Spontaneous Congenital Ping-Pong Fracture
*Corresponding Author(s):
Inês GanhãoDepartment Of Pediatrics, Centro Hospitalar Barreiro Montijo, Avenida Movimento Das Forças Armadas, Portugal
Tel:+351 212147300,
Email:inesieganhao@gmail.com
Abstract
Congenital ping-pong fractures are rare, occurring in 1 to 2.5 cases per 10000 live births. They are frequently associated with forceps application, but at times, there isn’t an identifiable traumatic episode, being therefore named “spontaneous”. Its etiology has not been fully elucidated and associated intracranial injuries are uncommon.
This is a case report describing the finding of a depressed skull fracture in a neonate with a non-instrumented delivery, no history of trauma during pregnancy and an unremarkable neurological examination at birth. Skull x-ray showed a parietal depression and head computed tomography performed afterwards confirmed a ping-pong fracture deforming the underlying brain parenchyma and excluded associated intracranial injuries. There was a complete resolution of these findings 6 months after, with an expectant attitude.
Although unsettling to the parents, spontaneous congenital ping-pong fractures are usually benign, resolving spontaneously within 6 months and can often be managed in a conservative way.
Keywords
Congenital; Newborn; Ping-pong fracture; Spontaneous
INTRODUCTION
Ping-pong fractures consist of depressed skull deformities, similar to a dent in a ping-pong ball - with no fracture line radiologically identified [1,2]. Typically occurs in newborns and infants when the skull bones are still soft, thin and resilient and therefore, able to indent without break. They are classified as a green stick fracture. Congenital ping-pong fractures occur with an estimated incidence of 1 to 2.5 cases per 10000 live births [3,4]. Usually result from head injury during complicated deliveries (With instrumental or obstetrical maneuvers, such as forceps application) or from maternal abdominal trauma during pregnancy [5,6]. In rare cases, there isn’t an identifiable traumatic episode, occurring in newborns after an uneventful pregnancy and non-traumatic delivery, and therefore named “spontaneous” [5]. Its etiology had not been fully elucidated yet. It is thought that may result from a continuous intrauterine pressure upon the soft fetal skull caused by bony structures (Such as the fifth lumbar vertebrae, sacral promontory, pubic symphysis, ischial bone), or by an asymmetric or contracted pelvis, a uterine myoma or even by fetal extremities. Mainly, these factors are unpredictable and not related to demographic or obstetric characteristics [1,5-7].
CASE REPORT
We report the case of a female newborn, born at full-term by eutocic delivery (Cephalic presentation) after an uneventful pregnancy of a healthy 33-year-old woman. Apgar score was of 9/10 at 1 and 5 minutes, respectively. Birth weight was 2625 g (Appropriate for gestational age) and head circumference 32 cm (3rd-15th percentile). Physical examination revealed a depression on right parietal region measuring approximately 3 x 2 cm, depth of 2 cm, without skin lesions and unremarkable neurological examination. Skull radiography showed an abnormal concavity in the parietal bone (Figure 1). Head Computed Tomography (CT) scan, performed afterwards, confirmed a ping-pong fracture deforming the underlying brain parenchyma and excluded any associated intracranial injuries (Figures 2 & 3). The newborn remained clinically stable, without signs of intracranial hypertension. After discussion with neurosurgery, an expectant attitude was decided. At 6-month-old there was a complete resolution of the deformity of the skull and she had an adequate neurodevelopment and physical growth.
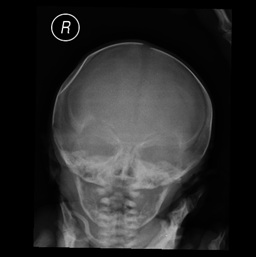 Figure 1: Skull x-ray showing a right-sided ping-pong fracture of the parietal bone.
Figure 1: Skull x-ray showing a right-sided ping-pong fracture of the parietal bone.
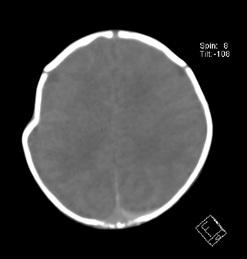 Figure 2: Head Computed Tomography (CT) scan, in the axial plane, showing the absence of intracranial injuries associated with the fracture.
Figure 2: Head Computed Tomography (CT) scan, in the axial plane, showing the absence of intracranial injuries associated with the fracture.
 Figure 3: Head CT scan in three-dimensional volume view showing the depressed deformity of right parietal bone.
Figure 3: Head CT scan in three-dimensional volume view showing the depressed deformity of right parietal bone.
DISCUSSION
Detailed birth history and postnatal examination for evidence of acute injury are crucial in differentiating between both etiologies of these fractures - “spontaneous” or ‘instrument associated’ - since radiological imaging provides limited information [7]. In this case, it is very likely that the skull fracture was congenital as there was no instrumentation use in labour. The diagnosis is clinical and affected newborns/infants are asymptomatic, unless there is intracranial injury associated [1]. Intracranial lesions are significantly more likely to occur when these fractures follows an instrumental delivery. Prognosis is good in spontaneous cases, as they’re rarely associated with intracranial injuries [5-8]. Skull radiography shows the degree of deformation and cranial ultrasound can identify intracranial hemorrhages or hematomas. Although CT scan is more sensitive, it should only be performed if there is any doubt regarding the diagnostic or suspicion of any complications [5,8]. Management is not standardized, ranging from neurosurgical correction to conservative treatment - watchful waiting. Non-surgical reduction is an option, using digital pressure or vacuum extractor. The choice is based on extension of the fracture and underlying brain injury [1-3,5,8,9]. If the lesion is small, it is likely to occur spontaneous resolution within months. On the other hand, large lesions (> 3 cm) with mass effect leading to midline deviation need surgical correction surgery. In addition, it is advisable to elevate severe depressions to prevent sustained pressure-induced cortical injuries [1,4,7,9]. Although these deformities are a source of great distress to the newborn’s family, they are usually benign and can be treated conservatively, with most of these fractures resolving spontaneously within 6 months [4].
DISCLOSURE
This case was presented in 2016, as poster presentation on 8th Excellence in Pediatrics Conference (Same case, different title).
FUNDING SOURCE
No external funding was obtained.
FINANCIAL DISCLOSURE
The authors have no financial relationships relevant to this article to disclose.
CONFLICT OF INTEREST
The authors have no conflicts of interest to disclose.
REFERENCES
- Lunt CMB, Roth K, Eich G, Pasquier S, Zeilinger G (2006) Neonatal ping pong fracture. Swiss Society of Neonatology, Switzerland. Pg no: 1-12.
- Z Zia, A-M Morris, R Paw (2007) Ping-pong fracture. Emerg Med J 24: 731.
- Amaral ME, Grilo E, Mimoso G (2015) Fratura em ping-pong. Acta Pediatr Port 46: 152-153.
- Basaldella L, Marton E, Bekelis K, Longatti P (2011) Spontaneous resolution of atraumatic intrauterine ping-pong fractures in newborns delivered by cesarean section. J Child Neurol 26: 1449-1451.
- Fantacci C, Massimi L, Capozzi D, Romano V, Ferrara P, et al. (2015) “Spontaneous” ping-pong fracture in newborns: case report and review of the literature. Signa Vitae 10: 103-109.
- Dupuis O, Silveira R, Dupont C, Mottolese C, Kahn P, et al. (2005) Comparison of “instrument-associated” and “spontaneous” obstetric depressed skull fractures in a cohort of 68 neonates. Am J Obstet Gynecol 192: 165-170.
- Brittain C, Muthukumar P, Job S, Sank S (2012) ‘Ping pong’ fracture in a term infant. BMJ Case 2012: 0120125631.
- Silva JB, João A, Miranda N (2019) Ping-pong fracture in newborn: A rare diagnosis. Acta Med Port 32: 549.
- Loire M, Barat M, Mangyanda Kinkembo L, Lenhardt F, M’buila C (2017) Spontaneous ping-pong parietal fracture in a newborn. Arch Dis Child Fetal Neonatal Ed 102: 160-161.
Citation: Ganhão I, Matias M, Parreira RM, Bretes I (2019) Spontaneous Congenital Ping-Pong Fracture. J Neonatol Clin Pediatr 6: 040.
Copyright: © 2019 Inês Ganhão, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.