Two-Stage Hybrid Open and Endovascular with Uncovered Stents Repair of a Crawford Type V Aortic Aneurysm
*Corresponding Author(s):
Carlos Alberto Da Silva Frias NetoDepartment Of Vascular And Endovascular Surgery, Presidente Dutra Hospital, Sao Luis, Brazil
Abstract
Thoracoabdominal Aortic Aneurysm (TAAA) is a morbid condition, and the management of these aneurysms has historically involved open surgery. However, this approach has high rates of morbidity and mortality, necessitating the development of alternative practices, especially in complex aneurysms. We present a case of a patient with modified Crawford classification type V TAAA. The patient underwent hybrid repair in two stages. Initially a PTFE graft was implanted surgically with revascularization of superior mesenteric artery from the right external iliac artery (debranching). On a later date, the second stage of treatment was with an endovascular technique with two thoracic endoprothesis and uncovered stents for renal arteries. The patient was discharged with no endoleaks and in good clinical condition, normal food intake and present eliminations, besides preserved renal function.
Keywords
INTRODUCTION
Thoracoabdominal Aortic Aneurysm (TAAA) is a morbid conditionof difficult resolution due to the involvement of visceral arteries, and the management of these aneurysms has historically involved open surgery [1]. Open repair of aortic aneurysm has high rates of morbidity and mortality, necessitating the development of alternative practices, especially in complex aneurysms. Hybrid repair has been increasingly used as an alternative to open repair techniques since the procedure was first described in 1999 [2]. In the other hand, endovascular techniques are developing and gaining space, among them are included the sandwich technique, chimney technique, periscope technique and more advanced devices such as fenestrated and ramified endoprothesis.
The choice for one technique depends on the anatomy of the aorta and visceral branches, the clinical conditions of the patient, the ability of the surgeon and the structure of the health unity. Depending on the case a combination of techniques can be done to reach a better result.
The objective of this paper is to show a case report of a treatment of a thoracoabdominal aortic aneurysm using association of surgical and endovascular techniques.
CASE REPORT
A 49-year-old male patient with hypertension was admitted to the University Hospital of Universidade Federal do Maranhao, with a history of sharp, severe pain between the shoulder blades. Thoracic and abdominal CT scans wereperformed. A type V thoracoabdominal aortic aneurysm was detected (according modified Crawford classification type V: sixth intercostal space to just above the renal arteries) with a larger diameter of 5.9cm (Figure 1).
 Figure 1: A type V thoracoabdominal aortic aneurysm.
Figure 1: A type V thoracoabdominal aortic aneurysm.
It was decided by a hybrid approach of the aneurysm, with first stage being performed by open surgery and second stage by endovascular treatment. The open surgery, consisted of xipho-pubic laparotomy, transperitoneal dissection of the right common iliac artery and the superior mesenteric artery, followed by a bypassfromthe right common iliac artery to the superior mesenteric artery with PTFE prosthesis of 6mm (Figure 2).
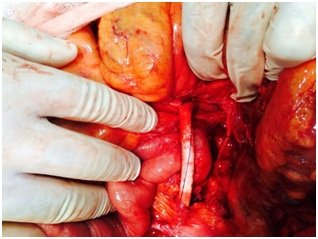 Figure 2: Bypass of the right common iliac artery to the superior mesenteric artery with PTFE.
Figure 2: Bypass of the right common iliac artery to the superior mesenteric artery with PTFE.
Nine days later, the endovascular procedure was performed. In this procedure, a transverse incision and dissection of the left common femoral artery and puncture in the right common femoral artery were performed. From the left femoral access, thoracic endoprosthesis E-Vita (from Jotec company) 33mm x 130mm was introduced with a proximal end at the descending aorta. A second thoracic endoprothesis E-Vita 33mm x 170mm was introduced inside the first one with the distal end distal and below the renal arteries. At the same time, two self-expanding stents of 6mm x 40mm were placed in the renal arteries (technique called inverted and open chimney technique or open periscope technique).
Control aortography demonstrated Endoleak (leaking to the aneurysmal sac) type II, appearing to be from the celiac trunk (covered by endoprosthesis) (Figure 3).
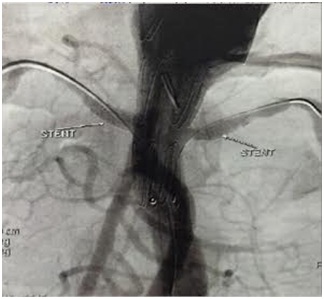 Figure 3: Endovascular repair with uncovered stents to renal arteries and endoleak.
Figure 3: Endovascular repair with uncovered stents to renal arteries and endoleak.
Control angiotomography demonstrated Endoleak persistence without clearly demonstrating the origin of endoleak (Figure 4).
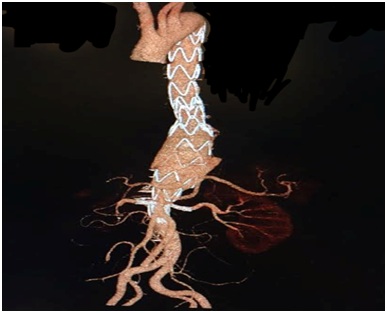 Figure 4: Control angiotomography demonstrated Endoleak persistence.
Figure 4: Control angiotomography demonstrated Endoleak persistence.
Then, sixteen days later, arteriography was performed by the right common femoral artery, the PTFE graft was catheterized, and then aortography above the endoprosthesis, no further signs of endoleak were observed (Figures 5 and 6).
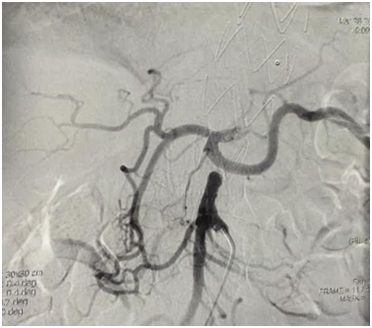 Figure 5: Angiography showing no signs of endoleak.
Figure 5: Angiography showing no signs of endoleak.
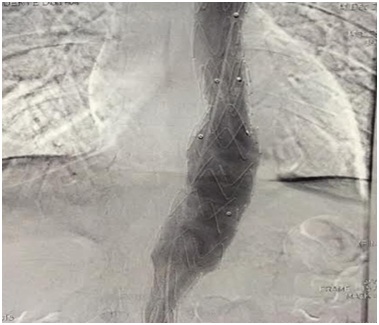 Figure 6: Angiography showing no signs of endoleak.
Figure 6: Angiography showing no signs of endoleak.
The patient was discharged after twenty days, in good clinical condition, normal food intake and present eliminations, besides preserved renal function. Outpatient return was scheduledfor 30 days after discharge.
DISCUSSION
Minimally invasive endovascular aneurysm repair was first reported in 1986. The three principal randomized trials comparing endovascular and open repair of abdominal aortic aneurysm have all shown a marked benefit of endovascular repair with respect to 30-day operative mortality [3].
Several groups have reported using hybrid approaches in which open visceral bypass grafting secures organ perfusion and subsequent stent graft placement achieves endoluminal exclusion of the entire TAAA [4]. The appeal of the hybrid approach (depending on aneurysm location) includes the avoidance of chest cavity invasion, aortic cross-clamping and circulatory support that is necessary in open repair [2]. However, there is little data in the literature to support the combined technique as better, worse, or equivalent to the open repair or simply medical treatment alone [5].
In 2007, Black and coworkers from St Mary’s Hospital, London, published their early results with a combined endovascular and surgical approach for the treatment of TAAA type I - III in 29 patients in a single step approach [6]. They demonstrated good feasibility and the encouraging results of reducing the mortality from 31% to 13% and no paraplegia in this high-risk group of patients. Another study reported their 6-year experience with the visceral hybrid procedure for high-risk TAAA and Chronic Expanding Aortic Dissections (CEAD), a series of 28 patients (20 male, mean age 66 years) were treated between January 2001 and July 2007. Their results are in accordance with the Black and coworkerspublication and add further information on visceral hybrid procedures in the thoracoabdominal aorta [7].
In complex aortic arch disease hybrid procedures were associated with a relatively high primary failure rate. Most failures were associated with type I or type III endoleak, which, in most cases, was successfully managed with extension grafts. The other causes of primary failure were major technical adverse events that required conversion to open surgery, sometimes resulting in death. The overall perioperative mortality and morbidity rates seem to be similar to those associated with open repair [8].
Associated to the complexity of this procedure was the use of an advanced endovascular technique, such as “inverted chimney” or “periscope”. Due the limitations of our public hospital, this technique was made with bare metal stents (or uncovered stents). The “open periscope” or “open chimney” technique was already demonstrated by other surgeons with good results [9,10].
In this case, we were successful in the treatment of the aneurysm by hybrid technique. The intention of the author was to perform less aggressive and shorter procedures, but still aiming for good results. No doubt perform bypass to all visceral branches would be a good option, but it would also significate greater morbidity.In the early postoperative period, we observed type II endoleak, appearing to be from the celiac trunk, which had spontaneous resolution without the need for a complementary approach. One review showed that intentional coverage of the Celiac Artery (CA) can be safely performed with a wide variety of endografts, as the use of various devices in the United States, Europe, and Asia was reported in the literature. Embolization of the CA prior to aortic endograft deployment is advocated by some to prevent the potential development of a type II endoleak into the aneurysm sac. However, only 21 (23%) reported cases underwent this additional procedure. In the remaining 72 patients, three (4%) developed a delayed type II endoleak on CTA evaluation during postoperative follow-up [11].
Despite the complexityof this advanced aortic aneurysm repair, hybrid open-endovascular with uncovered stents repair provides a feasible option of treatment for a hospital structure that do not provide better options and for high-risk population that are not suitable for conventional open repair [2].
CONCLUSION
The hybrid open-endovascular with uncovered stents repair provides a feasible option of treatment with good results in short term.
REFERENCES
- Wong R, Parenti JL, Green SY, Chowdhary V, Liao JM, et al. (2011) Open repair of thoracoabdominal aortic aneurysm in the modern surgical era: Contemporary outcomes in 509 patients. J Am Coll Surg 212: 569-579.
- Almerey T, Moore J, Farres H, Selim M, Agnew R, et al. (2018) Postoperative outcomes of complex aortic aneurysm repair using hybrid open-endovascular techniques. Annals of Vascular Surgery 47: 8.
- Greenhalgh RM, Brown LC, Powell JT, Thompson SG, Epstein D, et al. (2010) Endovascular versus open repair of abdominal aortic aneurysm. N Engl J Med 362: 1863-1871.
- Coselli JS, Bozinovski J, LeMaire SA (2007) Open surgical repair of 2286 thoracoabdominal aortic aneurysms. Ann Thorac Surg 83: 862-864.
- Donas KP, Czerny M, Guber I, Teufelsbauer H, Nanobachvili J (2007) Hybrid open-endovascular repair for thoracoabdominal aortic aneurysms: Current status and level of evidence. European Journal of Vascular and Endovascular Surgery 34: 528-533.
- Black SA, Wolfe JH, Clark M, Hamady M, Cheshire NJ, et al. (2006) Complex thoracoabdominal aortic aneurysms: Endovascular exclusion with visceral revascularization. J Vasc Surg 43: 1081-1089.
- Böckler D, Kotelis D, Geisbüsch P, Hyhlik-Dürr A, Klemm K, et al. (2008) Hybrid procedures for thoracoabdominal aortic aneurysms and chronic aortic dissections - a single center experience in 28 patients. J Vasc Surg 47: 724-732.
- Antoniou GA, El Sakka K, Hamady M, Wolfe JH (2010) Hybrid treatment of complex aortic arch disease with supra-aortic debranching and endovascular stent graft repair. Eur J Vasc Endovasc Surg 39: 683-690.
- Hiramoto JS, Chang CK, Reilly LM, Schneider DB, Rapp JH, et al. (2009) Outcome of renal stenting for renal artery coverage during endovascular aortic aneurysm repair. J Vasc Surg 49: 1100-1106.
- Ducasse E, Lepidi S, Brochier C, Deglise S, Berard X, et al. (2014) The “Open” chimney graft technique for juxtarenal aortic aneurysms with discrepant renal arteries. Eur J Vasc Endovasc Surg 47: 124-130.
- Jim J, Caputo FJ, Sanchez LA (2013) Intentional coverage of the celiac artery during thoracic endovascular aortic repair. J Vasc Surg 58: 270-275.
Citation: da Silva Frias Neto CA, Felice KP, de Brito Filho SB, Durans MSB (2019) Two-Stage Hybrid Open and Endovascular with Uncovered Stents Repair of a Crawford Type V Aortic Aneurysm. J Surg Curr Trend Innov 3: 013.
Copyright: © 2019 Carlos Alberto da Silva Frias Neto, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.