Treatment of Periapical Infected Site and Bony Defect in the Maxillary Esthetic Zone by Extraction & Immediate Implant Placement Particulate Equine Xenograft & Equine Pericardial GTR Membrane: A Case Report
*Corresponding Author(s):
Sudhanshu AgrawalDepartment Of Periodontology, Chandra Dental College & Hospital, Barabanki, India
Tel:+91 9415400591,
Email:drsudhanshu_bds@hotmail.com
Abstract
Immediate placement and restoration of the implant is a widely used protocol, but loading of implants in the site which is periapically infected is still not very popular. Very few studies have been conducted and it’s still in debate. The conventional protocol of placing implant and waiting for it to osseointegrate is time consuming and compromises patient’s esthetics and psychological comfort. This report presents a case of immediate placement and restoration of implant in the region with periapical infection.
Keywords
Dental implant; Immediate placement; · Periapical lesion; Restoration
Introduction
The concept of placement of implants into the freshly extracted sockets was introduced in the late 1970s but the use and success regarding the same has been achieved in the last few years [1]. Soon after the extraction of a tooth, the bone undergoes resorption and changes are seen in the bone volume. By placing the implant immediately in the socket, this bone loss can be prevented up to a certain extent. The advantages of immediate placement and load- ing in the fresh extraction sites compared to conventional loading are compliance to both dentist and the patient, reduced appointments, shorter treatment time, faster esthetic and functional results and higher success rates. Despite all these advantages there is a risk of microbial intervention in cases with periapical lesion which can delay the process of osseointegration [2]. The placement of implant immediately after tooth extraction with periapical lesion is still a debate and requires more studies to be conducted. However, Douglas had stated that in sockets with 3-4 intact walls, minimal periodontal resorption and good primary stability, immediate implantation is a safe procedure [3]. There are several reports which state the success of implants in the regions with periapical infection. A report by Siegenthaler and Lindeboom suggested that the complication rates with implants placed in the infected sites compared to those of non-infected sites are almost the same [4]. Novaes Jr, et al. and Novaes, et al. in their study stated success by few pre and post operative measures including antibiotic administration, meticulous cleaning, and alveolar debridement [5]. This case report describes the immediate placement and loading of implant in replacing teeth with periapical lesions in max illary anterior zone.
Case Report
A 29 year old non-smoker female patient in good health conditions and without any chronic diseases was reported with the history of dull pain and discharge in relation to maxillary left central incisor in which RCT was done previously and PFM crown was placed (Figure 1).
 Figure 1: Pre operative clinical view.
Figure 1: Pre operative clinical view.
On examination, failure RCT in left maxillary lateral incisor was observed radiographically confirming a large periapical pathology associated with the 21 (Figure 2). Case was referred to the endodontist; extraction was advised by the endodontist. Since the tooth was in a esthetic region the patient did not want to have a removable prosthesis extraction, so he was convinced for extraction of 21 following immediate implant placement under antibiotic coverage.
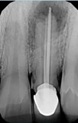 Figure 2: Pre operative radiograph.
Figure 2: Pre operative radiograph.
Diagnostic impressions were made and the casts were poured. Pre-operative radiographs orthopantomographs, IOPA and RVG with respect to 21 were taken. Oral antibiotics, amoxicillin 500 mg (tid) was started 2 days prior to the surgery.
Surgical Procedure
Pre-operative antibiotics and analgesic were prescribed and the patient was prepared in a sterile environment. Local anesthesia lignocaine 2% containing 1:80,000 adrenalines was injected in the area of surgery as an infiltration. The surgical access was obtained and the tooth was extracted with an anterior forceps with minimal tissue damage to preserve the gingiva as well as the bone and combined muco-periosteal flap was reflected on labial aspect and only mucosal flap on palatal side. The combined flap provides advantage of proper flap closure after implant placement complete closure of surgical site (Figure 3).
 Figure 3: Extraction of Tooth with Curettage
Figure 3: Extraction of Tooth with Curettage
The socket was debrided following the extraction and a small defect in the apical region of the socket was observed on the labial side. Hence, the osteotomy site (Figure 3) was prepared on the palatal wall and an Adin implant (4.5 mm in diameter and 11 mm in length) was placed (Figure 4).
 Figure 4: Implant Placed.
Figure 4: Implant Placed.
Since there was a large defect, graft material is used in the socket to fill the gap between implant and socket as this could cause failure of the implant. It is also observed that grafting is necessary when immediately loaded as the epithelium would not migrate into the socket instead form around the provisional and maintaining the architecture of the gingival (Figure 5). At the surgical sites, the defect was filled up with a equine based bone graft substitute Collagen granules Bio-Gen (Bioteck®, Italy) and covered with a resorabale pericardial derived equine based Biocollagen GTR membrane (Bioteck® Italy), and sutures given (Figure 6).
 Figure 5: Bone Graft Materials and Membrane Placed.
Figure 5: Bone Graft Materials and Membrane Placed.
 Figure 6: Clinical photograph showing [bio-absorbable equine collagen membrane (Biocollagen®)1 & equine bone graft (Bio-Gen®)2].
Figure 6: Clinical photograph showing [bio-absorbable equine collagen membrane (Biocollagen®)1 & equine bone graft (Bio-Gen®)2].
1Biocollagen®, the product support bone remodelling phase, Lyophilized Equine bioabsorbable collagen membrane, 25 x 25 x 0.2 mm, Bioteck, Torino, Italy.
2Bio-Gen®, bone tissue of animal Equine origin “xenograft”, deantigenized for total reabsorption, Bio-Gen Mix, Cortical-Spongy, GR. 0.5 size 0.5 - 1 mm, Bioteck, Torino, Italy.
Bone formation would take place in the gap between the socket and implant in a period of 2 months. Sutures were done following the placement and loading of implant.
Postoperative Management
After the surgical procedure the antibiotic therapy (amoxicillin 500 mg, 3 times/day) was continued for 5 more days. Anti-inflammatory and analgesics were prescribed for 3 days. The use of 0.2 % chlorhexidine was indicated for 7 days with no dilution. The patient was recalled after one week for the follow-up.
Follow-up
Following a 3 months healing period, patient was recalled for the definitive prosthesis. Radiographic evaluation did not reveal any lesion. Definitive prosthesis was fabricated and cemented (Figures 6&7). At 1-year regular follow-up examination, the implant was fully osseointegrated with satisfactory functional and esthetic conditions without any lesion or periapical pathology (Figure 8).
 Figure 6: 3 months regular follow-up.
Figure 6: 3 months regular follow-up.
 Figure 7: Implant Exposed For Placing Abutment.
Figure 7: Implant Exposed For Placing Abutment.
 Figure 8: 1-year regular follow-up.
Figure 8: 1-year regular follow-up.
Discussion
The primary objective of implants is to restore the function and esthetics. In order to reduce the bone resorption and to maintain the esthetics, immediate placement and loading is the treatment option which has been put forward by several authors and is widely used. But placement into the extraction site with periapical lesion is still a questionnaire and many studies are being conducted on the same. Casap, et al. conducted a study in which 30 implants were immediately placed into debrided infected sites in 20 patients and obtained 97.6 % success rate [6]. One implant failed immediately after restoration. Fabbro, et al. got excellent clinical results after immediate placement of implants following extraction along with PRGFs [1].
Many authors consider placement of an implant in a socket with periapical lesion as a contraindication, but several studies which were conducted do not show any signifi- cant difference compared to those with healthy sockets.
There was a slight gingival recession which was observed and it was masked with the gingival porcelain. If the underlying and surrounding bone is sound a more esthetic result can be obtained.
The causative factor for the endodontic lesions is mixed infections which are dominated by anaerobic bacteria’s. Most commonly which are found are fusobacterium, prevotella, porphyromonas, actinomyces [6]. The meticulous debridement of the infected socket along with pre and post operative antibiotics helps in eradicating the presence of the microorganisms at the particular site, thus establishing favourable conditions for bone healing and osseointegration.
While this case report presented successful results by placing implant immediately in an infected site with peri- apical infection, other factors should be considered as well for the same. Proper case selection, differentiating and debridement of the granulation tissue, and skills to the proposed protocol contribute for the esthetic and functional outcome [5]. Thorough debridement of the socket after the extraction can play a major role in the success of the implant.
Conclusion
Immediate implant placement and loading represents a viable treatment option for infected sites when combined along with antibiotic regime and complete elimination of microbiota from the infection socket. Although equine based bone graft substitute Collagen granules Bio-Gen (Bioteck®, Italy) and equine based Biocollagen GTR membrane (Bioteck® Italy) has shown promising results on clinical and radiographic evaluation, additional long-term studies should be undertaken to obtain more clinical evidence for regular use of this material.
References
- Fabbro M, Boggian C, Taschieri S (2009) Immediate implant placement into fresh extraction sites with chronic periapical pathologic features combined with plasma rich in growth factors: preliminary results of single-cohort study. J Oral Maxillofac Surg 67: 2476-2484.
- Chang S-W, Shin S-Y, Hong J-R, Yang S-M, Yoo H-M, et al. (2009) Immediate implant placement into infected and non-infected extraction sockets: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107: 197-203.
- Bell C et al (2011) The immediate placement of dental implants into extraction sites with periapical lesions: a retrospective chart J Oral Maxillofac Surg 69: 1623-1627.
- Crespi R, Cappare P, Gherlone E (2010) Fresh-socket implants in periapical infected sites in J Periodontol 81: 378-383.
- Novaes AB Jr, Novaes AB et al (1998) Immediate implants placed into infected sites: a histomorphometric study in dogs. Int J Oral Maxillofac Implants 13: 422-427.
- Casap N, Zeltser C et al (2007) Immediate placement of dental implants into debrided infected dentoalveolar sockets. J Oral Maxillofac Surg 65: 384-392.
Citation: Agrawal N, Kishore A, Sharma KS, Singh M, Mehta DS, et al. (2022) Treatment of Periapical Infected Site and Bony Defect in the Maxillary Esthetic Zone by Extraction & Immediate Implant Placement Particulate Equine Xenograft & Equine Pericardial GTR Membrane: A Case Report. J Clin Stud Med Case Rep 9: 0127.
Copyright: © 2022 Neeraj Agrawal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.