewing method. Although it revealed that our patients comprehended the QoL and HRQoL questionnaires (Arabic versions), with a very good response rate to both measures (SF36 and QoLI-Dialysis), they were sensitive to items related to sexual life and partnerships. The low level of response to sensitive items may be attributed to the method of face-to-face interviewing. Cultural and religious factors in Oman, and the region of middle east at large, could influence patients’ responses to such questions as it is considered taboo to discuss sensitive subjects, such as sexual life, with anyone other than partners. One possible way to overcome this issue is to administer the measures in a larger sample size and to use a different method of administration, such as self-completion.
COMPLIANCE WITH ETHICAL STANDARDS
Disclosure of potential conflicts of interest
The study was approved by the Directorate of Research and Ethical Review and Approve Committee, Ministry of Health, Oman, MH/DGP/R&S/PROPOSAL_APPROVAL/16/2015and certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments ethical standards. https://mohcsr.gov.om/my-researches/
Informed consent
Each participant was freely given, informed consent to undergo various assessment and laboratory investigations.
Availability of data and material
Data of this paper is not available publicly but can be requested from the corresponding author in a reasonable time.
Funding
No funding available for both authors.
Conflict of interest
Authors declare no conflict of interest.
Acknowledgment
We would like to thank all our patients for their trust on us. Also, authors appreciate all the help and support of the Ministry of Health, Muscat, Oman. In addition, we would like to thank all the staff responsible for the delivery of patients’ care.
REFERENCES
- Al Alawi I, Al Salmi I, Al Mawali A, Al Maimani Y, Sayer JA (2017) End-stage kidney failure in Oman: An analysis of registry data with an emphasis on congenital and inherited renal diseases. Int J Nephrol 2017: 6403985.
- Al Alawi IH, Al Salmi I, Al Mawali A, Sayer JA (2017) Kidney disease in Oman: A view of the current and future landscapes. Iran J Kidney Dis 11 :263-270.
- Al Ismaili F, Al Salmi I, Al Maimani Y, Metry AM, Al Marhoobi H, et al. (2017) Epidemiological transition of end-stage kidney disease in Oman. Kidney Int Rep 2: 27-35.
- Al Majarfi A, Al Salmi I, Metry AM, Al Ismaili F, Hola A, et al. (2018) Epidemiology of patients at initial treatment with hemodialysis. ARC Journal of Nephrology 3: 6-12.
- Al Salmi I, Hannawi S (2016) The World Health Report-health systems empowering citizens and improving performance. Research on Humanities and Social Sciences 6.
- Al Salmi I, Hannawi S (2018) Health workforce in the sultanate of Oman: Improving performance and the health system. J Int Med Pat Care 1: 101.
- Alshaaili K, Al Salmi I, Metry AM, Al Ismail M, Hola A, et al. (2018) The epidemiology of hemolytic uremic syndrome: Clinical presentation, laboratory findings, management and outcomes. Int J Hematol Blo Dis 3: 1-6.
- Soni RK, Weisbord SD, Unruh ML (2010) Health-related quality of life outcomes in chronic kidney disease. Curr Opin Nephrol Hypertens 19: 153-159.
- Mujais SK, Story K, Brouillette J, Takano T, Soroka S, et al. (2009) Health-related quality of life in CKD Patients: Correlates and evolution over time. Clin J Am Soc Nephrol 4: 1293-1301.
- Bergland A, Narum I (2007) Quality of life: Diversity in content and meaning 19: 115-139.
- Hall T, Krahn GL, Horner-Johnson W, Lamb G, Rehabilitation R, et al. (2011) Examining functional content in widely used health-related quality of life scales. Rehabil Psychol 56: 94-99.
- Carr AJ, Higginson IJ (2001) Are quality of life measures patient centred? BMJ 322: 1357-1360.
- Tavernier SS, Totten AM, Beck SL (2011) Assessing content validity of the patient generated index using cognitive interviews. Qualitative Health Research 21: 1729-1738.
- Joyce C, O’boyle C, McGee H (1999) Individual quality of life: Approaches to conceptualisation and assessment. Harwood Academic Publishers, London, UK.
- Gall TL, Malette J, Guirguis-Younger M (2011) Spirituality and religiousness: A diversity of definitions. Journal of Spirituality in Mental Health 13: 158-181.
- Kaasa S, Loge JH (2003) Quality of life in palliative care: Principles and practice. Palliat Med 17: 11-20.
- Krethong P, Jirapaet V, Jitpanya C, Sloan R (2008) A causal model of health-related quality of life in Thai patients with heart-failure. J Nurs Scholarsh 40: 254-260.
- Fang W, Ni Z, Qian J (2014) Key factors for a high-quality peritoneal dialysis program--the role of the PD team and continuous quality improvement. Perit Dial Int 34: 35-42.
- Panzini RG, Maganha C, Rocha NS, Bandeira DR, Fleck MP (2011) Brazilian validation of the quality of life instrument/spirituality, religion and personal beliefs. Rev Saude Publica 45: 1531-65.
- Crosby RD, Kolotkin RL, Williams GR (2003) Defining clinically meaningful change in health-related quality of life. J Clin Epidemiol 56: 395-407.
- Abdel-Kader K, Unruh ML, Weisbord SD (2009) Symptom burden, depression, and quality of life in chronic and end-stage kidney disease. Clin J Am Soc Nephrol 4: 1057-1064.
- Paul CB, Willis GB (2007) Research synthesis: The practice of cognitive interviewing. The Public Opinion Quarterly 71: 287-311.
- Willis G (2006) Cognitive interviewing as a tool for improving the informed consent process. J Empir Res Hum Res Ethics 1: 9-24.
- Willis G, Zahnd E (2007) Questionnaire design from a cross-cultural perspective: An empirical investigation of Koreans and non-Koreans. J Health Care Poor Underserved 18: 197-217.
- Elliott MN, Brown JA, Lehrman WG, Beckett MK, Hambarsoomian K, et al. (2012) A randomized experiment investigating the suitability of speech-enabled IVR and web modes for publicly reported surveys of patients’ experience of hospital care. Medical Care Research and Review 70: 165-184.
- Commarford PM, Lewis JR, Smither JA, Gentzler MD (2008) A comparison of broad versus deep auditory menu structures. Hum Factors 50: 77-89.
- Elliott MN, Brown JA, Lehrman WG, Beckett MK, Hambarsoomian K, et al. () A randomized experiment investigating the suitability of speech-enabled IVR and Web modes for publicly reported surveys of patients' experience of hospital care. Med Care Res Rev 70: 165-184.
- Galesic M, Tourangeau R, Couper MP (2006) Complementing random-digit-dial telephone surveys with other approaches to collecting sensitive data. Am J Prev Med 31: 437-443.
- McGee HM, O'Boyle CA, Hickey A, O'Malley K, Joyce CR (1991) Assessing the quality of life of the individual: The SEIQoL with a healthy and a gastroenterology unit population. Psychol Med 21: 749-759.
- Becker G, Merk CS, Meffert C, Momm F (2014) Measuring individual quality of life in patients receiving radiation therapy: The SEIQoL-Questionnaire. Qual Life Res 23: 2025-2030.
- Kolewaski CD, Mullally MC, Parsons TL, Paterson ML, Toffelmire EB, et al. (2005) Quality of life and exercise rehabilitation in end stage renal disease. CANNT J 15: 22-29.
- Picariello F, Hudson JL, Moss-Morris R, Macdougall IC, Chilcot J (2017) Examining the efficacy of social-psychological interventions for the management of fatigue in End-Stage Kidney Disease (ESKD): A systematic review with meta-analysis. Health Psychol Rev 11: 197-216.
- Picariello F, Moss-Morris R, Macdougall IC, Chilcot J (2018) 'It's when you're not doing too much you feel tired': A qualitative exploration of fatigue in end-stage kidney disease. Br J Health Psychol 23: 311-333.
- Picariello F, Moss-Morris R, Macdougall IC, Norton S, Da Silva-Gane M, et al. (2018) Cognitive-Behavioural Therapy (CBT) for renal fatigue (BReF): A feasibility randomized-controlled trial of CBT for the management of fatigue in Haemodialysis (HD) patients. BMJ Open 8: 020842.
- Ferrans CE, Powers MJ (1985) Quality of life index: Development and psychometric properties. ANS Adv Nurs Sci 8: 15-24.
- Ferrans CE, Powers MJ (1993) Quality of life of hemodialysis patients. ANNA J 20: 575-581.
- Ferrans CE, Powers MJ (2007) Quality of life index: development and psychometric properties. Rech Soins Infirm 88: 32-37.
- Bowling A (1995) The concept of quality of life in relation to health. Med Secoli 7: 633-645.
- Bowling A, Hankins M, Windle G, Bilotta C, Grant R (2013) A short measure of quality of life in older age: The performance of the brief Older People's Quality of Life questionnaire (OPQOL-brief). Arch Gerontol Geriatr 56: 181-187.
- Bowling A, Seetai S, Morris R, Ebrahim S (2007) Quality of life among older people with poor functioning. The influence of perceived control over life. Age Ageing 36: 310-315.
- Ciaran OB, John B, Anne H, Hannah M, CRB J (1995) The Schedule for the Evaluation of Individual Quality of Life (SEIQoL): A Direct Weighting procedure for Quality of Life Domains (SEIQoL-DW). Administration Manual.
- O'Boyle CA BJ, Hickey A, McGee HM, Joyce CRB (1993) The Schedule for the Evaluation of Individual Quality of Life (SEIQoL): A Direct Weighting procedure for Quality of Life Domains (SEIQoL-DW).
- Bowling CB, Zhang R, Franch H, Huang Y, Mirk A, et al. (2015) Underreporting of nursing home utilization on the CMS-2728 in older incident dialysis patients and implications for assessing mortality risk. BMC Nephrol 16: 32.
- Tourangeau R, Yan T (2007) Sensitive questions in surveys. Psychol Bull 133: 859-883.
- Willis GB, Lessler JT (1999) Question appraisal system QAS-99. Questionnaire Pretesting Methods.
- Knafl K, Deatrick J, Gallo A, Holcombe G, Bakitas M, et al. (2007) The analysis and interpretation of cognitive interviews for instrument development. Res Nurs Health 30: 224-234.
- Mountain LA, Campbell SE, Seymour DG, Primrose WR, Whyte MI (2004) Assessment of individual quality of life using the SEIQoL-DW in older medical patients. QJM 97: 519-524.
- Ohm R (2003) The African American experience in the Islamic faith. Public Health Nursing 20: 478-486.
- Edalat-Nejad M, Qlich-Khani M (2013) Quality of life and sleep in hemodialysis patients. Saudi J Kidney Dis Transpl 24: 514-518.
- Bakewell AB, Higgins RM, Edmunds ME (2001) Does ethnicity influence perceived quality of life of patients on dialysis and following renal transplant? Nephrol Dial Transplant 16: 1395-1401.
- Amro A, Waldum B, von der Lippe N, Brekke FB, Dammen T, et al. (2015) Symptom clusters predict mortality among dialysis patients in Norway: A prospective observational cohort study. J Pain Symptom Manage 49: 27-35.
- Brekke FB, Waldum B, Amro A, Østhus TBH, Dammen T, et al. (2014) Self-perceived quality of sleep and mortality in Norwegian dialysis patients. Hemodial Int 18: 87-94.
- Christensen AJ, Ehlers SL (2002) Psychological factors in end-stage renal disease: An emerging context for behavioral medicine research. J Consult Clin Psychol 70: 712-724.
- Christensen AJ, Raichle K, Ehlers SL, Bertolatus AJ (2002) Effect of family environment and donor source on patient quality of life following renal transplantation. Health Psychol 21: 468-476.
- Algarni AS, Ghorbel S, Jones JG, Guermazi M (2014) Validation of an Arabic version of the Oswestry index in Saudi Arabia. Ann Phys Rehabil Med 57: 653-663.
- Guermazi M, Allouch C, Yahia M, Huissa TB, Ghorbel S, et al. (2012) Translation in Arabic, adaptation and validation of the SF-36 health survey for use in Tunisia. Ann Phys Rehabil Med 55: 388-403.
- Coons SJ, Alabdulmohsin SA, Draugalis JR, Hays RD (1998) Reliability of an Arabic version of the RAND-36 health survey and its equivalence to the US-english version. Medical Care 36: 428-432.
- Alshehri A, Lohman E, Daher NS, Bahijri K, Alghamdi A, et al. (2017) Cross-cultural adaptation and psychometric properties testing of the arabic anterior knee pain scale. Med Sci Monit 23: 1559-1582.
- Al-Sobayel HI, Al-Hugail HA, AlSaif RM, Albawardi NM, Alnahdi AH, et al. (2016) Validation of an Arabic version of fatigue severity scale. Saudi Med J 37: 73-78.
- Tourangeau R, Yan T, Sun H, Hyland A, Stanton CA (2019) Population Assessment of Tobacco and Health (PATH) reliability and validity study: Selected reliability and validity estimates. Tob Control 28: 663-668.
- Chang L, Krosnick JA (2010) Comparing oral interviewing with self-administered computerized questionnaires an experiment. Public Opinion Quarterly 74: 154-167.
- Edwards P, Roberts I, Sandercock P, Frost C (2004) Follow-up by mail in clinical trials: Does questionnaire length matter? Control Clin Trials 25: 31-52.
- Edwards PJ, Roberts I, Clarke MJ, Diguiseppi C, Wentz R, et al. (2009) Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst Rev 9: MR000008.
- Bowling A (2005) Mode of questionnaire administration can have serious effects on data quality. J Public Health 27: 281-291.
- Cope AB, Ramirez C, DeVellis RF, Agans R, Schoenbach VJ, et al. (2016) Measuring concurrency attitudes: Development and validation of a vignette-based scale. PLoS One 11: 0163947.
APPENDIX
For appendix file please click below link:
https://www.heraldopenaccess.us/fulltext/Nephrology-&-Renal-Therapy/HNRT-20-024-Appendix.docx
Citation: Al-Rajhi W, Al Salmi I (2020) Quality of Life and Health-Related Quality of Life Among End-Stage Kidney Disease Patients: Testing the Concepts and Assessing the Measures. J Nephrol Renal Ther 6: 041.
Copyright: © 2020 Waleed Al-Rajhi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.