Journal of Angiology & Vascular Surgery Category: Medical
Type: Case Report
Trans Obturator Ilio-Femoral Bypass in Case of Ruptured Left Common Femoral Artery Pseudoaneurysm
*Corresponding Author(s):
Amr Abdelghaffar MahmoudSpecialist And Assistant Lecturer Of Vascular Surgery, Ain Shams University, Cairo, Egypt
Tel:+20 1003521634,
Email:amr.mahmoud@med.asu.edu.eg
Received Date: Feb 09, 2018
Accepted Date: Apr 16, 2018
Published Date: Apr 30, 2018
Abstract
Context: Trans-obturator bypass may be a good solution in hostile groin either scared or infected in Intravenous (IV) drug addict patients.
Objective: To report a case of infected groin treated with trans-obturator bypass.
Subjects and Methods: A case of trans-obturator bypass was performed for IV addict patient with infected groin. Ilio-femoral bypass was performed. The tunnel was fashioned in a plane deep to the adductor muscles to be away from the infected areas.
Results: Acute Ischemia was resolved, patent graft for the 6 months follow up.
Conclusion: Trans-obturator bypass may be a good alternative or a good solution in hostile groin (scared or infected) with severe sepsis in drug addict patient.
The procedure should not be omitted from the armamentarium of any vascular surgeon.
Keywords
Infected groin; Obturator bypass; Pseudoaneurysm
INTRODUCTION
The obturator bypass was initially employed to avoid infected groin during revascularizations [1]. An example of infected groin is infected CFA pseudoaneurysm in cases of Intravenous (IV) addict patients which is common in young age and represents a challenge for proper management [2]. Important factors that must be considered before performing such a bypass include the proper assessment of adequate inflow, outflow, and the anatomic site of infection [3].
A review of the literature showed 1 and 5-year patency rates for all indications of obturator bypass to be 71% and 60%, respectively [4]. As the procedure is generally safe, this extra anatomic bypass should be included in the armamentarium of the vascular surgeon.
SUBJECTS AND METHOD
This is a case report. In this case report, 32 years old female patient has no past history of medical illness (Non diabetic nor hypertensive). The patient is IV addict (Heroin addict). She presented with ruptured Lt Common Femoral Artery (CFA) pseudoaneurysm and infected left groin.
Surgical technique
• Excision of infected arterial segment and ligation of External Iliac Artery (EIA) distally as possible and Ligation of Superficial Femoral Artery (SFA)
• First day postoperatively, patient developed left Lower Limb (LL) acute ischemia Rutherford stage II b in the form of absent distal pulsation, absent Dopplersignals, decrease motor power and coldness
• She received urgent operation in the form of trans-obturator ilio-femoral bypass (between EIA proximal to ligation site and distal to SFA) (Figure 1)
• Type of bypass is synthetic bypass using 8 mm ringed Polytetrafluoroethylene (PTFE) graft
• The tunnel was fashioned in a plane deep to the adductor muscles to be rather away from the infected areas without need of leg fasciotomy
• The infection was deep seated at left groin with affection skin, subcutaneous tissue and femoral vessel with subsequent pseudoaneurysm at CFA. Muscles of medical compartment and anterior compartment of thigh are viable with no need for muscle debridement
• First day postoperatively, patient developed left Lower Limb (LL) acute ischemia Rutherford stage II b in the form of absent distal pulsation, absent Dopplersignals, decrease motor power and coldness
• She received urgent operation in the form of trans-obturator ilio-femoral bypass (between EIA proximal to ligation site and distal to SFA) (Figure 1)
• Type of bypass is synthetic bypass using 8 mm ringed Polytetrafluoroethylene (PTFE) graft
• The tunnel was fashioned in a plane deep to the adductor muscles to be rather away from the infected areas without need of leg fasciotomy
• The infection was deep seated at left groin with affection skin, subcutaneous tissue and femoral vessel with subsequent pseudoaneurysm at CFA. Muscles of medical compartment and anterior compartment of thigh are viable with no need for muscle debridement
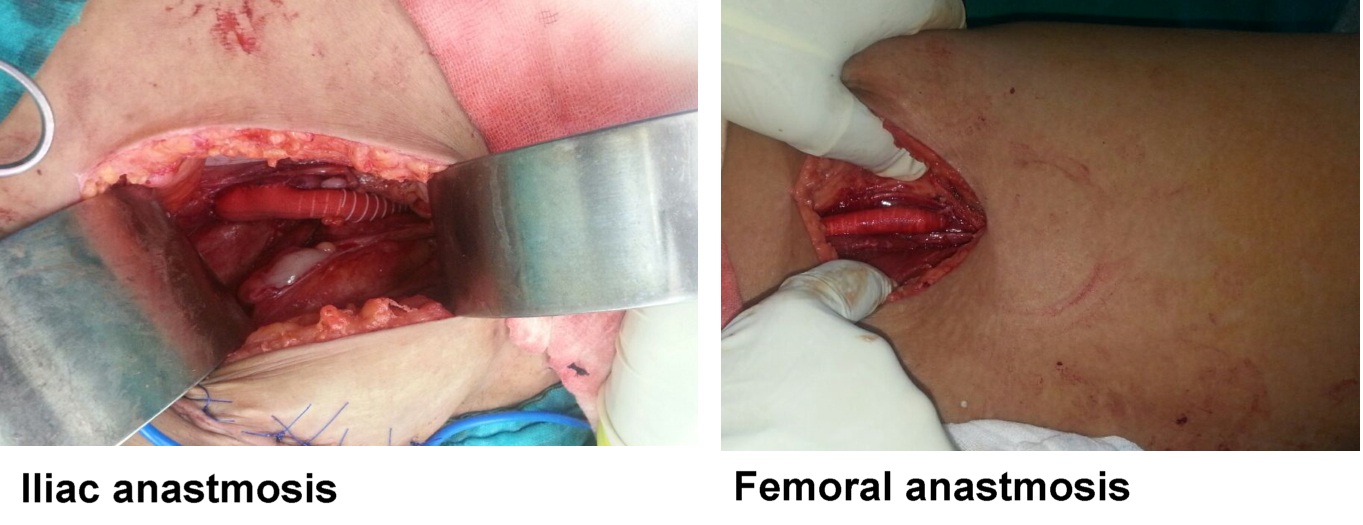 Figure 1: Iliac anastomosis and femoral anastomosis using PTFE graft 8 mm.
Figure 1: Iliac anastomosis and femoral anastomosis using PTFE graft 8 mm.Aim of study
It’s a single case report study. To report a case of infected groin treated with trans-obturator bypass.
DISCUSSION
The extra-anatomical transobturator bypass represents available option in situations where the groin is no longersafe for revascularization [4]. Whenever the groin infection was marked, a deeper tunnel in the thigh was created where the graft was routed deep to the adductor magnus tendon to be away from the infected areas. Some authors pertained that a subcutaneous tunnel should better be avoided in drug abusers who may reinject themselves through the graft [5].
Attention to technical details was important, assuring a straight course of the graft [6]. This could be seen in follow-up CT angiographies. An 8 mm PTFE graft was also used by other authors [4]. No kinks of the graft or change of the ankle/brachial index occurred with flexion of the hip joint [7].
The approach to the donor vessel may be carried out either retroperitoneally or transperitoneally. Some authors favored a direct transperitoneal approach [4]. Another study reported a preference for extraperitoneal access with this technique; retroperitoneal approach carries a diminished risk of complications as peritoneal irritation, infection, and postoperative ileus [1]. Complications of trans obturator bypass are shortlisted in table 1.
| Intraoperative complications |
| Hemorrhage [1] |
| Bladder perforation [3] |
| Bypass misplacement (vaginal transgression) [1] |
| Injury to neurovascular bundle [8] |
| Rectal perforation [9] |
| Postoperative complications |
| Graft infection1 [10] |
| Occlusion (early and late) [10] |
| Muscle necrosis [11] |
| False aneurysm of graft1 [8] |
| Recurrent hemorrhage secondary to persistent Infection [1] |
Table 1: Complications of trans obturator bypass.
RESULTS
Acute lower limb ischemia has resolved. Patient has intact pedal pulsation.
The graft is still patent for the 6 months follow up (Ultrasound is the tool for follow up).
The graft is still patent for the 6 months follow up (Ultrasound is the tool for follow up).
CONCLUSION
Trans- obturator bypass may be a good alternative or a good solution in hostile groin (scared or infected) with severe sepsis in drug addict patient.
The procedure should not be omitted from the armamentarium of any vascular surgeon.
The procedure should not be omitted from the armamentarium of any vascular surgeon.
REFERENCES
- Sautner T, Niederle B, Herbst F, Kretschmer G, Polterauer P, et al. (1994) The value of obturator canal bypass. A review. Arch Surg 129: 718-722.
- Fromm SH, Lucas CE (1970) Obturator bypass for mycotic aneurysm in the drug addict. Arch Surg 100: 82-83.
- Guida PM, Moore SW (1969) Obturator bypass technique. Surg Gynecol Obstet 128: 1307-1316.
- Rabbani A, Moini M, Rasouli MR (2008) Obturator bypass as an alternative technique for revascularization in patients with infected femoral pseudoaneurysms. Arch Iran Med 11: 50-53.
- Salehian MT, Shahid N, Mohseni M, Ghodoosi I, Marashi SA, et al. (2006) Treatment of infected pseudoaneurysm in drug abusers: Ligation or reconstruction? Arch Iran Med 9: 49-52.
- Ruangsetakit C, Chinsakchai K, Hahtapornsawan S, Wongwanit C, Sermsathanasawadi N, et al. (2012) Successful outcome of obturator bypass surgery in infected femoral pseudoaneurysm: Three cases report and literature review. J Med Assoc Thai 95: 470-475.
- Pearce WH, Ricco JB, Yao JS, Flinn WR, Bergan JJ (1983) Modified technique of obturator bypass in failed or infected grafts. Ann Surg 197: 344-347.
- Van Det RJ, Brands LC (1981) The obturator foramen bypass: An alternative procedure in iliofemoral artery revascularization. Surgery 89: 543-547.
- Sheiner NM, Sigman H, Stilman A (1969) An unusual complication of obturator foramen arterial bypass. J Cardiovasc Surg (Torino) 10: 324-328.
- Prenner KV, Rendl KG (1982) Indications and technique for obturator bypass. In: Greenhalgh RM, (ed). Extra-anatomic and secondary arterial reconstruction. Pitman Books, London, pg no: 406.
- Geroulakos G, Parvin SD, Bell PR (1988) Obturator foramen bypass--the alternative route for sepsis in the femoral triangle. Acta Chir Scand 154: 111-112.
Citation: Mahmoud AA, Kamel AN (2018) Trans Obturator Ilio-Femoral Bypass in Case of Ruptured Left Common Femoral Artery Pseudoaneurysm. J Angiol Vasc Surg 3: 014.
Copyright: © 2018 Amr Abdelghaffar Mahmoud, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!