Validation of Caprini’s Saphenous Ablation Scores
*Corresponding Author(s):
Fakhry ADepartment Of Vascular Surgery, Egyptian Military Academy, Egypt
Tel:+20 1223779844,
Email:ayman_vasc@live.com
Abstract
Introduction: Deep Vein Thrombosis (DVT) after varicose vein surgery is well recognized. Less well documented is Endovenous Heat-Induced Thrombosis (EHIT), thrombus extension into a deep vein after superficial venous thermo ablation. There is no current agreement on the routine use of thromboprophylaxis in patients undergoing varicose vein surgery. more data on the incidence of VTE, and the need for postoperative thromboprophylaxis are necessary to formulate evidence-based clinical guidelines.
Aim of the study: Comparison of the use of Caprini's Saphenous Ablation Scores versus Standard Caprini’s Score for the prophylaxis of VTE in EVLA.
Patients & Methods: 60 patients admitted to Royal Vascular Center, Alexandria - Egypt. From Jan. 1st, 2021, to June 30th 2021 divided in 3 groups. - Group A) Treated by ablation of Great saphenous vein and received VTE prophylaxis according to Caprini’s Saphenous Ablation Scores Fig 1-A & B - Group B) Treated by ablation of Great saphenous vein and received VTE prophylaxis according to Standard Caprini’s Risk Assessment Score for VTE Fig 2-A&B - C) Treated by ablation of Great saphenous vein without VTE prophylaxis Ablation was done using radial 1480 YAG laser fibers and Post-operative Duplex was done one day, 3 month and one-year.
Results: Age: 35.6+0.2, 34.3+0.5 and 37.6+0.09 years in the 3 groups M/F: 6/14, 8/12 and 7/13. In group A) all patients showed absent reflux post operatively and in all follow up visits. Duplex examination revealed significant reflux in the great saphenous veins in all patients and ranged from 0.7:0.9 Sec. and mean duration 0.7+0.09 Sec. Vein diameter ranged from (0.6: 0.9,X+0.76 CM.) in group A), (0.6: 0.8,X+0.7 CM.) in group B) , (0.5: 0.8,X+0.65 CM.) in group C) According to Caprini’s saphenous score 14 patients 70% were classified as low risk, 4 patients 20% were of moderate risk and 2 patients 10% of high-risk in Group A, while applying standard Caprini’s Score in group B patients revealed: 6 patients 30% were of moderate risk and 14 patients 70% of high risk in Group B) . 3 patients developed superficial thrombophlebitis 15% and one patient 5% developed left calf DVT in Group C, while no VTE events were shown in both A&B Groups Significant drop in CVSS in patients in the three groups.
Conclusion: Risk assessment of patients undergoing varicose veins ablation should be done and applying Caprini’s saphenous score as a better alternative to Standard Caprini’s score for VTE prophylaxis and is considered a safe and cost-effective tool in VTE prevention in these patients.
Keywords
Risk assessment score; Thrombosis prophylaxis; Varicose veins; Venous thromboembolism
Introduction
Laser Ablation of Varicose vein is among the most performed procedures worldwide, Venous Thromboembolism (VTE), either as Deep Venous Thrombosis (DVT) or a potentially fatal Pulmonary Embolus (PE), is the most serious complication in all of these procedures after treatment of varicose veins [1-3]. Hilly, et al. pointed out that there is no consensus of the perioperative thrombosis prophylaxis after varicose veins laser ablation [4]. Clinical guidelines by the American ACCP, Scottish SIGN and Dutch CBO all recommend risk stratification after which only patients with risk factors for thrombosis are to be treated with prophylaxis. The most important risk factors are obesity and a history of VTE [5].
Aim of the Study
Comparison of the use of Caprini's Saphenous Ablation Scores versus Standard Caprini’s Score for the prophylaxis of VTE in EVLA.
Patients & Methods
60 patients admitted to Royal Vascular Center, Alexandria - Egypt. From Jan. 1st 2021 to June 30th 2021 divided in 3 groups. - Group A) Treated by ablation of Great saphenous vein and received VTE prophylaxis according to Caprini’s Saphenous Ablation Scores Figure 1 A &B -Group B) Treated by ablation of Great saphenous vein and received VTE prophylaxis according to Standard Caprini’s Risk Assessment Score for VTE Figure 2 C) Treated by ablation of Great saphenous vein without VTE prophylaxis Patients signed an informed consent [6,7]. The pre-operative assessment by venous Duplex Ultrasound to assess the incompetence of SFJ and DVT detection prior to intervention. Ablation was done using radial 1470 YAG laser fibers and Post-operative Duplex was done one day and one month.

Figure 1: A & B) Caprini’s Saphenous Ablation.
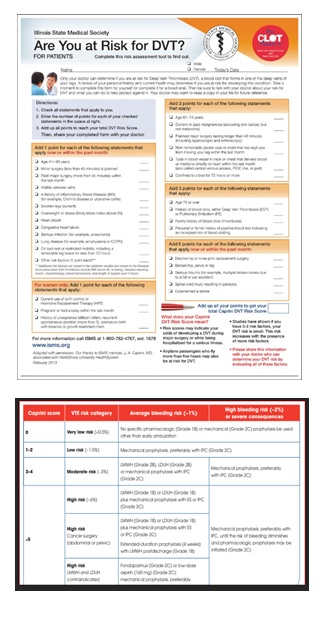 Figure 2: Standard Caprini's Risk Assessment.
Figure 2: Standard Caprini's Risk Assessment.
Inclusion Criteria
Patients with primary varicose veins with saphenofemoral junction incompetence with CEAP classification 2-6.
Exclusion Criteria
- Patients with history of DVT
- Patients with recurrent varicose veins
- Patients who are unable to provide an informed consent
- Pregnant patients at the time of the examination
Results
Age: 35.6+0.2, 34.3+0.5 and 37.6+0.09 years in the 3 groups M/F: 6/14, 8/12 and 7/13. In group A) all patients showed absent reflux post operatively and in all follow up visits .Dilated veins was noticed on the left side in 12 patients 60%, 2 patient on right and on 6 patients 30 % in Group (A), 14 patients 70%,one patient 5% and 5 patients 25% in Group (B) and 13 patients 65%,2 patients 10% and 5 patients 25% in Group (C), Table 1.
|
|
Left side |
Right side |
Both sides |
|
Group A |
12 patients 60% |
2 patients 10% |
6 patients 30% |
|
Group B |
14 patients 70% |
one patient 5% |
5 patients 25% |
|
Group C |
13 patients 65% |
2 patients 10% |
5 patients 25% |
Table 1: Side of varicose veins in the groups.
Clinical presentation according to CEAP Classification showed that:(2,8,9,0,1 patents) were C2,3,4,5,and 6 in Group A , ( 2,7,9,1,1 patents) were C2,3,4,5,and 6 in Group B and( 3,6,10,0,1 patents) were C2,3,4,5,and 6 in Group C. Duplex examination revealed significant reflux in the great saphenous veins in all patients and ranged from 0.7:0.9 Sec. and mean duration 0.7+0.09 Sec. Vein diameter ranged from (0.6: 0.9,X+0.76 CM.) in group A), (0.6: 0.8,X+0.7 CM.) in group B) , (0.5: 0.8,X+0.65 CM.) in group C) Table 2.
|
|
Group A |
Group B |
Group C |
|
GSV diameter |
Range:0.7:0.9 CM X 0.7+0.09 CM |
Range:0.7:0.9 CM X 0.7+0.09 CM |
Range:0.7:0.9 CM X 0.7+0.09 CM |
Table 2: Preoperative Duplex.
According to Caprini’s saphenous score 14 patients 70% were classified as low risk who used compression stockings only , 4 patients 20% were of moderate risk who received 40mg Enoxaparin /day for one week in addition to the stockings and 2 patients 10% of high-risk who received 40mg Enoxaparin /day for 28 days in addition to the stockings in Group A, while applying standard Caprini’s Score in group B patients revealed : 6 patients 30% were of moderate risk and 14 patients 70% of high risk in Group B ) Table 3.
|
|
Group A |
Group B |
|
Low risk |
14 patients 70% |
ZERO |
|
Moderate risk |
4 patients 20% |
6 patients 30% |
|
High risk |
2 patients 10% |
14 patients 70% |
Table 3: Risk assessment in Group A &B patients according to both risk assessment scores.
So, 14 patients 70% received Enoxaparin 40 mg / day for 7 days in group B patients, only 4 patients 20% received the same dose and duration ,with 2 patients 10% received the same dose for 28 days in group A patients. No VTE events were shown in both A&B, while 3 patients developed superficial thrombophlebitis 15% and one patient 5% developed left calf DVT in Group C, and the estimated Saphenous score was 11 and the standard score was 7 for these patients. Significant drop in VCSS in patients in the three groups, it dropped from 10.9 to 8.1, from 10.7 to 7.9 and 10.6 to 7.7 in group A, B and C. The time needed to complete total ablation of GSV ranged from 40:51.5, with a mean time 43.6+0.3, 44.3+0.9, 43.7 + 0.75 minutes the 3 groups.
So, 14 patients 70% received Enoxaparin 40 mg / day for 7 days in group B patients, only 4 patients 20% received the same dose and duration ,with 2 patients 10% received the same dose for 28 days in group A patients. No VTE events were shown in both A&B, while 3 patients developed superficial thrombophlebitis 15% and one patient 5% developed left calf DVT in Group C, and the estimated Saphenous score was 11 and the standard score was 7 for these patients. Significant drop in VCSS in patients in the three groups, it dropped from 10.9 to 8.1, from 10.7 to 7.9 and 10.6 to 7.7 in group A, B and C. The time needed to complete total ablation of GSV ranged from 40:51.5, with a mean time 43.6+0.3, 44.3+0.9, 43.7 + 0.75 minutes the 3 groups [8-10].
Conclusion
Risk assessment of patients undergoing varicose veins ablation should be done and applying Caprini’s saphenous score as a better alternative to Standard Caprini’s score for VTE prophylaxis and is considered a safe and cost-effective tool in VTE prevention in these patients.
Disclosure
The authors have no conflict of interest to declare.
Conflicts of Interest
The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
Funding
The authors report no involvement in the research by the sponsor that could had influenced the outcome of this work.
Acknowledgements
The authors acknowledge doctors and nursing staff in vascular surgery department of Alexandria Armed Forces hospital for proofreading activity.
References
- Marsh P, Price BA, Holdstock J, Harrison C, Whiteley MS (2010) Deep Vein Thrombosis (DVT) after Venous Thermoablation Techniques: Rates of Endovenous Heat-induced Thrombosis (EHIT) and Classical DVT after Radiofrequency and Endovenous Laser Ablation in a Single Centre. Eur J Vasc Endovasc Surg 40: 521-272.
- Testroote MJG, Wittens CHA (2013) Prevention of venous thromboembolism in patients undergoing surgical treatment of varicose veins. Phlebology 1: 86-90.
- Dexter D, Kabnick L, Berland T, Jacobowitz G, Lamparello P, et al. (2012) Complications of endovenous lasers. Phlebology 27: 40-45.
- Healy DA, Kimura S, Power D, Alhaj A, Abdeldaim Y, et al. (2018) A Systematic Review and Meta-analysis of Thrombotic Events Following Endovenous Thermal Ablation of the Great Saphenous Vein. Eur J Vasc Endovasc Surg 56: 410-424.
- Jacobs CE, Pinzon MM, Orozco J, Hunt PJB, Rivera A, et al. (2014) Deep venous thrombosis after saphenous endovenous radiofrequency ablation: Is it predictable? Ann Vasc Surg 28: 679-685.
- Caprini JA (2021) Thrombosis Prophylaxis in Varicose Vein Patients, Patient Evaluation and Degree of Risk. Presented online. Egyptian Venous Forum.
- Cronin MA, Dengler N, Krauss ES, Segal A, Wei N, et al. (2019) Completion of the Updated Caprini Risk Assessment Model (2013 Version). Clin Appl Thromb Hemost 25: 1-10.
- Mao J, Zhang C, Wang Z, Gan S, Ll K (2012) A retrospective study comparing endovenous laser ablation and microwave ablation for great saphenous varicose veins. Eur Rev Med Pharmacol Sci 16: 873-877.
- Shutze WP, Kane K, Hicks T, Kedora J, Hohmann S, et al. (2021) Bertram Smith Baylor University Medical Center, Dallas, TX . The Incidence and Outcome of DVT after Endovenous Laser Ablation.
- Enoch S, Woon E, Blair SD (2003) Thromboprophylaxis can be omitted in selected patients undergoing varicose vein surgery and hernia repair. Br J Surg 90: 818-820.
Citation: Caprini J, Fakhry A, Nagib S (2021) Validation of Caprini’s Saphenous Ablation Scores. J Angiol Vasc Surg 6: 082.
Copyright: © 2021 J Caprini, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.