The Perspective of Whole Body Cryotherapy in Rheumatic Diseases: A Narrative Review
*Corresponding Author(s):
Perrotta Adolfo MarcoDepartment Of Translational And Precision Medicine, University Of Rome 'La Sapienza', Rome, Italy
Email:adolfo.perrotta@gmail.com
Abstract
Objective: Whole Body Cryotherapy (WBC) consists in using cold application as a form of physical therapy to reduce pain and inflammation levels.
Data source: This narrative review reports data from trials studying the role of WBC in treating rheumatologic diseases such as Rheumatoid Arthritis (RA), Fibromyalgia (FM), Ankylosing Spondylitis (AS) and Chronic Pain. The systematic literature research was conducted on the past ten years. The main search keywords were “whole body”, “cryotherapy”, “cabin”, “Rheumatoid Arthritis”, “Ankylosing Spondylitis”, “Fibromyalgia”, “Psoriatic Arthritis”, “Chronic Fatigue”, “Rheumatic disorder”, “Rheumatic disease”.
Data selection and data Extraction: The sample size, subject’s age and gender, year of publication, duration and temperature of exposition, physical activity and outcomes were extracted. Of all the articles examined, only 17 met the inclusion criteria.
Data synthesis: Data regarding 816 subjects aged between 17 to 80 were included in the review. The WBC protocols covered temperatures from -10 to -196 degrees Celsius, while exposure times ranged from 30 seconds to 3 minutes. WBC was usually paired with other kinds of physical therapies, such as Kinesiotherapy and physical exercise. WBC seems to be a safe procedure for all the groups of the population examined, with no major events to report.
Conclusion: WBC could be an “add-on therapy” useful in the management of several Rheumatic diseases, even though numerous aspects need to be clarified, as shown in the research agenda proposed in this review. Hence, further studies are necessary to establish standardized protocols.
Keywords
Whole body; Cryotherapy; Rheumatoid arthritis; Ankylosing spondylitis; Fibromyalgia; Psoriatic arthritis; Chronic fatigue; rheumatic disorder
Introduction
Cryotherapy corresponds to the therapeutic application of cold to control inflammation and relieve pain in sports after traumas, often using cold packs to do so. Cryotherapy is often used as an additional therapy to control the level of inflammation in rheumatic diseases [1,2]. Cold has a positive effect in mitigating pain levels and allows the patients to increase physical activity [3]. Cryotherapy seems to downregulate the levels of pro-inflammatory cytokines [4]. Whole-body cryotherapy (WBC) is a short exposure to extremely cold air in a controlled cabin for time periods ranging from 2 to 5 mins. WBC was born in Japan during the ‘70s. Starting from Germany, it spread throughout Europe ten years later [5]. This technique requires exposure to a very low temperature (from −110°C to −160°C) in a dry environment for a short period of time, usually 1-3 minutes. Some studies demonstrated its efficiency in decreasing articular pain and supporting physical rehabilitation [6,7].
Some data show that WBC is able to reduce inflammation and to produce analgesic effects, therefore it has been explored in inflammatory musculoskeletal disorders such as rheumatoid arthritis and ankylosing spondylitis. It’s been demonstrated that, as well as recovering after any form of heavy exercise, Cryotherapy determines an increase in white blood cells, antiinflammatory cytokines, ACTH, beta-endorphins, cortisol and catecholamines. Moreover, Cryotherapy is believed to cause immunostimulation, by increasing noradrenaline response to cold, reducing pain through the decrease of nerve conduction and increasing the level of plasma total antioxidant cytokines, therefore improving immune function in general. Also, while muscle stress and inflammation increase the level of oxidants in the intercellular space leading to membrane damage and, ultimately, to an increase in inflammation, the cold has been suggested to reduce oxidant production by decreasing the level of inflammation.
In 1986 Yamauchi found that the effects of WBC with temperatures as low as -175°C influences cortisol concentrations and has a direct analgesic effect in RA patients, while Samborski and Sobieska, in a cross over study (which compared the effects of WBC to hot mud pack), showed that WBC with temperatures at -150°C could lead to an increase of the pressure pain threshold, decrease of the number of tenderpoints and pain levels in general in the short-term in patients affected by FM.
In 2000, Offenbächer reviewed treatment options in FM, considering cardiovascular fitness training physiotherapy, massage, acupuncture and trigger point injection , biofeedback, TENS and WBC, which may reduce localized as well as generalized pain in the short term. Even though there is no single best treatment for FM, a multidisciplinary approach combining physical therapy and these other treatment options is thought to be the most promising strategy. Also, in the same review, Offenbächer delved further into the use of WBC in previous research programs and its rationale as a treatment possibility for rheumatoid diseases [8]. In addition, some recent meta-analyses have confirmed the positive influence of cryogenic temperatures on patients with AS [9,10]. The effects of WBC on oxidative stress in healthy people [4,11,12] and AS patients [11,13] is under investigation, especially to establish and standardize treatment protocols [1].
The aim of this narrative review is to report trials and studies regarding the application of WBC in rheumatic diseases such as RA, FM, AS and CF in order to summarize and better understand its limitations and effectiveness in patients affected by rheumatic diseases.
Methods
To conduct the electronic and systematic search, the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) Guidelines were followed and databases such as PubMed, Scopus and ScienceDirect were used. The main search keywords were “whole body”, “cryotherapy”, “cabin”, “Rheumatoid Arthritis”, “Ankylosing Spondylitis”, “Fibromyalgia”, “Psoriatic Arthritis”, “Chronic Fatigue”, “Rheumatic disorder”, “Rheumatic disease”. By doing so, the following data regarding the number and characteristics of participants (sample size, subject’s age, and gender) were obtained, as well as year of publication, description of the intervention (application characteristics, duration and temperature of treatment), level of activity, inclusion criteria, trial groups, outcomes, tools used to evaluate results and study results.
Results from the past ten years were investigated and 17 articles which met the criteria were found, after thorough research conducted by PMS, FM and AM. The search strategy is depicted in Figure 1.
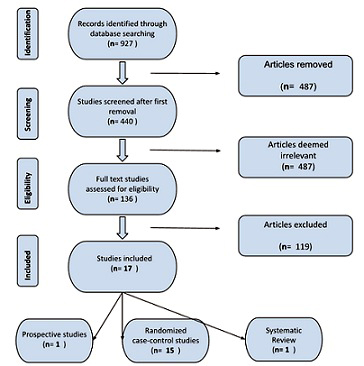 Figure 1: Prisma Flow Chart.
Figure 1: Prisma Flow Chart.
Duplicated and irrelevant articles, wrong outcomes, incorrect patient population, incorrect intervention and topics were all criteria of exclusion.
Results
The results are reported according to the specific disease explored in the study.
Fibromyalgia
Fibromyalgia is a chronic widespread pain disorder in which the neurogenic origin of the pain, featured by allodynia and hyperalgesia, results from an imbalance in the levels of neurotransmitters and, consequently, of the peripheral pro- and anti-inflammatory mediators [13]. In 2018 Javier Rivera evaluated the efficacy of WBC to control pain and symptoms in sixty patients affected by FM in an open, randomized, crossover trial. Patients were divided into two groups: while one of them underwent 15 WBC sessions in 3 weeks (-60°C (30s) plus -140°C (3min)) with a Cryosense TCT cabin, the remaining acted as a control group. This first period of treatment was followed by a 1-week of washout during which the two groups were inverted, and another 3-weeks period of treatment. The Study measured change (Δ) in pain after 2 and 4 weeks, according to a visual analogue scale (VAS), Δ burden of disease, evaluated by the FM Impact Questionnaire (FIQ), and severity of FM, measured by the Combined Index of Severity of FM (ICAF). It showed that outcomes were significantly larger in the WBC group after the first period of treatment. The authors concluded that WBC with a Cryosense TCT cabin may be a useful adjuvant therapy for FM [14]. In the same year, Vitenet randomized 24 patients with FM into 2 groups; 11 patients were treated with 10 sessions of WBC (-110°C) for 3 min, over a duration of 8 days in addition to usual care, while the control group (13 patients) received usual care. Patients in the WBC group reported a significantly improved quality of life compared to the control group, lasting up to a month after the exposure to cold [15]. Furthermore, in 2021 Klemm compared 23 FM patients to 30 healthy subjects (HC) after 6 serial sessions of WBC at − 130°C for 3 min, administered twice a week, evaluating both symptomatic outcomes (such as change in pain level and disease activity) and laboratories findings (like cytokine levels interleukin (IL)-1, IL-6, tumor necrosis factor α (TNFα) and IL-10) after 3 sessions and 3 months after WBC exposition. The patients’ opinions about the satisfaction, effectiveness and relevance of WBC were also reported. Patients treated with WBC showed a significant reduction in pain and disease activity after 3 and 6 sessions, without clinical benefits at 3 months follow up. However, patients in the WBC group reported high levels of satisfaction and considered WBC relevant and valuable. Laboratory findings showed that patients suffering from FM had a significantly different response of IL1, − 6 and − 10 to WBC compared to healthy subjects [16]. Taking all in consideration WBC could be a therapeutic option for FM patients.
Rheumatoid Arthritis (RA)
In 2015, Gizinska compared the effects of WBC on 25 patients, exposed for 10 sessions in 2 weeks to −110° C for 3 min, to 19 patients treated with a traditional rehabilitation program (TR). Systemic levels of IL-6 and TNF-α were evaluated. After therapy all patients exhibited similar improvement in pain levels, disease activity, fatigue and physical activity. The TR group showed significantly better results in HAQ only; similar important reduction in IL-6 and TNF-α levels were detected in both groups [17]. In 2017 H. Hirvonen investigated 60 RA patients, randomized into 3 groups: (1) WBC at −110°C, (2) WBC at −60°C, or (3) local cryotherapy. Each session was administered three times/day for 7 consecutive days and was combined with conventional rehabilitation. RA disease activity, daily plasma samples and total peroxyl radical trapping antioxidant capacity of plasma (TRAP) were evaluated before the first and after the last session. The authors report that only WBC at −110 °C induced a short-term increase in TRAP during the first treatment session and that the effects were short, being unable to maintain a significant improvement in oxidative stress or adaptation along 1 week [18]. Moreover, in 2019 Sadura compared the effects of WBC (administered for 20 days once a day at-140°C for 3 min) and conventional rehabilitation (CR) in 50 RA patients divided into a study group (CT, n = 25) and a control group (CR, n = 25). The disease activity score (DAS28), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels, serum concentrations of IL-6, TNF-α, macrophage migration inhibitory factor [MIF]) and IL-10 cytokines were measured. No statistically significant differences were observed between the two groups DAS28, morning stiffness and pain, as well as in the serum concentrations of tested cytokines after rehabilitation, nor between patient groups. Statistically significant improvements in CRP serum level were reported only in the CT group [19]. Finally, Klemm recently evaluated 56 patients affected by active RA undergoing a 16-day multimodal rheumatologic complex treatment randomized to either WBC (6 applications in 14 days at -130°C for 3 min) or no treatment. Significative differences between the two groups regarding pain, disease activity, functional capacity, cytokine levels, and consumption of analgesics were assessed. After 12 weeks, the modification in pain scale remained significant, despite the disease activity score and functional capacity, which were still meaningful but not statistically significant [20].
Ankylosing spondylitis
In 2015, Stanek investigated the capacity of WBC sessions to produce beneficial effects on index of AS disease Activity Index (BASDAI) and BASFI, pain intensity and spine mobility parameters in AS patients, after a WBC session (at -120°C) lasting 3 minutes a day with a subsequent 60 minutes of kinesiotherapy, compared with 60 minutes of kinesiotherapy only for 10 consecutive days. The authors reported that the WBC group with subsequent kinesiotherapy showed an average of about twice better results compared to the group treated only with kinesiotherapy [21].
In a study conducted in 2018 by Anna Straburzynska-Lupa, sixty-five patients affected by AS were randomized to one of these three arms : WBC at −110° C, −60°C (for 3 min each session, once a day per 8 days), or exercise therapy (non-WBC). The Bath BASDAI, AS Disease Activity Score (ASDAS-CRP), concentration of C-RP, and the concentrations of IL-8, IL-17, also the concentration of thiobarbituric acid reactive substances (TBARS) were assessed to determine the effect of WBC on oxidative stress. BASDAI, ASDAS-CRP, and the IL-8 concentration decreased in all the studied patients. At the end of the treatment the TBARS concentration was significantly increased in the group treated with WBC at −110°C. After therapy BASDAI resulted significantly lower in the WBC at −110° C group compared to the non-WBC group [22]. Moreover, Romanowski compared the effects of 3 regimens of treatment (WBC at-110°C for 3 min combined with exercise, WBC at -60°C for 3 min combined with exercise and exercise therapy alone) on disease activity and the functional parameters at the end of the 8-day treatment of the 92 patients with AS. All patients showed a significant reduction in disease activity, back pain, fatigue, duration and intensity of morning stiffness and a significant improvement in the patient’s functional capacity, spine mobility and chest expandability, with no changes in the levels of CRP. The group that underwent cryotherapy at -110°C manifested a significantly reduced BASDAI compared to exercise therapy only (p = 0.024) [23]. In 2018, Stanek estimated the impact of WBC (at -120°C) lasting 3 minutes a day with a subsequent 60-minute session of kinesiotherapy on oxidative stress in 16 patients affected by active AS, compared to a session of kinesiotherapy alone. The parameters of oxidative stress (antioxidant enzymatic and nonenzymatic antioxidant status, lipid peroxidation products, total oxidative status (TOS), and oxidative stress index (OSI)) as well as BASDAI and BASFI indexes were calculated at baseline and one day after the sessions. In the WBC group, a significant decrease of oxidative stress markers (TOS and OSI) and a significant increase of total antioxidant status were detected. Also the BASDAI and BASFI indexes decreased significantly in both groups, but the differences between before and after treatment were significantly higher in the WBC group than in the control one [24]. Stanek also investigated the impact of WBC on cardiovascular risk factors in male patients with AS, by evaluating disease activity, markers of inflammation, oxidative stress, lipid profile, and atherosclerosis plaque after WBC sessions (administered at -120°C for 3 min a day) with subsequent kinesiotherapy, or kinesiotherapy alone. In both groups, a decrease of the total cholesterol and LDL cholesterol, triglycerides, sCD40L, PAPP-A, and PLGF levels were observed, but the difference was higher in the WBC group. Similar results were found considering the BASDAI and BASFI indexes [10].
Chronic fatigue
Bettoni, in 2013, evaluated a total of 100 fibromyalgic patients: 50 subjects underwent cryotherapy, and 50 did not. Patients treated with WBC (15 sessions in 3 weeks, -60°C (30s) plus -140 C° (3min))showed a higher improvement of the quality of life measured by Visual Analogue Scale, Short Form-36, Global Health Status and Fatigue Severity Scale, in comparison with the patients of the control group [14]. Also, in 2021 Kujavsky compared the functional interrelation of fatigue and cognitive, cardiovascular and autonomic nervous systems implications in a group of 32 patients affected by CFS with 18 healthy controls. The patients were treated with WBC (-120°C) combined with a static-stretching (SS) program with 5 sessions per week, for 2 weeks. In the CFS group an increased fatigue was found, related to baroreceptor function. After ten sessions of WBC with a static stretching exercise, both groups showed an improvement regarding fatigue, cognitive function, cardiovascular and autonomic nervous systems [25]. Recently, the same author investigated the tolerability and effects of SS and WBC on fatigue, daytime sleepiness, cognitive functioning and autonomic nervous system functioning in 32 patients suffering from CFS compared to a control group (18 healthy subjects). All patients underwent a programme of five sessions per week for 2 weeks, composed by SS associated with WBC. A significant decrease in fatigue was reported in the CFS group. Moreover, some parameters of cognitive functioning, such as speed of processing visual information and set-shifting, also improved in both groups [26].
Discussion
Rheumatic diseases are systemic disorders, affecting the organism as a whole, thus needing systemic therapy. In addition physical exercise is undoubtedly fundamental to produce beneficial effects on pain in these diseases [27], but it’s not sufficient alone. For instance, low intensity exercise is the main therapy applied in rheumatic patients [28], but adjuvant therapies for muscular soreness are needed as well, such as cold therapy. Therefore, using WBC in addition to medications and physical therapy, could lead to a significant improvement in the patient’s general well-being and quality of life and, at the same time, to a decrease of systemic collateral effects by reducing drug dosage. Data here indicates the importance of employing a combined therapeutic approach [27] of WBC to reduce pain in Rheumatic diseases when associated with physical activity. This combination seems to lead to adjunctive beneficial results, such as improvement in mood, promotion of a better pain adjustment and facilitation of physical and mental activities [18,19,24,27,29,30]. It is also suggested that this therapeutic association could improve the management of patients affected by AR, ameliorating the aerobic capacity and reducing their cardiovascular risk [31]. Different pathways and mechanisms of action have been investigated to explain WBC’s positive effects on patients. Firstly, WBC is capable of significantly reducing oxidative stress and inflammation levels in the organism. This is the reason why it has been suggested for clinical use in all Rheumatic diseases [32]. Furthermore, WBC is able to regulate neurotransmission involved in pain perception, and also to balance pro- and anti- inflammatory cytokine levels in the body. Moreover, WBC has been used with a positive effect on other systemic diseases such as Atherosclerosis and dyslipidemia, proving itself to be a useful method of prevention [10].
WBC’s positive effects on cardiovascular and autonomic functions have been shown by Kujavsky as well: his recent studies confirm that WBC is well tolerated by patients affected with CFS and leads to symptomatic improvements associated with cardiovascular health. Hence, given the preliminary data showing the beneficial effect of cryotherapy, its relatively easy application, good tolerability, and proven safety, it appears to be an approach worthy of attention [26].
Moreover, as shown by Guillot by pooling 6 studies including 257 RA patients, a significant decrease activity score after chronic cryotherapy was assessed. Also, local cryotherapy was demonstrated to induce intra-joint temperature decrease, thus down regulating mediators involved in inflammation and joint damage, such as cytokines, proangiogenic factors and cartilage-degrading enzymes [1].
WBC is also to be considered a safe therapy option (using temperatures spanning from -130°C to -60°C), as demonstrated by the lack of side effects in the rheumatic patients enrolled in the studies taken into account in this paper. Similar results about safety have been found in healthy subjects and athletes as well as obese and/or old patients [33-36]. WBC seems also to have positive effects in the rheological parameters of blood in older women showing a significant decrease in erythrocyte elasticity and aggregation indices [35]. In particular, Kujawsky reported that in older subjects (aged > 55) with Mild Cognitive Impairment (MCI), WBC treatment determined a significant improvement of short-term memory, such as a reduction in IL-6 levels and an increase in BDNF release when whole blood was challenged with Aβ42 (Amyloid β-42) [36]. Considering all together we can argue that WBC can enhance performance and alleviate chronic conditions in older patients, combined with regular physical exercise. It could also represent a potential affordable treatment in conditions associated with cognitive dysfunction [25,26]. WBC could be proposed for clinical use in RA and other joint inflammatory diseases as an additional therapy to conventional or biological disease-modifying antirheumatic drugs (DMARDs), as well to corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs) in order to decrease the dosage of systemic pharmacological treatments, minimizing the likely of severe related side effects [1].
Even if studies on cryotherapy were not numerous, the evidence suggesting the benefits on pain relief and disease activity is increasing. These results, however, need to be confirmed, because pain relief can be due to several factors and pain level is probably not the most specific parameter to evaluate the efficacy in the management of disease. In addition the duration of clinical benefit seems to be short. Unfortunately, the lack of literature concerning WBC and its protocols leads to questions about the intensity (temperature wise) and duration of the treatment, repetition of sessions or the most suitable time to perform WBC in addition to physical therapy. Finally, additional research is required to define the best moment to start WBC regarding the course and stage of the target disease. All these unanswered questions are reported in the Research Agenda. However, the impact and contribution of WBC to medical and physical therapy appears to be promising, but not yet completely defined [37,38], as it is equally not fully determined the comparison between the effects of systemic and local cryotherapy [37,39], because of the lack of studies comparing the effectiveness of WBC among other crio-therapies (Table 1).
|
Research agenda |
|
Standardization of protocols related to each specific disease is required |
|
Personalization of protocols according to subject characteristics is necessary |
|
Duration of exposure, range of temperature during exposure, frequency and number of sessions have to defined |
|
Determination of the appropriate timing of exposure in relation to physical therapy has to be determined |
|
Determination of the appropriate timing of exposure in relation to the stage of disease needs to be investigated |
|
Determination of the protocol based on disease’s activity/inactivity is necessary |
|
The gender difference in safety and clinical efficacy must be attentively reported |
Table 1: Research Agenda.
To discern between PBC and WBC, it is helpful to refer to a study conducted by Bouzigon in 2016. In PBC treatment, the head region is excluded and a more moderate-sized mobile device is used than in WBC. The study also demonstrates that PBC is the preferred treatment in the sport recovery domain, since it can be easily performed in the field, or wherever needed, whereas WBC requires cabins and more stable and stationary equipment. This is the reason why WBC is more widespread in a rehabilitation context. Furthermore, WBC is a convenient option when more patients need to be treated at the same time. Of course there are limitations that seem to stand for both treatments: while PBC seems to be the least safe option (since direct contact with nitrogen is needed for the procedure), it is easier to exit a PBC cabin. Another limitation applies to energy consumption, which is high for both treatments, although it seems that PBC is the most economical one in terms of purchase. However, large quantities of nitrogen (which is expensive and hard to supply) is needed to perform PBC, while it is not used in WBC. Lastly, PBC exposes the user to temperature heterogeneity during the treatment, while there is not sufficient data about WBC cabins’ temperature [2] (Table 2).
|
Author |
Article |
Pathology |
Diagnostic criteria |
N. patients |
Inclusion Criteria |
Exclusion Criteria |
Temperature/time (WBC group) |
Temperature/time (control group) |
Outcome |
Results |
Adverse events/Results |
||||
|
1 |
J.Rivera (2018) |
RCT |
FM |
ACR |
60 |
25-80yo FM for more than 1 year Reduced or no response to therapies Not pregnant |
Cardiovascular or psychiatric comorbidity Cold intolerance |
10 sessions in 3 weeks |
Primary endpoint: changes in VAS and in FIQ. Secondary endpoint: changes in the severity of the disease (assessed by ICAF). |
Improvement of: VAS, FIQ and ICAF |
Tremors, stiffness, headache, vomiting, palpitations, sleep disturbances (8%) |
||||
|
2 |
P.Klemm (2021) |
Prospective Control Study |
FM |
2010/11 |
53 (23 FM and 30 HC) |
18 – 80yo FM |
Pregnant Change of drug therapy in the last 4 weeks |
6 sessions in 3 weeks |
No treatment |
Primary endpoint: changes in VAS after 6 sessions. Secondary outcome: changes in VAS after 3 sessions of WBC and 3 months of discontinued therapy and in cytokine levels (IL-1, IL-6, TNF-a and IL-10) |
Subjective satisfaction of WBC group. |
Nausea (1%), Erythema (1%) |
|||
|
3 |
T. Sadura-Kieklucka (2019) |
RCT |
RA |
EULAR |
50 (25 each group) |
18-59yo Same therapy for at least 3 months. |
Surgery within the last 6 months, prior cancer. |
1 session daily for 20 days; 1 WBC session (for 3min at -140 C° for 20 days) + FKT + 30min of physical exercise |
1 FKT session+ 30min of water exercise |
Primary endpoint: changes in DAS28, changes in VAS and ESR. |
Improved in both groups: DAS28, VAS. |
None observed |
|||
|
4 |
Peres (2017) |
Systematic Review |
RA |
683 |
WBC + local crioT + physical activity |
Primary endpoint: evaluation of disease activity and pain relief. |
Improvement of: VAS, |
||||||||
|
5 |
M. Gizinska (2015) |
RCT |
RA |
ACR |
44 (25 and 19) |
Post menopausal women |
10 sessions in 2 week (-10 C°) + (-60 C°) + (-110 C°) for 3min |
Traditional rehabilitation program with other physical agents (i.e. magnetotherapy) |
Primary endpoint: changes in DAS28, changes in VAS, physical function (measured by HAQ-DI) and 50-meter walking test |
Improvement in both groups: disease status, functional performance, VAS, DAS28, TNF-a, IL-6. Decrease in: pain, fatigue, IL-6 and TNF. |
None observed |
||||
|
6 |
H.Hirvonen (2017) |
RCT |
RA |
Active AR |
60 (20, 20 and 20) |
Active seropositive AR |
Hypertension Arhythmia Cardiovascular disease Pulmonary disease Raynaud's disease Cold allergy Cold bronchospasm |
20 sessions in a week First study group: sessions at -110 C°; Second study group: sessions at -60 C° |
20 sessions in a week; local cryotherapy |
Primary endpoint: changes in TRAP |
Only WBC at -110° produced an increase in TRAP |
Intolerance and side effects (15% in both study groups) |
|||
|
7 |
S. Kujavsky (2021) |
RCT |
CF |
Fukuda criteria |
50 (32 CF+ 18 HC) |
Psychiatric disorders CF secondary to other causes |
10 sessions every 2 weeks |
10 sessions every 2 weeks |
Primary endpoint: reduction of fatigue severity (measured by CFQ, FSS and FIS). |
Improvement of: CFQ, FSS, FIS |
None observed |
||||
|
8 |
M.Romanowsky (2020) |
RCT |
AS |
Modified New York criteria |
92 (32, 31 and 29) |
18-65yo; stable pharmacotherapy (2wks for CC and NSAIDs, 12wks for DMARDS) |
Presence of other chronic pathologies and contraindications to WBC |
6 sessions in a week. First study group: sessions at -110 C Second study group: sessions at -60 C°. Each session followed by |
6 sessions in a week. Physical therapy only. |
Primary endpoint: changes in BASDAI, ASDAS-CRP. Secondary outcomes: functional parameters (measured by BASFI and BASMI) |
No difference between groups in: BASFI, BASMI, PCR. |
Respiratory infection (3%) |
|||
|
9 |
A. Straburzy?ska (2018) |
RCT |
AS |
Modified New York criteria |
65 (23, 21 and 21) |
BASDAI>4 Stable pharmacotherapy (2wks for CC and NSAIDs, 12wks for DMARDS) |
Contraindications to WBC |
6 sessions in a week. First study group: sessions at -110 C°: Second study group: sessions at -60 C°. Each session followed by 30min of physical exercise |
6 sessions in a week. Physical therapy only. |
Primary endpoint: changes in BASDAI, ASDAS-CRP, IL-8 and IL-17 levels, total antioxidant capacity measurement. |
Improvement in (all): BASDAI, ASDAS-CRP, IL-8, |
None observed |
|||
|
10 |
C.Garcia (2021) |
CP |
Pain >3months |
||||||||||||
|
11 |
M.Vitenet (2018) |
RCT |
FM |
ACR |
24 (11 and 13) |
18 years or older |
Modification of usual treatments during the experimentationRecent history of WBC treatment Diagnosis of coexisting diseases Potential contraindications for WBC procedures |
10 sessions in 8 days; -110 C° for 3 min |
No treatment |
Primary endpoint: changes in pain and/or inflammatory processes, quality of life and perceived health |
Improvement: health-reported quality of life |
None observed |
|||
|
12 |
Klemm (2022) |
RCT |
RA |
EULAR |
56 (31 and 25) |
18 years or older |
Body weight over 120 kg Intolerance to cold Change |
6 sessions in 14 days; -130°C for 3 min |
No treatment |
Primary endpoint: changes in pain on an NRS, in DAS28, functional capacity (measured by HAQ), serum levels of IL-6, IL-10 and use of analgesics. |
Improvement in: pain level, DAS28, functional capacity and disability, Reductionin : cytokine levels and use of analgesics |
None observed |
|||
|
13 |
Stanek (2015) |
RCT |
AS |
New York Criteria for AS |
48 (32 and 16) |
No associated pathologiesNo treatment with DMARDs, biologic agents, or steroids. |
1 session/day for 3 minutes, with a subsequent 60 minutes of kinesiotherapy |
1 session/day for 10 days. 60-minute session of kinesiotherapy only |
Primary endpoint: evaluation of BASDAI and BASFI Secondary endpoint: changes in pain intensity and chosen spine mobility parameters. |
Reduction in: BASDAI, BASFI in the study group |
None observed |
||||
|
14 |
Stanek (2018) |
RCT |
AS |
Modified New York Criteria |
32 (16 each group) |
No associated pathologiesNo treatment with DMARDs, biologic agents, or steroids |
1 session/day for 10 days. 3 minutes a day with a subsequent 60-minute session of kinesiotherapy |
1 session/day for 10 days. 60-minute session of kinesiotherapy only |
Primary endpoint: evaluation of BASDAI and BASFI Secondary endpoint: changes in oxidative stress parameters |
Improvement in: SOD, total antioxidant activity Reduction: oxidative stress markers; higher reduction of BASFI and BASDAI in study group |
None observed |
||||
|
15 |
Stanek (2018) |
RCT |
AS |
Modified New York Criteria |
32 (16 each group) |
No associated pathologiesNo treatment with DMARDs, biologic agents, or steroids |
1 session/day for 10 days. 3 minutes a day with a subsequent 60-minute session of kinesiotherapy |
1 session/day for 10 days. 60-minute session of kinesiotherapy only |
Primary endpoint: evaluation of BASDAI and BASFI; changes in markers of inflammation (i.e. IL-6), oxidative stress, lipid profile, and atherosclerosis plaque. |
Reductionin: oxidative stress markers, BASDAI and BASFI, total cholesterol and LDL cholesterol, triglycerides. |
None observed |
||||
|
16 |
Bettoni (2012) |
RCT |
CF/FM |
ACR |
100 (50 WBC + 50 no WBC) |
Age range 17-70 years |
15 sessions in 3 weeks; -60° C for 30 sec, then - 140° C for 3 min |
No WBC treatment |
Primary enpoint: evaluation of VAS, of physical and SF-36, of health status, of FSS |
Improvement: quality of life |
None observed |
||||
|
17 |
S.Kujavsky (2022) |
RCT |
CF |
Fukuda criteria |
50 (32 + 18 HC) |
Psychiatric/psychological impairment Fatigue not being the main complaint |
10 sessions in 2 weeks; SS + -110/-160°C |
10 sessions in 2 weeks; SS + -110/-160°C |
Primary endpoint: changes in fatigue, daytime sleepiness, cognitive functioning and autonomic nervous system functioning |
Improvement in: some domains of cognitive functioning (speed of processing visual information and set-shifting). Reductionin: fatigue. |
None observed |
||||
|
Abbreviations |
|
||||||||||||||
|
WBC= |
Whole Body Chriotherapy |
ICAF= |
Combined Index of Severity of Fibromyalgia |
||||||||||||
|
RCT= Randomized Control Trial |
Randomized Control Trial |
HAQ-DI= |
Health Assessment Questionnaire |
||||||||||||
|
FM= |
Fibromyalgia |
TRAP= |
Total peroxyl radical trapping antioxidant capacity of plasma |
||||||||||||
|
RA= |
Rheumatoid Arthritis |
CFQ= |
Chalder Fatigue Scale |
||||||||||||
|
AS= |
Ankilosing Spondylitis |
FSS= |
Fatigue Severity Scale |
||||||||||||
|
CF= |
Chronic Fatigue |
FIS= |
Fatigue Impact Scale |
||||||||||||
|
CP= |
Chronic Pain |
ASDAS= |
AS Disease Activity Score |
||||||||||||
|
ACR= |
American College of Rheumatology |
BASFI= |
Bath Ankylosing Spondylitis Functional Index |
||||||||||||
|
EULAR= |
European League Against Rheumatism |
BASMI= |
Bath Ankylosing Spondylitis Metrology Index |
||||||||||||
|
SD= |
Standard Deviation |
SF-36= |
Short Form Health Survey 36 |
||||||||||||
|
IQR= |
Interquartile Range |
ESR= |
Erythrocyte Sedimentation Rate |
||||||||||||
|
NSAIDS= |
Non-steroidal anti-inflammatory drugs |
MIF= |
Macrophage migration Inhibitory Factor |
||||||||||||
|
DMARDS= |
Disease modifying antirheumatic drugs |
NRS= |
Numerical Rating Scale |
||||||||||||
|
BASDAI= |
Bath Ankylosing Spondylitis Disease Activity Index |
VAS= |
Visual Analog Scale |
||||||||||||
|
DAS= |
Disease Activity Score |
FIQ= |
Fibromyalgia Impact Questionnaire |
||||||||||||
Table 2: Summaries of WBC studies.
Conclusion
WBC seems to be a safe and promising therapeutic option to add to systemic treatments and physical activity in order to improve quality of life in the management of numerous Rheumatic diseases, such as RA, AS, FM and Chronic Fatigue. Its positive effects on pain, oxidative stress, inflammatory response in the system and overall well-being of patients are encouraging. However many items need to be investigated in detail and further studies are necessary. Standardized protocols are not completely defined, considering the lack of literature on this matter. Hence, further studies are required
Declarations of Interest
None
References
- Guillot X, Tordi N, Mourot L, Demougeot C, Dugué B, et al. (2014) Cryotherapy in inflammatory rheumatic diseases: A systematic review. Expert Rev Clin Immunol 10: 281-294.
- Bouzigon R, Grappe F, Ravier G, Dugue B (2016) Whole- and partial-body cryostimulation/cryotherapy: Current technologies and practical applications. J Therm Biol 61: 67-81.
- Braun KP, Brookman-Amissah S, Geissler K, Ast D, May M, et al. (2009) Whole-Body Cryotherapy in Patients with Inflammatory Rheumatic Disease. A Prospective Study. Med Klin (Munich) 104: 192-196.
- Lubkowska A, Szygula Z, Chlubek D, Banfi G (2011) The effect of prolonged whole-body cryostimulation treatment with different amounts of sessions on chosen pro-and anti-inflammatory cytokines levels in healthy men. Scand J Clin Lab Invest 71: 419-425.
- Braun J, Sieper J (2007) Ankylosing spondylitis. Lancet 369: 1379-1390.
- Smith JA (2015) Update on Ankylosing Spondylitis: Current Concepts in Pathogenesis. Curr Allergy Asthma Rep 15: 489.
- Samborski W, Stratz T, Sobieska M, Mennet P, Müller W, et al. (1992) Intraindividual comparison of whole body cold therapy and warm treatment with hot packs in generalized tendomyopathy. Z Rheumatol 51: 25-30.
- Offenbächer M, Stucki G (200) Physical Therapy in the Treatment of Fibromyalgia. Scand J Rheumatol Suppl 113: 78-85.
- Stanek A, Cieslar G, Strzelczyk J, Kasperczyk S, Sieron-Stoltny K, et al. (2010) Influence of Cryogenic Temperatures on Inflammatory Markers in Patients with Ankylosing Spondylitis. Polish J of Environ Stud 19: 167-175.
- Stanek A, Cholewka A, Wielkoszynski T, Romuk E, Sieron A (2018) Whole-Body Cryotherapy Decreases the Levels of Inflammatory, Oxidative Stress, and Atherosclerosis Plaque Markers in Male Patients with Active-Phase Ankylosing Spondylitis in the Absence of Classical Cardiovascular Risk Factors. Mediators Inflamm 2018: 8592532.
- Banfi G, Lombardi G, Colombini A, Melegati G (2010) Whole-Body Cryotherapy in Athletes. Sports Med 40: 509-517.
- Lubkowska A, Szygula Z, Klimek AJ, Torii M (2010) Do sessions of cryostimulation have influence on white blood cell count, level of IL6 and total oxidative and antioxidative status in healthy men? Eur J Appl Physiol 109: 67-72.
- Stanek A, Cholewka A, Wielkoszynski T, Romuk E, Sieron A (2018) Decreased oxidative stress in male patients with active phase ankylosing spondylitis who underwent whole-body cryotherapy in closed cryochamber. Oxid Med Cell Longev 2018: 7365490.
- Bettoni L, Bonomi FG, Zani V, Manisco L, Indelicato A, et al. (2013) Effects of 15 consecutive cryotherapy sessions on the clinical output of fibromyalgic patients. Clin Rheumatol 32: 1337-1345.
- Rivera J, Tercero MJ, Salas JS, Gimeno JH, Alejo JS (2018) The effect of cryotherapy on fibromyalgia: a randomised clinical trial carried out in a cryosauna cabin. Rheumatol Int 38: 2243-2250.
- Vitenet M, Tubez F, Marreiro A, Polidori G, Taiar R, et al. (2018) Effect of whole body cryotherapy interventions on health-related quality of life in fibromyalgia patients: A randomized controlled trial. Complement Ther Med 36: 6-8.
- Klemm P, Becker J, Aykara I, Asendorf T, Dischereit G, et al. (2021) Serial whole-body cryotherapy in fibromyalgia is effective and alters cytokine profiles. Adv Rheumatol 61: 3.
- Gizinska M, Rutkowski R, Romanowski W, Lewandowski J, Straburzynska-Lupa A (2015) Effects of Whole-Body Cryotherapy in Comparison with Other Physical Modalities Used with Kinesitherapy in Rheumatoid Arthritis. Biomed Res Int 2015: 409174.
- Hirvonen H, Kautiainen H, Moilanen E, Mikkelsson M, Leirisalo-Repo M (2017) The effect of cryotherapy on total antioxidative capacity in patients with active seropositive rheumatoid arthritis. Rheumatol Int 37: 1481-1487.
- Sadura-Sieklucka T, Soltysiuk B, Karlicka A, Sokolowska B, Kontny E, et al. (2019) Effects of whole body cryotherapy in patients with rheumatoid arthritis considering immune parameters. Reumatologia 57: 320-325.
- Klemm P, Hoffmann J, Asendorf T, Aykara I, Frommer K, et al. (2022) Whole-body cryotherapy for the treatment of rheumatoid arthritis: a monocentric, single-blinded, randomised controlled trial Whole-body cryotheraphy in RA / P. Klemm et al. In Clinical and Experimental Rheumatology 40: 2133-2140.
- Stanek A, Cholewka A, Gadula J, Drzazga Z, Sieron A, et al. (2015) Can whole-body cryotherapy with subsequent kinesiotherapy procedures in closed type cryogenic chamber improve BASDAI, BASFI, and some spine mobility parameters and decrease pain intensity in patients with ankylosing spondylitis? BioMed Research International.
- Straburzynska-Lupa A, Kasprzak MP, Romanowski MW, Kwasniewska A, Romanowski W (2018) The effect of whole-body cryotherapy at different temperatures on proinflammatory cytokines, oxidative stress parameters, and disease activity in patients with ankylosing spondylitis. Oxidative Medicine and Cellular Longevity 2157496.
- Romanowski MW, Straburzynska-Lupa A (2020) Is the whole-body cryotherapy a beneficial supplement to exercise therapy for patients with ankylosing spondylitis? Journal of Back and Musculoskeletal Rehabilitation 33: 185-192.
- Kujawski S, Bach AM, Slomko J, Pheby DFH, Murovska M, et al. (2021) Changes in the allostatic response to whole-body cryotherapy and static-stretching exercises in chronic fatigue syndrome patients vs. Healthy individuals. Journal of Clinical Medicine 10:
- Kujawski S, Slomko J, Godlewska BR, Cudnoch-Jedrzejewska A, Murovska M, et al. (2022) Combination of whole body cryotherapy with static stretching exercises reduces fatigue and improves functioning of the autonomic nervous system in Chronic Fatigue Syndrome. Journal of Translational Medicine 20: 273.
- Bidonde J, Busch AJ, Webber SC, Schachter CL, Danyliw A, et al. (2008) Director of Quality Improvement, Saskatchewan Health Quality Council. Address reprint requests to A. In J. Busch, School of Physical Therapy 35: 6.
- Jones KD, Adams D, Winters-Stone K, Burckhardt CS (2006) A comprehensive review of 46 exercise treatment studies in fibromyalgia (1988-2005). In Health and Quality of Life Outcomes 4:67.
- Jastrzabek R, Straburzynska-Lupa A, Rutkowski R, Romanowski W (2013) Effects of different local cryotherapies on systemic levels of TNF-α, IL-6, and clinical parameters in active rheumatoid arthritis. Rheumatology International 33: 2053–2060.
- Ksiezopolska-Orlowska K, Pacholec A, Jedryka-Góral A, Bugajska J, Sadura-Sieklucka T (2016) Complex rehabilitation and the clinical condition of working rheumatoid arthritis patients: Does cryotherapy always overtop traditional rehabilitation? Disability and Rehabilitation 38: 1034-1040.
- Peres D, Sagawa Y Jr, Dugué B, Domenech SC, Tordi N, et al. (2017) The practice of physical activity and cryotherapy in rheumatoid arthritis: systematic review. In European journal of physical and rehabilitation medicine 5: 775-787.
- Capodaglio P, Cremascoli R, Piterà P, Fontana JM (2022) Whole-body Cryostimulation: A Rehabilitation Booster. Journal of Rehabilitation Medicine - Clinical Communications 5:2810.
- Sarais P, Rey G, Boni G, Diracoglu D, Lains J, et al. (2023) Whole Body Cryotherapy in Sport and Physical Activity: a Narrative Review. Journal of Orthopaedics and Sports Medicine 5.
- Fontana JM, Bozgeyik S, Gobbi M, Piterà P, Giusti EM, et al. (2022) Whole-body cryostimulation in obesity. A scoping review. In Journal of Thermal Biology 106: 103250.
- Kulis A, Misiorek A, Marchewka J, Glodzik J, Teleglów A, et al. (2017) Effect of whole-body cryotherapy on the rheological parameters of blood in older women with spondyloarthrosis. Clinical Hemorheology and Microcirculation 66: 187-195.
- Kujawski S, Newton JL, Morten KJ, Zalewski P (2021) Whole-body cryostimulation application with age: A review. In Journal of Thermal Biology 96:102861.
- Hirvonen HE, Mikkelsson MK, Kautiainen H, Pohjolainen TH, Leirisalo-Repo M (2006) Effectiveness of different cryotherapies on pain and disease activity in active rheumatoid arthritis. A randomised single blinded controlled trial 24: 295-301.
- Westerlund, Tarja, Oulun yliopisto (2009) Thermal, circulatory, and neuromuscular responses to whole-body cryotherapy. ACTA 2009.
- Miller E (2006) Effectiveness Comparison of Local and Whole Body Cryotherapy in Chronic Pain. Polish Journal of Physiotherapy 6: 27-31.
Citation: Leone R, Malvezzi M, Sarais PM, Guaglianone G, Migliore F, et al. (2024) The Perspective of Whole Body Cryotherapy in Rheumatic Diseases: A Narrative Review. J Phys Med Rehabil Disabil 10: 088.
Copyright: © 2024 Raimondo Leone, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.