Sandwich EVAR is Salvageable Technique in Juxtarenal AAA
*Corresponding Author(s):
Supatcha PrasertcharoensukDepartment Of Surgery, Khon Kaen University, Khon Kaen, Thailand
Tel:+66 43363252,
Fax:+66 43363252
Email:supatcha.p@gmail.com
Abstract
The most common technical concern in Endovascular Aneurysm Repair (EVAR) is the proximal landing zone of stent. Sandwich technique is the effective procedure to preserve internal iliac blood flow. This case report describes using this procedure for successful EVAR in patient with juxtarenal abdominal aortic aneurysm.
Keywords
Abdominal aortic aneurysm; Juxtarenal abdominal aortic aneurysm; Sandwich technique
Introduction
Sandwich EVAR technique was used to preserve internal iliac artery when iliac branch device was not suitable [1,2]. There are several reports using this technique in thoracoabdominal aortic aneurysm for extending proximal landing zone with visceral profusion [3,4]. We apply it for juxtarenal abdominal aortic aneurysm that renal artery is in upward angle that is difficult to cannulate from above and may compromise flow to renal artery if chimney from brachial approach in this patient. The patient provided written informed consent for the report of the details and images related to his case.
Case Presentation
A 72-year-old man with hypertension and diabetes mellitus complained of severe abdominal pain was referred to our hospital with a 52 mm juxtarenal abdominal aortic aneurysm. Imaging information of this patient is shown in Figure 1. Computed tomography angiography revealed a juxtarenal AAA with maximum diameter 52 mm with intramural thrombus and periaortic fat stranding anteriorly (Figure 1A, 1B & 1C). The images also demonstrated narrowest part of aortic neck and 60 degrees angulation (Figure 1D).
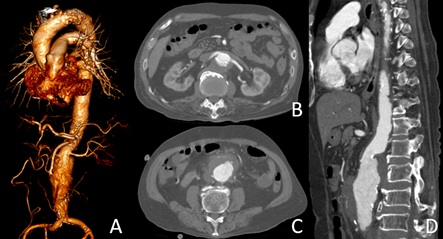
Figure 1: (A) 3D reconstruction shows short and angulation of aortic neck. (B) The narrowest part of aorta with mural thrombus. (C) Infrarenal aortic aneurysm part that contains mural thrombus and peri aortic fat stranding anteriorly.
Owing to small angulate aortic neck demonstrate in Figure 2A, the narrowest diameter was 18.5 mm. The proximal landing zone from below celiac trunk to superior edge of aneurysm was 24 mm in length (Figure 2B). In the beginning, we planned to do 3 chimney EVAR, after we cannulated left renal artery successfully, but unable to put the long sheath through renal artery due to tortuosity of suprarenal aorta and infrarenal angulation even though we used balloon assist from below. We changed the plan to do sandwich EVAR, infrarenal aorta diameter in the first 5 mm was 33 mm and suprarenal aorta diameter was 20-25 mm.The first step was performed by two target vessels (Superior mesenteric artery and right renal artery) were catheterized through left axillary conduit (8 mm Dacron graft) with 7-F, 55-cm-long sheath and two balloon expandable stents (Begraft; Bentley InnoMed, Hechingen, Germany) 8 mm and 6 mm were placed consequently (Figure 3A & 3B). As usually, coming from below, a bifurcate aortic endograft ETBF3616C145EE (Endurant; Medtronic Vascular, Santa Rosa, CA, USA) was first deployed just below lowest renal artery, contralateral limb was cannulated then an iliac limb extension ETLW1613C93EE was inserted through contralateral femoral access. Ipsilateral limb was inserted through left femoral access after completing deployed of main device. Left renal artery was approached from below with 7-F, 55 cm-long sheath and a 6 mm balloon expandable stent was located. An aortic cuff was deployed between flow divider of the bifurcate graftand celiac trunk, all 3 balloon expandable stents were deployed simultaneously and balloon molding all stents with kissing technique (Figure 3C&3D). Lastly, to prevent kinking of snorkel left renal artery, we reenforced with self-expandable stent (Eluvia; Boston Scientific, Natick, MA, USA) (Figure 3E). Completion aortogram showed visceral vessels patency without any endoleak (Figure 3F).
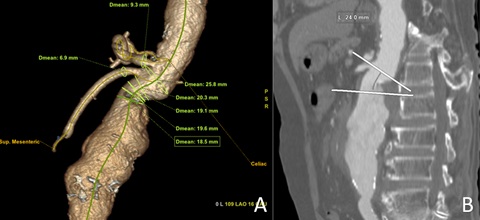 Figure 2: A) 3d reconstruction shows diameter of aortic neck; B) Sagittal view demonstrate neck length from below celiac to aneurysm.
Figure 2: A) 3d reconstruction shows diameter of aortic neck; B) Sagittal view demonstrate neck length from below celiac to aneurysm.
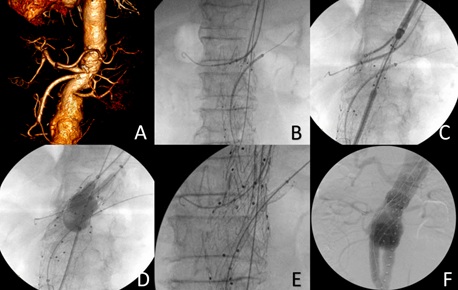 Figure 3: A) 3D reconstruction demonstrates narrow aortic neck and upward renal angle; B) Intraoperative angiography showing 3 long sheaths with balloon expandable stents in places; C) Aortic cuff placement between celiac and flow divider of the graft; D) Molding graft with kissing technique; E) Reenforce left renal stent with self-expandable stent; F) Complete aortogram confirms no endoleak with visceral flow preservation.
Figure 3: A) 3D reconstruction demonstrates narrow aortic neck and upward renal angle; B) Intraoperative angiography showing 3 long sheaths with balloon expandable stents in places; C) Aortic cuff placement between celiac and flow divider of the graft; D) Molding graft with kissing technique; E) Reenforce left renal stent with self-expandable stent; F) Complete aortogram confirms no endoleak with visceral flow preservation.
Total procedure time was 250 minutes (fluoroscopic time was 60 minutes), contrast volume was 150 mL, and estimate blood loss was 600 mL. The post-operative CTA demonstrated stent in sandwich configuration without visceral stent occlusion (Figure 4A, 4B & 4C) and no endoleak but left retroperitoneal hematoma (Figure 4D). The hospital stay was 9 days, patient was discharged with dual antiplatelet therapy.
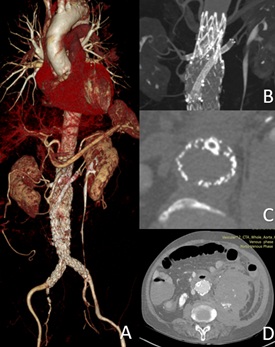 Figure 4: A) Post-operative 3D reconstruction shows stent patency; B) Stent configuration depicts snorkel in left renal artery; C) Cross section reveals sandwich of left renal stent; D) Left retroperitoneal hematoma post-operatively.
Figure 4: A) Post-operative 3D reconstruction shows stent patency; B) Stent configuration depicts snorkel in left renal artery; C) Cross section reveals sandwich of left renal stent; D) Left retroperitoneal hematoma post-operatively.
Discussion
Total endovascular treatment of juxtarenal AAA in emergency setting that on the shelf device is not available is a challenging situation to modify all devices and techniques to exclude aneurysmal sac from circulation. Adjunctive procedure such as endo-anchor, chimney, sandwich or physician-modified fenestrated endograft was added to standard Endovascular Aneurysm Repair (EVAR) in order to fit complex anatomy of each patient [5-8]. Postoperative Acute Kidney Injury (AKI) is associated with increase mortality, we attempted to preserve good flow to both kidneys, left renal artery was unable to place long sheath from above, so snorkel with sandwich technique was done.
The sandwich technique is an another technique to facilitate EVAR feasibility in the setting of challenging proximal landing zone. Its main advantages include no visceral flow jeopardize when deploy physician-modified fenestrate endograft and suprarenal aortic tortuosity that makes difficult manipulation of devices from above.
Conclusion
The sandwich technique is a salvageable technique for tough situation in EVAR. Mix and match of endovascular device is needed.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgment
The authors would like to thank (a) Prof. Kittisak Sawanyawisuth for assistance with writing this manuscript, and (b) all staffs from department of operating room nursing, Srinagarind hospital for assistance with operation.
References
- Lobato AC (2011) Sandwich technique for aortoiliac aneurysms extending to the internal iliac artery or isolated common/internal iliac artery aneurysms: a new endovascular approach to preserve pelvic circulation. J Endovasc Ther 18: 106-111.
- Massmann A, Mosquera Arochena NJ, Shayesteh-Kheslat R, Buecker A (2016) Endovascular anatomic reconstruction of the iliac bifurcation with covered stentgrafts in sandwich-technique for the treatment of complex aorto-iliac aneurysms. Int J Cardiol 222: 332-339.
- Prasertcharoensuk S, Wongkonkitsin N, Tunmit P, Theeragul SA, Ahooja A (2018) Sandwich EVAR occludes Celiac and Superior Mesenteric Artery for Infected Suprarenal Abdominal Aortic Aneurysm Treatment. Case Rep Vasc Med 2018: 4037683.
- Marchal J, Verhelst R, Astarci P, Elens M (2021) Endovascular Repair of a Ruptured Thoracoabdominal Aortic Aneurysm With the Sandwich Technique: A Case Report. Vasc Endovascular Surg. 55: 86-90.
- Xiong J, Hu Z, Zhang H, Xu H, Chen D, et al. (2017) Successful use of retrograde branched extension limb assembling technique in endovascular repair of pararenal abdominal aortic aneurysm. J Vasc Surg Cases Innov Tech 3: 90-94.
- Gibello L, Frola E, Ripepi M, Ruffino MA, Varetto G, et al. (2021) Physician-modified fenestrated Navion endograft for the treatment of a symptomatic postdissection thoracoabdominal aneurysm. J Vasc Surg Cases Innov Tech 7: 344-349.
- Jennings J, Sheahan LD, Gloss CC, Vogel TR, Bath J (2021) Multiple Chimney Endografts (ChEVAR) for Ruptured Pararenal Aortic Aneurysm. Ann Vasc Surg.
- Yammine H, Briggs CS, Stanley GA, Ballast JK, Arko Iii FR (2018) Advanced Techniques for Treating Juxtarenal and Pararenal Abdominal Aortic Aneurysms: Chimneys, Periscopes, Sandwiches and Other Methods. Tech Vasc Interv Radiol 21: 165-174.
Citation: Prasertcharoensuk S, Wongkonkitsin N, Tunmit P, Angkasith P, Teeratakulpisarn P, et al. (2021) Sandwich EVAR is Salvageable Technique in Juxtarenal AAA. J Angiol Vasc Surg 6: 073.
Copyright: © 2021 Supatcha Prasertcharoensuk, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.