Small Bowel Obstruction Secondary to an Internal Hernia after a Robotic Sacrocolpopexy with Mesh
*Corresponding Author(s):
James ChambersDepartment Of Surgery, Northeast Georgia Heath System, Braselton, GA, United States
Email:jchamb7389@aol.com
Abstract
Background: Small bowel obstruction has been noted to occur in anywhere from 1-10% of patients with a history of abdominal surgery, and in 4.7% of patients after robotic surgery, all of these studies have focused mainly on adhesions being the source of obstruction. Internal hernia is a much less common cause for small bowel obstruction post robotic sacrocolpopexy.
Case: Herein is presented a case of a 69 year old female with a small bowel obstruction caused by an internal hernia as a result of the space between the sacral promontory and the elevated cervix sacrocolpopexy. Operative findings were consistent with the peritoneum not remaining closed between these two structures after the absorbable suture had dissolved.
Conclusion: When a patient has a small bowel obstruction post sacrocolpopexy close attention should be paid to the potential that the patient may have an internal hernia causing such a process and the general surgery service should be involved in the patients care soon after presentation.
Introduction
While small bowel obstruction occurs anywhere from 1-10% after open abdominal surgery [1], a recent study shows that its frequency during robotic surgery is only about 4.7% [2]. Internal hernias are most often associated with gastric bypass surgery and account for 27.9% of post gastric bypass bowel obstruction [3]. They are however, relatively uncommon after pelvic and GYN surgery. Review of the literature shows that small bowel obstruction and port site hernia post sacrocolpopexy is uncommon as well at 0.7% and 0.4% respectively [4]. Few studies exist that describe an internal hernia after such operation [5]. This case describes the scenario of an internal hernia as a result of an internal hernia between the sacral promontory and the elevated cervix. It is purported that the cause of this was failure of the peritoneal closure to stay intact after the absorbable suture had dissolved.
Case
A 69-year-old female with a history of uterine prolapse and failed pessary underwent a robotic assisted supracervical hysterectomy with bilateral salipingo ophorectomy and sacrocolpopexy with mesh in September 2019. Boston Scientific Y mesh was utlized and 0 V lock sutures were used to cover the mesh. Her family medical history was significant for a brother and son with Marfan’s syndrome. She has an uneventful postoperative course until approximately November 2019. At this time she was admitted through the Emergency Room to the GYN service with a bowel obstruction, her symptoms abated after 24 hours of NG decompression and she was discharged. On this admission she had and episode of SVT which prompted a cardiac evaluation. Less than 24 hours after discharge, she presented back to the ED with worsening symptoms. General Surgery was consulted and initial management of the bowel obstruction with nasogastric tube decompression, intravenous fluids and bowel rest were initiated. The patients CT was worrisome for a small bowel obstruction with a transition point in the pelvis and had worsening distention from CT on the prior admission. The patient was counseled on management of the small bowel obstruction and potential need for surgical intervention, given the rapid return of her adverse symptoms. On hospital day number one the patient had a bowel movement, but her NG output remained high, and remained distended. The decision was made to explore that patient on hospital day number 3, after a small bowel follow through showed a persistent obstruction. A diagnostic laparoscopy converted to laparotomy demonstrated that a portion of her small bowel was entrapped though an internal hernia created between elevated cervix and vagina and the sacral promontory, as the peritoneal flap had not closed, the V lock suture that had been used to close this space had absorbed. The small bowel was reduced from this space and a small bowel resection with anastomosis was required as the small bowel was ischemic from a closed loop obstruction. The potential space between the sacral promontory and the elevated cervix and vagina was closed with 2-0 silk sutures. The patient had a postoperative ileus and was discharge on post op day nine and has been doing well in the interim (Figure 1).
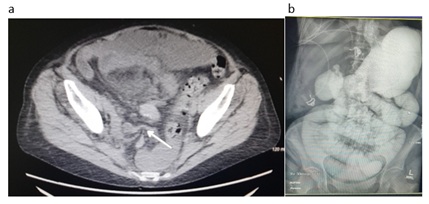 Figure 1: CT on readmission showing transition point (denoted by arrow) in pelvis that would later prove to be the internal hernia (a). Image from small bowel follow through showing persistent obstruction (b).
Figure 1: CT on readmission showing transition point (denoted by arrow) in pelvis that would later prove to be the internal hernia (a). Image from small bowel follow through showing persistent obstruction (b).
Discussion
This case demonstrates a rarely reported source for an internal hernia causing a small bowel obstruction [5]. Review of the literature showed a very low incidence of small bowel obstruction related complications after a robotic sacrocolpopexy [5,6]. Few mesh complications were also observed as well [7]. There are a growing number of papers in the literature that describe small bowel obstructions caused by the V lock suture [8]. It was our original suspicion that the V lock suture may have contributed to the obstruction. Now the suspicion is that the absorbable V lock suture did not allow for the peritoneum to have enough time to scar down over the mesh in this patient that likely has some degree of connective tissue disfunction given her son and father having Marfan’s syndrome. This case highlights the importance of consideration of patient factors in selection of what type of suture is used for a given purpose. It also highlights the need for prompt consultation of the General Surgery service when a small bowel obstruction is suspected.
References
- Sakari T, Chrristersson M, Karlbom U (2020) Mechanisms of adhesive small bowel obstruction and outome of surgery; a population based study BMC Surg 20: 62.
- Banapour P, Yuh B, Cheenam A, Shen JK, Ruel N, et al. (2020) Readmission and complications after robotic surgery: Experience of 10,000 opeerations at a comprehensive cancer center. J Robot Surg 15: 37-44.
- Bower KL, Lollar DI, William SL, Adkins FC, Luyimbazi DT, et al. (2018) Small Bowel Obstruction. Surg Clin North Am 98: 945-971.
- Hudson CO, Northington, GM, Lyles RH, Karp DR (2014) Outcomes of robotic sacrocolpopexy: A systemic review and meta-analysis. Female Pelvic Med Reconstr Surg 20: 252-260.
- Halwani Y, Nicolau-Tolouse V, Oakes J, Leipsic J, Geoffrion R, et al. (2013) Transvaginal strangulated small intestinal hernia after abdominal sacrocolpopexy: Case report and literature review. Hernia 17: 279-283.
- Gavlin A, Kierans AS, Chen J, Song C, Guniganti P, et al. (2020) Imaging and treatment of complications of abdominal and pelvic mesh repair. Radiographics 40: 432-453.
- Anand M, Woelk JL, Weaver AL, Trabuco EC, Klingele CJ, et al. (2014) Perioperative complications of robotic sacrrocolpopexy for post-hysterectomy vaginal vault prolapse. Int Urogynecol J 25: 1193-1200.
- Zipple MK, Bankhead-Kendall B, Roy MD, Yaldo B (2020) Small bowel obstruction secondary to barbed suture after minimally invasive inguinal hernia repair. AmSurgeon 86: 14-16.
Citation: Chambers J (2021) Small Bowel Obstruction Secondary to an Internal Hernia after a Robotic Sacrocolpopexy with Mesh. Archiv Surg S Educ 3: 029.
Copyright: © 2021 James Chambers, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.