Rare Case of a Newborn with Heterotaxy Syndrome, Right Aortic Arch and an Isolated Left Brachiocephalic Artery Arising from a Left Ductus Arteriosus
*Corresponding Author(s):
Lawrence E GreitenDivision Of Pediatric Cardiothoracic Surgery, Arkansas Children’s Hospital, Little Rock, Arkansas, United States
Tel:+1 5013645858,
Email:LGreiten@uams.edu
Abstract
Heterotaxy is an abnormal arrangement of viscera across the left-right axis of the body often associated with a variety of complex cardiac lesions. We present a case of left isomeric heterotaxy, a right aortic arch, and a left brachiocephalic artery arising from a left ductus arteriosus.
Keywords
Heterotaxy; Left atrial isomerism; Right aortic arch
Introduction
Heterotaxy syndrome is a complex set of abnormalities related to arrangements of the internal thoracic-abdominal structures across the left-right axis. The reported incidence is 1-1.5 in 10,000 live births.Right-sided aortic arch with isolation of the innominate artery is an extremely rare congenital anomaly, in which the innominate artery loses its connection with the ascending aorta and is supplied by either a patent ductus or mediastinal collaterals [1]. Here we are presenting a case with left isomeric heterotaxy and a left brachiocephalic artery arising from a left ductus arteriosus in connection with the left pulmonary artery.
Case Report
An infant was prenatally diagnosed with a moderately unbalanced AV canal with large atrial and ventricular component, mild Atrioventricular Valve (AV) regurgitation, bilateral superior vena cava without bridging vein, ipsilateral pulmonary venous return, and subaortic obstruction by fetal echocardiogram. The infant was born at 39 weeks gestational agevia spontaneously delivery. Her APGAR scores were 9 at both 1and 5 minutes of life. Prostaglandin 0.01mcg/kg/min was initiated immediately after delivery and she was transferred to CVICU breathing comfortably with oxygen saturations 98% on room air. Her birth weight was 2690g (6th percentile), length was 47cm (11th percentile) and head circumference was 32cm (3rd percentile).
Investigation
Postnatal echocardiogram demonstrated a complete atrioventricular canal defect (moderately unbalanced with inflow commitment greater toward the left) and moderately hypoplastic right ventricle. There was a large atrial and ventricular component of the atrioventricular canal with moderate common AV valve regurgitation. The aortic arch was noted to be right sided with bilateral ductus arteriosus. The aortic valve was mildly hypoplastic and the main pulmonary artery moderately dilated along with suspicion for a single coronary artery. Additionally, there was significant subaortic narrowing and an elongated left ventricular outflow tract. The patient was also noted to have bilateral superior vena cava returning to the superior aspect of the ipsilateral atrium without a bridging vein. Ipsilateral pulmonary venous return was seen with right upper pulmonary vein returning to the superior aspect of the right atrium and right lower returning to the inferior aspect of the right atrium, with the mirror image pattern occurring with the left pulmonary veins.
Surprisingly, her abdominal ultrasound showed “normal” sidedness of her internal organs.
To better visualize the venous, great vessel, and coronary anatomy, she underwent a Cardiac-Gated Computed Tomography (CTA) scan in preparation for surgical palliation. CTA showed ipsilateral hepatic venous drainage with the right hepatic veins joining an intact right sided inferior vena cava drained into the right atrium. The left hepatic veins became confluent and drained into the left atrium. The previously noted right aortic arch was mildly hypoplastic and gave rise to the right common carotid and right subclavian arteries. This right sided arch showed no evidence of coarctation. An isolated left brachiocephalic artery was discovered, which arose from the left sided ductus arteriosus. The base of the left ductus was stenotic at its proximal portion arising from the main pulmonary artery near the proximal left pulmonary artery origin. There was also a large right sided ductus that originated from the proximal descending aorta inserting on the main pulmonary artery near the right pulmonary artery origin. The atrial appendage morphology was ambiguous being both broad based but also elongated (Figures 1-4).
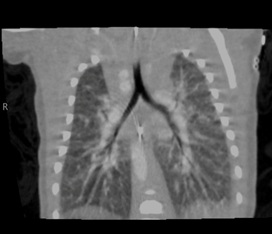 Figure 1: CT demonstrating bilateral hyparterial bronchi consistent with left atrial isomerism.
Figure 1: CT demonstrating bilateral hyparterial bronchi consistent with left atrial isomerism.
 Figure 2: CT demonstrating moderately unbalanced AV canal with left ventricular dominance, large primum ASD, large inlet VSD and ipsilateral pulmonary venous return of right and left lower pulmonary veins.
Figure 2: CT demonstrating moderately unbalanced AV canal with left ventricular dominance, large primum ASD, large inlet VSD and ipsilateral pulmonary venous return of right and left lower pulmonary veins.
 Figure 3: Cardiac CT 3D model demonstrating a right aortic arch (double arrow) giving rise to a right common carotid artery and right subclavian artery. This model also demonstrates the isolated left brachiocephalic artery which arises from the left sided patent ductus arteriosus (arrow).
Figure 3: Cardiac CT 3D model demonstrating a right aortic arch (double arrow) giving rise to a right common carotid artery and right subclavian artery. This model also demonstrates the isolated left brachiocephalic artery which arises from the left sided patent ductus arteriosus (arrow).
 Figure 4: Cardiac CT 3D model demonstrating ipsilateral hepatic venous drainage (arrow), ipsilateral pulmonary venous return and bilateral superior vena cava (double arrow).
Figure 4: Cardiac CT 3D model demonstrating ipsilateral hepatic venous drainage (arrow), ipsilateral pulmonary venous return and bilateral superior vena cava (double arrow).
Treatment And Outcome
The infant became progressive lytachypneic secondary to pulmonary over circulation for which respiratory support was escalated to high flow oxygen at 6LPM FiO2 21%. Due to significant left ventricular outflow tract obstruction, a mildly hypoplastic right sided transverse arch, and complex venous anatomy; single ventricle palliation was deemed the most appropriate surgical intervention to provide hemodynamic stability. She subsequently underwent a Damus-Kaye-Stansel (DKS) amalgamation with arch augmentation, Sano shunt placement from the right ventricle to the main pulmonary artery and left brachiocephalic artery re-implantation. She tolerated the procedure well (Figure 5).
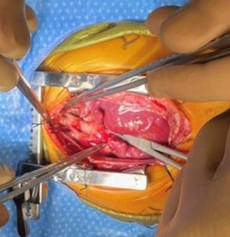 Figure 5: Interoperative image of great artery anatomy.
Figure 5: Interoperative image of great artery anatomy.
Postoperative transthoracic echocardiogram showed unobstructed egress from left ventricle through VSD to the neoaortic valve and into the DKS reconstructed arch as well as unobstructed flow in the Sano conduit. Ventricular function was normal and AV valve function was unchanged being reported as moderate regurgitation.
Discussion
Morphologically, this patient’s classification as either left (polysplenic) or right (asplenic) heterotaxy syndrome is controversial, as is the case with many heterotaxy patients [2]. The bronchial pattern and ipsilateral pulmonary veins support a diagnosis of left isomerism, however, an intact right sided inferior vena cava was more consistent with right atrial isomerism. Her ambiguous atrial morphology was not a helpful categorizing feature, nor was the abdominal organ orientation. Ultimately, we elected to classify the patient as having left sided atrial isomerism based on her bronchial and pulmonary venous anatomy.
The most distinguishing and rare feature of this case is the isolated left brachiocephalic artery anatomy. The case highlights the fact that the aortic arch and head and neck vessels are subject to abnormal symmetric pattering as is the venous, bronchial and abdominal structures in patients with heterotaxy syndrome. The aortic arch undergoes differentiation and regression before typical head and neck vessel formation. D’Cruz, et al. reported the first case of right aortic arch and isolation of left innominate artery in 1966 [3]. A right aortic arch, defined as aortic arch traversing the right bronchus, occurs due to the persistence of the right dorsal aorta with the regression of the left dorsal aorta [4]. The two most common type of a right-sided arch is that with mirror image branching (a left brachiocephalic trunk, right common carotid, and right subclavian artery arising from the arch), or a right aortic arch with an aberrant left subclavian artery. In this rare presentation of an isolated left brachiocephalic artery arising from a left sided ductus arteriosus, the possible embryologic mechanisms remain ill defined.
Currently the long-term overall outcome of left isomerism heterotaxy have not been well documented. Arecent study reports that AV valve regurgitation and anomalous pulmonary venous connection are considered to be the most important contributors to increased mortality in patients with heterotaxy syndrome who undergo single ventricle palliation [5]. The patient in case will require ongoing monitoring for these potential cardiovascular problems.
References
- Mangukia C, Sethi S, Agarwal S, Mishra S, Satsangi DK (2014) Right aortic arch with isolation of the left innominate artery in a case of double chamber right ventricle and ventricular septal defect. Ann Pediatr Cardiol 7: 148-151.
- Hastreiter AR, D'Cruz IA, Cantez T, Namin EP, Licata R (1996) Right-sided aorta. I. Occurrence of right aortic arch in various types of congenital heart disease. II. Right aortic arch, right descending aorta, and associated anomalies. Br Heart J 28: 722-739.
- Hanneman K, Newman B, Chan F (2017) Congenital variants and anomalies of the aortic arch. Radio Graphics 37: 32-51.
- Smith A, McKay R (2004) Atrial arrangement(situs)/Isomerism/Juxtaposition. In: A practical atlas of congenital heart disease. 1st edn London. Springer-Verlag London Ltd. Page no: 41-52.
- Lee SH, Kwon BS, Kim GB, Bae EJ, Noh CI, et al. (2016) Clinical Characteristics and Independent Factors Related to Long-Term Outcomes in Patients with Left Isomerism. Korean Circ J 47: 501-508.
Citation: Xu W, Merves S, Arthur L, Zakaria D, Reemtsen B, et al. (2021) Rare Case of a Newborn with Heterotaxy Syndrome, Right Aortic Arch and an Isolated Left Brachiocephalic Artery Arising from a Left Ductus Arteriosus. J Angiol Vasc Surg 6: 064.
Copyright: © 2021 Wenyuan Xu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.