The Symptom and Frequency of the Patients with Multiple Myeloma in Osteoporotic Vertebral Body Fracture in the Elderly: A Case Control Study
*Corresponding Author(s):
Kengo HiguchiDepartment Of Orthopaedic Surgery, Fukuoka Kinen Hospital, 1-1-35, Nishijin, Sawaraku, Fukuoka, 814-8525, Japan
Tel:+81 0928214731,
Email:sea_cherry_brossom@yahoo.co.jp
Abstract
Background: In an aging society, osteoporotic vertebral fracture will continue to rise. Multiple myeloma is mostly developed in elderly, so there is also a possibility to increase the number of multiple myeloma. Multiple myeloma patients tend to have osteolysis lesion especially in the vertebral, so they are easy to injury vertebral fractures. In the medical care of osteoporotic vertebral fracture, it is not rare that we meet with undiagnosed multiple myeloma, but there are few reports of the symptom and frequency of the patients with multiple myeloma included in osteoporotic vertebral fracture. In multiple myeloma patients, early treatments improve consequence. So early medical examination by orthopaedist is clinically important. The purpose of this study is to investigate the symptom and frequency of the patients with multiple myeloma included in osteoporotic vertebral fracture.
Methods: Between April 2016 and March 2017, 145 patients was diagnosed osteoporotic vertebral fracture, among these, the 108 patients was chosen with use of our criteria. Among these 108 patients, we examined blood examinations, Bence Jones proteins in urine, monoclonal protein on serum and numbers of vertebral fracture at the first visit to a doctor.
Results: 6.5% (7/108) patients was diagnosed with symptomatic multiple myeloma. The rate between 75 to 84 years old patients was 5.1%, over the 85 years old was 8.2%. In the 7 patients, the mean age was 85, hemoglobin was 7.8g/dL and albumin-globulin ratio was 0.83 that was low value in all 7 patients. Existing vertebral lesion was 6.0 bodies.
Conclusion: Multiple bone lesions or early refracture of vertebral is positively suspicious symptom of MM. The measurement of electrophoresis of protein, albumin-globulin ratio is recommended with vertebral lesion in elderly. The MM patients having bone lesion are likely to first visit orthopaedist, so it is necessary to positively considerate this pathophysiology.
Keywords
Albumin-globulin ratio; Bence Jones proteins; Monoclonal protein; Multiple myeloma; Osteoporotic vertebral fracture
List of Abbreviations
OVF: Osteoporotic Vertebral Fracture
MM: Multiple Myeloma
MRI: Magnetic Resonance Imaging
ORIF: Open Reduction and Internal Fixation
A-G ratio: Albumin-Globulin Ratio
CT: Computed Tomography
PET: Positron Emission Computerized Tomography
Background
In an aging society, OVF [1] will continue to rise. MM [2] is mostly developed in elderly, so there is also a possibility to increase the number of MM patients. MM patients tend to have osteolysis lesion especially in the vertebral, so they are easy to injury vertebral fractures. In the medical care of OVF, it is not rare that we meet with undiagnosed MM, but there are few reports of the symptom and frequency of the patients with MM included in OVF. In MM patients, early treatments improve consequence. So early medical examination by orthopaedist is clinically important. The purpose of this study is to investigate the symptom and frequency of the patients with MM included in OVF.
Methods
From April 2016 to March 2017, OVF was diagnosed 145 patients in our hospital with use of MRI [3]. Among these patients, include over 75- years old, fragility fractures, and exclude under 75-years old and high energy injury cases, complication of infection, medical history of cancer treatment. 108 patients became an object for this study. We examined Bence Jones proteins in urine, monoclonal protein on serum. In case of detecting monoclonal protein, added immunoelectrophoresis, we diagnosed symptomatic MM, and made a comparison between symptomatic MM and OVF. Survey item is corrected calcium, hemoglobin, creatinine, albumin, total protein as blood examinations, and we investigate the numbers of vertebral fracture with use of imaging study at the first visit to a doctor.
Results
We showed the all cases of diagnosing MM [Table 1]. 7 patients within 108 OVF patients (6.5%) was diagnosed symptomatic MM. The rate diagnosed symptomatic MM between 75 and 84 years old was 5.1% (3/59 patients), in over 85 years old was 8.2% (4/49 patients). These results indicated the possibility that MM get mixed with OVF patients especially in elderly. The mean age of symptomatic MM patients was 85.0 years old, corrected calcium was 10.0 mg/dl, hemoglobin was 7.8g/dl, creatinine was 1.09mg/dl, albumin was 3.2g/dl total protein was 7.7g/dl,. The mean A-G ratio7 was 0.91, low value in all cases, and existing vertebral lesion was 6.0 bodies. MM patients were anemic and indicated multiple vertebral lesions with a significant difference than OVF patients. A-G ratio was lower in MM patients than OVF patients but there was no significant difference [Table 2].
|
Case |
Age |
Sex |
C.C |
Ca |
Cr |
Hb |
Tp |
Alb |
A/G ratio |
OVF |
Outcome |
|
1 |
81 |
M |
LBP paralized inferior limbs |
10.9 |
0.94 |
5.3 |
6.5 |
3.3 |
1 |
2 |
Changing hospital (hematology) |
|
2 |
75 |
M |
LBP |
9.6 |
1.05 |
9 |
10.9 |
3.4 |
0.5 |
5 |
Decease |
|
3 |
91 |
F |
LBP |
9 |
0.75 |
11.1 |
8.6 |
3.5 |
0.7 |
9 |
Ambulatory |
|
4 |
84 |
M |
LBP |
9.7 |
1.66 |
8.4 |
5.3 |
2.4 |
1.07 |
9 |
Decease |
|
5 |
88 |
F |
LBP groin pain |
11.1 |
0.96 |
9.6 |
9.2 |
3.8 |
0.7 |
2 |
Changing hospital (hematology) |
|
6 |
89 |
M |
LBP |
10.2 |
0.87 |
10.3 |
7.1 |
2.8 |
0.83 |
11 |
Changing hospital (recuperation) |
|
7 |
83 |
M |
LBP |
9.3 |
1.42 |
11.2 |
6.1 |
3.1 |
1 |
2 |
Changing hospital (hematology) |
|
Mean |
85 |
10.0 |
1.09 |
7.8 |
7.7 |
3.2 |
0.83 |
6 |
Table 1: The all cases of symptomatic MM diagnosed in this study.
|
|
MM |
OVF |
P value |
|
Number of patients |
7 |
101 |
|
|
Age (mean) |
85.0 |
81.2 |
NS |
|
Corrected Ca(mean, mg/dl) |
10 |
9.5 |
NS |
|
Hb (mean, g/dl) |
7.8 |
10.3 |
<0.05 |
|
Cr (mean, mg/dl) |
1.09 |
0.87 |
NS |
|
Alb (mean, g/dl) |
3.2 |
3.8 |
NS |
|
TP (mean, g/dl) |
7.7 |
6.9 |
NS |
|
A-G ratio (mean) |
0.91 |
1.21 |
NS |
|
Numbers of vertebral fracture (mean) |
6.0 |
2.1 |
<0.05 |
Table 2: A comparison between symptomatic MM and OVF. MM patients were anemic and indicated multiple vertebral lesions with a significant difference than OVF patients. A-G ratio was lower in MM patients than OVF patients but there was no significant difference.
Present a case
A 81-years-old man
Chief complaint: Low back pain, paralysis of inferior limbs, bladder and rectal dysfunction.
Present history: He had a fracture of proximal part of femur, due to fall. ORIF [4] was performed immediately as much as possible. Post operation, he changed hospital in order to have rehabilitation. At there, he had persistent low back pain, paralysis of inferior limbs and bladder and rectal dysfunction. The imaging studies showed vertebral body fracture of 4th level. So we had a consultation the case.
Physical examination: He had paralysis of inferior limbs and bladder and rectal dysfunction. Laboratory studies showed low value of hemoglobin (5.3g/dl) and A-G ratio (1.0). In CT [5] scan [Figure 1], there existed osteolysis or crush injury in multiple vertebral body. At the level of 4th, compression of thoracic spinal cord was indicated. In MRI [Figure 2], at the level of 4, 5, 9th low density tumor localized under T1-weightedconditions. 4th vertebral body had burst fracture and it compress thoracic spinal cord. MRI image reading by radiologist indicated the possibility of multiple metastatic vertebral body tumor or multiple myeloma, so we investigated primary lesion minutely by an inspection of tumor marker, gastrointestinal endoscope, contrast radiography of CT, PET [6] of whole body, but there is no significant findings. On immunoelectrophoresis, M protein was detected, and 12% plasma cell was detected with bone marrow biopsy. We diagnosed with MM, the patient changed special hospital of hematology.
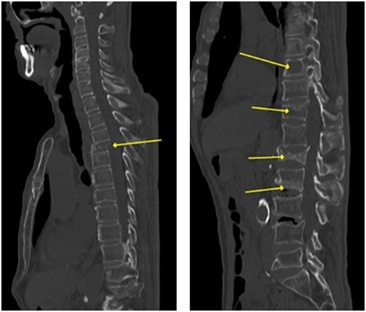 Figure 1: Multiple vertebral osteolysis or fracture was showed in CT scan.
Figure 1: Multiple vertebral osteolysis or fracture was showed in CT scan.
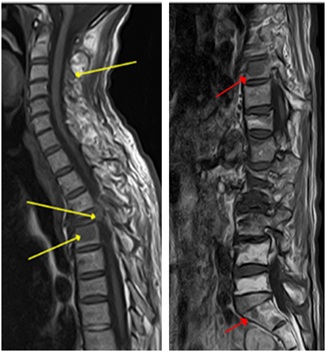 Figure 2: There located low density tumor at the level of 4, 5, 9th under T1-weighted conditions. At the level of 4th, crushed vertebral body compressed thoracic spinal cord.
Figure 2: There located low density tumor at the level of 4, 5, 9th under T1-weighted conditions. At the level of 4th, crushed vertebral body compressed thoracic spinal cord.
Discussion
It is reported as the clinical characteristics of MM that affection rate of MM is highly in middle and old-aged man [1], low back pain is the most as the chief complaint. And also, red flag sign, such as the night pain and the pain in rest, is indicated characteristically [2]. A rate of incidence of MM is about 1% in all malignant neoplasms, it is about 13% in hematologic disease [3]. The frequency of MM is six out of one hundred thousand people (6/100,000) each year [4], and over 65 years old occupy 62.1% of whole MM patients [7]. In this study, 4.8% patients were diagnosed MM in OVF, and 8.2% patients were diagnosed in over 85 age, 5.1% patients were diagnosed in 75 to 84 age. So there is a possibility that MM get mixed with OVF patients especially in elderly. There are several reports that MM patient’s bone lesions are highly localized in vertebral [5,6]. In this study, MM patients also had multiple vertebral lesions, so it is considered that MM patients highly have first medical examination with orthopaedist. There are also reports that 124 parts of vertebral fractures were examined with 50 MM patients, and among them, 76% of patients were not diagnosed MM at the previous time of vertebral injury, 50% of the patients developed vertebral fracture within 4 months after diagnosed MM [6], and the rate of misdiagnosis is 25-60% when the MM patients have first medical examination with orthopaedist [8]. The early examination and the early treatment is necessary. In MM patients, it is reported that MRI is useful indicating a characteristic findings, but clinically, imaging findings are mixed and it is difficult to diagnosis only using imaging findings [Figure 3], so complex judgment is required at clinical place [9,10]. Multiple bone lesion and early refracture of vertebral is positively suspicious symptom of MM. Generally, blood and urine examination is valid procedure of diagnosing MM [11]. The measurement of electrophoresis of protein, A-G ratio is recommended with vertebral lesion in elderly. A-G ratio is useful and simple marker of diagnosing MM, but laboratory data of A-G ratio tends to overlooked by a surgeon. So we should have medical examination in mind this disease state.
 Figure 3: Imaging findings of case 2 and case 6. Localized tumor and fracture findings are mixed both of cases.
Figure 3: Imaging findings of case 2 and case 6. Localized tumor and fracture findings are mixed both of cases.
Conclusion
We reported about MM experienced in our hospital. Multiple bone lesion and early refracture of vertebral is positively suspicious symptom of MM. The measurement of electrophoresis of protein, A-G ratio is recommended with vertebral lesion in elderly. The MM patients having bone lesion is likely to first visit orthopaedist, so it is necessary to positively considerate this pathophysiology.
Declarations
Ethics approval and consent to participate
The study was conducted correspondingly to the World Medical Association’s Declaration of Helsinki. All participants were given verbal- and written information about the trial before providing their written informed consent to participate in the trial. All participants were made aware of their possibility to voluntarily terminate their participation at any time.
Consent for publication
Non-identifiable descriptive data only is presented in this paper. All participants were aware and consented to non-identifiable information to be included in a publication.
Availability of data and materials
The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Competing interests
The authors declare that they have no competing interests.
Funding
There is no funding.
Authors' contributions
KH wrote and prepared the manuscript, and all of the authors SK, HH, MM participated in the study design, reading, reviewing and approved the article.
Acknowledgement
Not applicable.
References
- Kyle RA, Gertz MA, Witzig TE, Lust JA, Lacy MQ, et al. (2003) Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc 78: 21-33.
- van Tulder M, Becker A, Bekkering T, Breen A, del Real MT, et al. (2006) Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. Eur Spine J 15: 169-191.
- Angtuaco EJ, Fassas AB, Walker R, Sethi R, Barlogie B (2004) Multiple Myeloma: Clinical Review and Diagnostic Imaging. Radiology 231: 11-23.
- Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, et al. (2010) SEER Cancer Statistics Review, 1975–2007. National Cancer Institute, Bethesda, USA.
- Khan OA, Brinjikji W, Kallmes DF (2014) Vertebral Augmentation in Patients with Multiple Myeloma: A Pooled Analysis of Published Case Series. AJNR Am J Neuroradiol 35: 207-210.
- Miller JA, Bowen A, Morisada MV, Margetis K, Lubelski D, et al. (2015) Radiologic and clinical characteristics of vertebral fractures in multiple myeloma. Spine J 15: 2149-2156.
- Kristinsson SY, Landgren O, Dickman PW, Derolf AR, Björkholm M (2007) Patterns of Survival in Multiple Myeloma: A Population-Based Study of Patients Diagnosed in Sweden From 1973 to 2003. J Clin Oncol 25: 1993-1999.
- Dimopoulos M, Terpos E, Comenzo RL, Tosi P, Beksac M,, et al. (2009) International myeloma working group consensus statement and guidelines regarding the current role of imaging techniques in the diagnosis and monitoring of multiple myeloma. Leukemia 23: 1545-1556.
- Uetani M, Hashmi R, Hayashi K (2004) Malignant and benign compression fractures: Differentiation and diagnostic pitfalls on MRI. Clin Radiol 59: 124-131.
- Yanik B, Tur BS, Kutlay S (2005) Metastatic vertebral tumor misdiagnosed in magnetic resonance imaging as benign degenerative bone marrow changes: A case report. Rheumatol Int 25: 384-387.
- Duffy TP (1992) The many pitfalls in the diagnosis of myeloma. N Engl J Med 326: 394-396.
Citation: Higuchi K, Kumamoto S, Honke H, Mawatari M (2021) The Symptom and Frequency of the Patients with Multiple Myeloma in Osteoporotic Vertebral Body Fracture in the Elderly: A Case Control Study. J Gerontol Geriatr Med 7: 095.
Copyright: © 2021 Kengo Higuchi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.