Journal of Physical Medicine Rehabilitation & Disabilities Category: Medical
Type: Research Article
Wheelchair Tennis and Its Impact on People with Physical Disabilities
*Corresponding Author(s):
Zdravka LeutarDepartment Of Social Work, Law Faculty, University Of Zagreb, Croatia
Tel:+385 981865004,
Email:zleutar@pravo.hr
Received Date: Sep 23, 2016
Accepted Date: Jan 10, 2017
Published Date: Jan 24, 2017
Abstract
The first part of this paper presents a general definition of people with physical disabilities, their historical position in society, modern models of disability characterized by processes of integration with regard to sports persons with disabilities in general and, finally, it discusses tennis as practiced by people with disabilities in particular. The second part contains qualitative research designed to gain insight into the views and experiences of people in wheelchairs on practicing tennis as a sport activity for people with disabilities. The research study included 15 participants from 22 to 50 years of age. Data collection involved the use of a semi-structured interview, with qualitative analysis used in the data processing, while for the organization of the data collected the method of open coding was used. According to the results, the motives for involvement in this sport can be divided into intrinsic and extrinsic. Benefits to the life of players with disabilities are reflected at three levels: physical, psychological and social. Therefore, it seems reasonable to conclude that for people with physical disabilities who play tennis, the sport is an essential factor in their integration into society, as well as having a good effect on their mental and physical capabilities. It is important for society as a whole to invest more in the development of this sport and to continue conducting research on wheelchair tennis.
Keywords
People with physical disabilities; Tennis, Wheelchair tennis
INTRODUCTION
Perception of wheelchair tennis
People with disabilities are a part of every society. The number of people with disabilities in the world is large and still growing [1]. Estimates from the World Health Organization show that about 10% of the world population is affected by some type of injury that limits or changes their abilities in various areas of life [2]. Thus, the 2001 census showed that there are 429,421 persons with disabilities in Croatia, which is 9.7% of the total population of the country. With respect to sex, women are outnumbered in that group by the men, who make up 57.3% of the total number of persons with disabilities. But the fact is that in Croatia, on 13th December 2010, there were 529,103 people with disabilities, of which 316,557 were males (59.8%) and 212,546 females (40.2%). Therefore, people with disabilities make up about 11.9% of the total population of Croatia. The population studied in this research, i.e., people with physical impairments, makes up the largest percentage of people with disabilities-386,165 or 73% of the total number of people with disabilities in Croatia. The largest number of people with disabilities, 286,523 (54.2%), is of working age, from 19 to 64 years. However, disability is present in all age groups, including childhood, 0-19 years, where the figure is 7% [3].
Social policy towards people with disabilities has changed over time-from the possibility of the removal, elimination/killing or exposure of such children in ancient Greece and ancient Rome, through the expression of compassion for these people in the middle ages and the support of the great philosophers of empiricism and rationalism for people with disabilities, until the present policy of integration of people with disabilities in society. Living conditions, the social and economic policies of different periods, as well as social factors such as negligence, ignorance, superstition and fear that have historically slowed the progress of people with disabilities [1,4-6] are reflected in this variation in policy. Despite the fact that today this policy is developing more and more in a positive direction, in the direction of integration within society at large and equal opportunities for people with disabilities, in practice they still feel the effects of the negative attitudes of society towards them-they have higher unemployment rates, lower average earnings, lower participation in activities outside home, less possibility of using means of transport and a lower quality of life in general [7].
In the literature relating to this topic and in various legal and other documents, different definitions and concepts are used for people with disabilities. Some of the most commonly used are: invalidity, defectiveness, disabled, disability, people with disabilities, persons with impairment, physically and mentally handicapped persons, etc. The term disability, as one of the most frequently used, refers to “the different types and degrees of damage, difficulties or health problems (barriers) i.e., irregularities in the field of physical, mental, psychological or physical and social development” [8]. The World Health Organization in turn gives the international classification of impairments, disabilities and handicaps [9-11] in which disability is defined as any loss of or deviation from the normal psychological, physiological or anatomical structure or function. Disability is defined as any restriction or lack of ability to perform an activity in the manner or within the range that is considered normal for a human being. Handicap, on the other hand and according to this classification, is the lack that particular individuals suffer from, that which results from impairment or disability and restricts or disables them to fulfill their natural role in society. The latest version of the classification sees the functioning of an individual as a result of the interaction of physical or mental condition of a person with the social and physical environment, with the result that disability is seen as a consequence of a number of factors, not simply residing in the persons themselves [12].
Physical disability or impairment of motor skills is related to a wide range of different disturbances and irregularities of the body, which are sometimes expressed in the area of gross motor skills (involving larger movements of the body i.e., corpus and limbs), sometimes in the area of fine motor skills (involving smaller movements, such as gestures of the face or the hand or fingers) or in both areas. Disorders that interfere with motor skills may arise during the prenatal, perinatal or postnatal period, as well as in the later period of growth and development of a child, as a result of illness or trauma. Damage to the musculoskeletal system is an inherent or acquired reduction or loss of motor or functional abilities in the performance of certain activities. Topographic classification of motor disorders is defined by the number of limbs diagnosed with motor disorder [13].
Monoparesis is the motor weakness of one limb, and diparesis of two limbs. Paraparesis is a motor disorder of the lower extremities, triparesis is a motor disorder of three limbs, tetraparesis is a motor disorder in all four limbs. Complete tetraplegia results from injury above the sixth cervical (C6) segment and such a person is totally dependent on the help of another person. Hemiplegia is weakness of one half of the body. According to their severity, motor disorders are classified as easy, moderate and difficult. Pareses imply weakness of the limbs, where just slight motor function exists. Plegias are heavy motor disorders which may be related to changes on the skin, loss of sensation and loss of reflexes [13].
The authors Leutar and Štambuk [14] define physical disability from even more perspectives, such as the medical or etiological. People with physical disabilities resulting from certain types of damage, deformation, functional failure or interference caused by damage to the musculoskeletal system, to the central or peripheral nervous system or to chronic disease, regularly or occasionally require professional assistance in education and training for work and life under optimal conditions, tailored to the particular individual need.
The characteristics of sport for people with disabilities include:
• The aims of every person with disabilities are to achieve socialization, to be more equal with other members of society and to be better in a variety of skills
• Inclusion in sport is one of the possibilities for people with disabilities to be active and to express their talents and abilities
• Sport develops fun, fellowship - it thrills, encourages and helps gain confidence
• A small number of activities for people with disabilities require adaptation [15]
Tennis practiced by people with disabilities began to make progress at the first tournament of its kind, held in Los Angeles in 1977. Until then, it had been played only individually. After the tournament, people with disabilities started increasingly to promote this sport, on various occasions within hospitals and a little less often at tournaments. Tennis in a wheelchair then expanded to Europe (Netherlands, Germany, France etc.,). The International Wheelchair Tennis Foundation (IWTF) was founded in 1980, with the goal of organizing and promoting tennis in a wheelchair. Wheelchair tennis in Croatia began to develop in 1990 at the instigation of a few amateurs - enthusiasts. A more serious approach and development began only in 1996 after the involvement of professional staff, which was to increase the quality of training [16]. Wheelchair tennis today is among the most popular of sports played in wheelchairs. The reason is that a person in a wheelchair can play tennis with people without disabilities [17].
Vrdoljak [18] writes that in tennis, people with disabilities play by the same rules as people without disabilities-the rules specified by the international tennis federation-with just one difference: the ball can bounce twice before a person in a wheelchair returns it, and the ball can bounce on the ground just once before a person without disabilities returns it.
The tennis court for people with disabilities is identical to the standard court. The playing area is 23.77m long and 8.23m wide, the net hanging on a rope or metal rope with a diameter of at most 0.8cm, where the ends are attached to poles or transferred through two posts 1.07m high, the width not exceeding 15cm. The net has to be stretched to fill the space between the two posts, and must be thick enough to prevent the ball from passing through it. The net height in the middle is 0.914m, lower than at the sides of the court. The lines on the ground flanking the ends and sides of the court are called base lines and side lines. Service lines are drawn parallel with the net over a distance of 6.40m. The area between the service line and the side line is divided by a centre service line into two equal parts, and that area is called the service courts.
Immobility is the only criterion for participation in the competition in wheelchair tennis. As already stated, to participate in competition one must have partial or complete paralysis of one or more parts of the body, or lower-extremity amputations. Quadriplegic players are those with limited mobility, power and strength in at least three limbs due to an accident, spinal injury or other similar cause. To this group of players also belong walking quadriplegics, people who use electric powered wheelchairs or have undergone triple amputation. Players who cannot use both hands to move a wheelchair are allowed to use their legs. If there are doubts about eligibility to participate in wheelchair tennis competitions, the IWTF Committee on Rules has the ability to register any player who wants to be recognized .
There is a complete lack of research on the practice of tennis by people with disabilities in Croatia, which was the motivation for exploring the experiences of people with disabilities engaged in tennis. Qualitative methodology was used in order to cover this issue broadly and come to a clearer insight into participant responses to the research objective of this paper and the problems it identifies.
Social policy towards people with disabilities has changed over time-from the possibility of the removal, elimination/killing or exposure of such children in ancient Greece and ancient Rome, through the expression of compassion for these people in the middle ages and the support of the great philosophers of empiricism and rationalism for people with disabilities, until the present policy of integration of people with disabilities in society. Living conditions, the social and economic policies of different periods, as well as social factors such as negligence, ignorance, superstition and fear that have historically slowed the progress of people with disabilities [1,4-6] are reflected in this variation in policy. Despite the fact that today this policy is developing more and more in a positive direction, in the direction of integration within society at large and equal opportunities for people with disabilities, in practice they still feel the effects of the negative attitudes of society towards them-they have higher unemployment rates, lower average earnings, lower participation in activities outside home, less possibility of using means of transport and a lower quality of life in general [7].
In the literature relating to this topic and in various legal and other documents, different definitions and concepts are used for people with disabilities. Some of the most commonly used are: invalidity, defectiveness, disabled, disability, people with disabilities, persons with impairment, physically and mentally handicapped persons, etc. The term disability, as one of the most frequently used, refers to “the different types and degrees of damage, difficulties or health problems (barriers) i.e., irregularities in the field of physical, mental, psychological or physical and social development” [8]. The World Health Organization in turn gives the international classification of impairments, disabilities and handicaps [9-11] in which disability is defined as any loss of or deviation from the normal psychological, physiological or anatomical structure or function. Disability is defined as any restriction or lack of ability to perform an activity in the manner or within the range that is considered normal for a human being. Handicap, on the other hand and according to this classification, is the lack that particular individuals suffer from, that which results from impairment or disability and restricts or disables them to fulfill their natural role in society. The latest version of the classification sees the functioning of an individual as a result of the interaction of physical or mental condition of a person with the social and physical environment, with the result that disability is seen as a consequence of a number of factors, not simply residing in the persons themselves [12].
Physical disability or impairment of motor skills is related to a wide range of different disturbances and irregularities of the body, which are sometimes expressed in the area of gross motor skills (involving larger movements of the body i.e., corpus and limbs), sometimes in the area of fine motor skills (involving smaller movements, such as gestures of the face or the hand or fingers) or in both areas. Disorders that interfere with motor skills may arise during the prenatal, perinatal or postnatal period, as well as in the later period of growth and development of a child, as a result of illness or trauma. Damage to the musculoskeletal system is an inherent or acquired reduction or loss of motor or functional abilities in the performance of certain activities. Topographic classification of motor disorders is defined by the number of limbs diagnosed with motor disorder [13].
Monoparesis is the motor weakness of one limb, and diparesis of two limbs. Paraparesis is a motor disorder of the lower extremities, triparesis is a motor disorder of three limbs, tetraparesis is a motor disorder in all four limbs. Complete tetraplegia results from injury above the sixth cervical (C6) segment and such a person is totally dependent on the help of another person. Hemiplegia is weakness of one half of the body. According to their severity, motor disorders are classified as easy, moderate and difficult. Pareses imply weakness of the limbs, where just slight motor function exists. Plegias are heavy motor disorders which may be related to changes on the skin, loss of sensation and loss of reflexes [13].
The authors Leutar and Štambuk [14] define physical disability from even more perspectives, such as the medical or etiological. People with physical disabilities resulting from certain types of damage, deformation, functional failure or interference caused by damage to the musculoskeletal system, to the central or peripheral nervous system or to chronic disease, regularly or occasionally require professional assistance in education and training for work and life under optimal conditions, tailored to the particular individual need.
The characteristics of sport for people with disabilities include:
• The aims of every person with disabilities are to achieve socialization, to be more equal with other members of society and to be better in a variety of skills
• Inclusion in sport is one of the possibilities for people with disabilities to be active and to express their talents and abilities
• Sport develops fun, fellowship - it thrills, encourages and helps gain confidence
• A small number of activities for people with disabilities require adaptation [15]
Tennis practiced by people with disabilities began to make progress at the first tournament of its kind, held in Los Angeles in 1977. Until then, it had been played only individually. After the tournament, people with disabilities started increasingly to promote this sport, on various occasions within hospitals and a little less often at tournaments. Tennis in a wheelchair then expanded to Europe (Netherlands, Germany, France etc.,). The International Wheelchair Tennis Foundation (IWTF) was founded in 1980, with the goal of organizing and promoting tennis in a wheelchair. Wheelchair tennis in Croatia began to develop in 1990 at the instigation of a few amateurs - enthusiasts. A more serious approach and development began only in 1996 after the involvement of professional staff, which was to increase the quality of training [16]. Wheelchair tennis today is among the most popular of sports played in wheelchairs. The reason is that a person in a wheelchair can play tennis with people without disabilities [17].
Vrdoljak [18] writes that in tennis, people with disabilities play by the same rules as people without disabilities-the rules specified by the international tennis federation-with just one difference: the ball can bounce twice before a person in a wheelchair returns it, and the ball can bounce on the ground just once before a person without disabilities returns it.
The tennis court for people with disabilities is identical to the standard court. The playing area is 23.77m long and 8.23m wide, the net hanging on a rope or metal rope with a diameter of at most 0.8cm, where the ends are attached to poles or transferred through two posts 1.07m high, the width not exceeding 15cm. The net has to be stretched to fill the space between the two posts, and must be thick enough to prevent the ball from passing through it. The net height in the middle is 0.914m, lower than at the sides of the court. The lines on the ground flanking the ends and sides of the court are called base lines and side lines. Service lines are drawn parallel with the net over a distance of 6.40m. The area between the service line and the side line is divided by a centre service line into two equal parts, and that area is called the service courts.
Immobility is the only criterion for participation in the competition in wheelchair tennis. As already stated, to participate in competition one must have partial or complete paralysis of one or more parts of the body, or lower-extremity amputations. Quadriplegic players are those with limited mobility, power and strength in at least three limbs due to an accident, spinal injury or other similar cause. To this group of players also belong walking quadriplegics, people who use electric powered wheelchairs or have undergone triple amputation. Players who cannot use both hands to move a wheelchair are allowed to use their legs. If there are doubts about eligibility to participate in wheelchair tennis competitions, the IWTF Committee on Rules has the ability to register any player who wants to be recognized .
There is a complete lack of research on the practice of tennis by people with disabilities in Croatia, which was the motivation for exploring the experiences of people with disabilities engaged in tennis. Qualitative methodology was used in order to cover this issue broadly and come to a clearer insight into participant responses to the research objective of this paper and the problems it identifies.
METHODOLOGY
- Must not change position by moving or turning the wheelchair around. It shall not be held that the player who serves alters his position if there is a slight displacement of the wheel that does not significantly affect the initial position
- Should not touch even with one wheel any surface other than the one behind the baseline within the imaginary extension of the central mark and side lines
c. If a player deliberately uses the feet for braking or stabilization while serving, the service will be accounted a fault
d. If the usual methods of service are physically impossible for the player to perform owing to the player’s quadriplegic condition, then someone else can throw the ball for him
In tennis for people with disabilities, wheelchairs are considered to be a part of the body
The player loses the point:
a. If the ball in play touches a player, his wheelchair or something he carries or holds, except for the racket in his hand
b. If the service ball hits him, his wheelchair or something he carries or holds, except for the racket in his hand
c. If a player intentionally uses his feet or lower extremities for braking or stabilization while serving or to kick the ball, stop or turn
d. If a player at the moment of contact with the ball loses contact with the wheelchair.
The player does not lose the point if he returns the ball, then falls out of the wheelchair and returns to the wheelchair to retrieve the ball when it is returned to his court [19].
- Should not touch even with one wheel any surface other than the one behind the baseline within the imaginary extension of the central mark and side lines
c. If a player deliberately uses the feet for braking or stabilization while serving, the service will be accounted a fault
d. If the usual methods of service are physically impossible for the player to perform owing to the player’s quadriplegic condition, then someone else can throw the ball for him
In tennis for people with disabilities, wheelchairs are considered to be a part of the body
The player loses the point:
a. If the ball in play touches a player, his wheelchair or something he carries or holds, except for the racket in his hand
b. If the service ball hits him, his wheelchair or something he carries or holds, except for the racket in his hand
c. If a player intentionally uses his feet or lower extremities for braking or stabilization while serving or to kick the ball, stop or turn
d. If a player at the moment of contact with the ball loses contact with the wheelchair.
The player does not lose the point if he returns the ball, then falls out of the wheelchair and returns to the wheelchair to retrieve the ball when it is returned to his court [19].
Design
Data were collected by semi-structured interview. The interview consisted of questions related to various general characteristics, such as age, sex or marital status, and questions based on the pursuit of tennis advantage, problems and prospects for the future. The interview consisted of a total of five questions. Interviews were conducted by the authors of this paper. We found the participants with help of the Croatian association of wheelchair tennis, which provided information about the club where people with physical disabilities train. Before the research, the researchers explained to research participants the aim of the research, requested voluntary consent to participate in the research and informed participants about anonymity and confidentiality of the shared information. It was emphasized to each participant that his responses would be combined with the responses of other participants in order to analyze the phenomenon itself, because there could be no accurate nor incorrect answers, only their subjective assessment of the subject. The average duration of the interview was 30 minutes. The questions were open-ended, for example: “What do you think of wheelchair tennis?” Most of the interviews were recorded with a voice recorder and by written notes. One participant sent a reply by e-mail for legitimate reasons. Participants were told that they would be informed of the research results after the research was completed and the data processed.
One example of a statement on wheelchair tennis made by a participant in an interview: “I would personally recommend practicing tennis to any person with disabilities, because it helps in all respects and the benefits of the court can be ‘replicated’ in daily life”.
One example of a statement on wheelchair tennis made by a participant in an interview: “I would personally recommend practicing tennis to any person with disabilities, because it helps in all respects and the benefits of the court can be ‘replicated’ in daily life”.
Ethical implications
At the beginning of the interview, it was explained to the participants that the interview would be recorded. Each research participant was guaranteed confidentiality. Participants were informed that at any moment they could drop all discussion and have the right not to answer further questions if they so desired. At the end of each interview, each participant was asked if he/she wanted to say anything else and how he/she felt after the conversation. Each interview was recorded using a dictaphone after the verbal consent of research participants had been obtained.
Participants
The data for the survey were collected and the research was carried out, as already mentioned, with the Croatian association of wheelchair tennis players. The study included 15 participants in Zagreb, Croatia in summer 2014. It was not a random sample because the population selected for interviewing was exclusively made up of people with disabilities engaged in tennis. All 15 participants were male. The age of participants ranged from 22-50 years of age. Most often they had finished high school and one person had finished college. Some participants were disabled in the homeland war of the 1990s, while most persons with paraplegia had been so affected since their childhood.
Data processing
To process the data, the process of qualitative analysis was used and for the organization of the collected data the method of thematic analysis was used. Thematic analysis can be an essentialist or realist method, which reports experiences, meanings and the reality of participants, or it can be a constructionist method, which examines the ways in which events, realities, meanings, experiences and so on are the effects of a range of discourses operating within society [20]. In accordance with this method, the first step in the processing of data was the editing of empirical material by marking sentences and parts of sentences that were significant with regard to the above research questions, which was done in order to define the so-called codes of the first order. After that, the procedure of combining related terms into categories was conducted, whereby each code of the first order was associated with the relevant term at the second order and in that way the essence of each unit of text was emphasized. The last step was the assignment of related terms to categories, which was followed by their analysis (Table 1 and Table 2).
Table 1: Data processing.
| No | Statements made by people with disabilities on the usefulness of practicing tennis | Code |
| 1 | Tennis to me is a real lifeline for my life. It is particularly beneficial to my health. It is very important that people with disabilities are involved in sports. In that way, they feel better and it gives us security. I would recommend that all sportsmen to practice their desired sport | - Tennis as lifeline |
| - Beneficial to health | ||
| - Better feeling | ||
| - Gives security | ||
| - Recommendation that people with disabilities practice their desired sport | ||
| 2 | First, I would recommend any sport because it’s great for us, but of course I would also recommend tennis in particular. We sweat a lot, we are active, it is good for health, we occupy our free time. And if you’re not into sports, you get fat. I play tennis to sweat and enjoy myself, to socialize (5). | - Physical activity |
| - Constructively occupied free time | ||
| - Socializing |
| Interview | Subtheme | Theme |
| Tennis to me is a real lifeline for my life. It is particularly beneficial to my health. It is very important that people with disabilities are involved in sports. In that way, they feel better and it gives us security. | - Beneficial to health | Benefits of practicing tennis for people with disabilities |
| - Feeling of usefulness and satisfaction | ||
| I would recommend that all sportsmen practice their desired sport (2). | ||
| First, I would recommend any sport because it’s great for us, but of course I would also recommend tennis in particular. We sweat a lot, we are active, it is good for health, we occupy our free time. And if you’re not into sports, you get fat. I play tennis to sweat and enjoy myself, to socialize (5). | - Constructive occupied free time | |
| - Socializing |
Benefits of practicing tennis for people with disabilities
Physical activity is an important and indispensable component of life that satisfies man’s primary need for movement, which especially in the open air has additional effects: it increases the overall level of activation of all physiological functions and resources of the organism, speeds up the elimination of harmful substances from the body by e.g., breathing, accelerating metabolism and the like [21].
The analysis of empirical data shows that participants see benefit as achieved through the following elements.
The analysis of empirical data shows that participants see benefit as achieved through the following elements.
Good for health
Tennis to me is a real lifeline for my life. It is particularly beneficial to my health... (2)
...it is good for health... (5)
We sweat a lot, we are active... (5)
And if you’re not into sports, you get fat. I play tennis to sweat and enjoy myself… (5)
...it is good for health... (5)
We sweat a lot, we are active... (5)
And if you’re not into sports, you get fat. I play tennis to sweat and enjoy myself… (5)
Feeling of satisfaction and safety
In that way, they feel better and it gives us security... (2)
Constructively occupied free time
…we occupy our free time... (5)
Socializing
…to socialize (5)
RESULTS AND DISCUSSION
Thematic map 1 (Figure1)
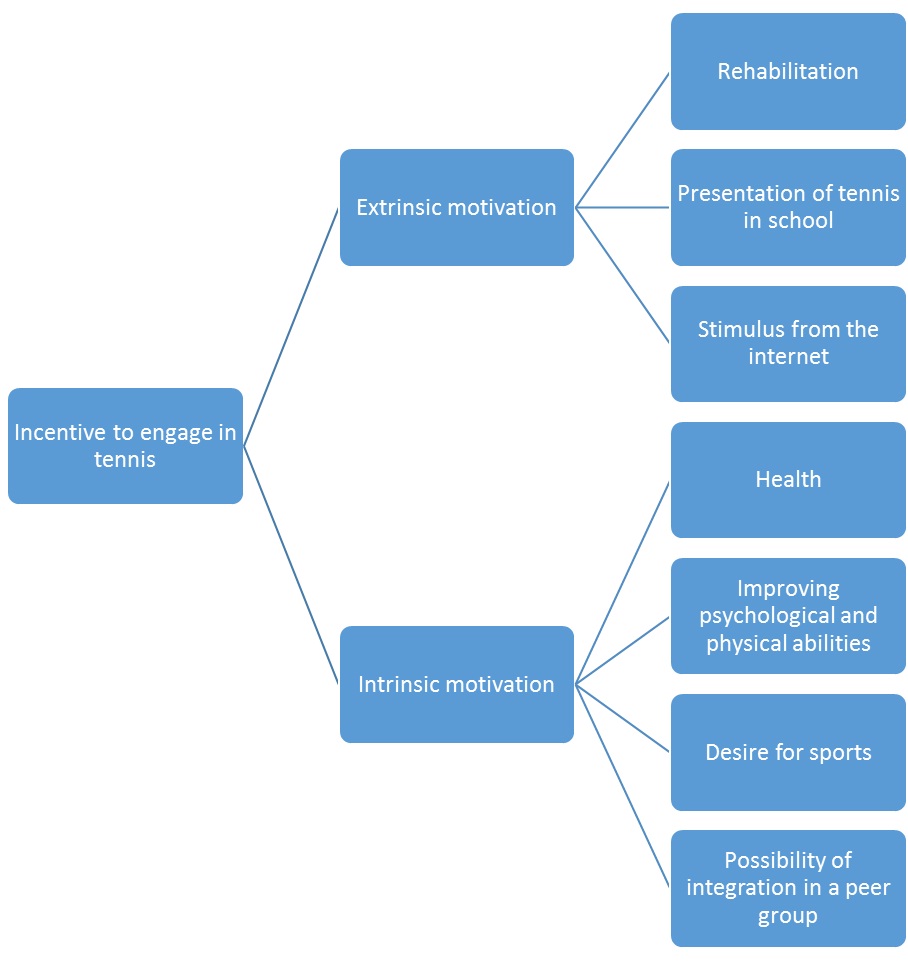
Motivational factors influencing participation in tennis
Motivation means behavior that incites an organism to be active, directs the activity in a particular direction and regulates the duration of the activity; this behavior can be triggered by some internal (intrinsic) motive such as need or desire, or some external (extrinsic) motive [22]. The question about motivation for involvement in tennis was included in order to find out which were the enabling factors in the life of respondents that influenced the selection of tennis and inclusion in the active practice of tennis.
In the field of sports and recreational activities, intrinsic motivation is the kind of motivation where the need has arisen from internal motives, such as the need for exercise and health or for a beautiful and healthy appearance, and satisfaction is derived from the very activity and/or its meaning [23]. Intrinsic motivation for some sport reflects the primary interest in, or the need for, that particular activity, and the activity itself constitutes a reward, a sense of fulfillment, the reaching of a goal, the completion of a motivational cycle [23]. When participation in a sporting activity is controlled by external reasons as, for example, the desire for a trophy, we talk about extrinsic motivation [22]. It is generally believed that sportsmen are simultaneously driven by both intrinsic and extrinsic reasons, only the relation of the two is not the same in all cases. However, it is considered that intrinsically-motivated sportsmen generally persist longer in the activities than extrinsically-motivated sportsmen because the reasons for external activity cease to exist by achieving an external goal [24].
The analysis of the responses resulted in the establishment of two categories of motivational source: personal motivation and incentives from the environment.
In the field of sports and recreational activities, intrinsic motivation is the kind of motivation where the need has arisen from internal motives, such as the need for exercise and health or for a beautiful and healthy appearance, and satisfaction is derived from the very activity and/or its meaning [23]. Intrinsic motivation for some sport reflects the primary interest in, or the need for, that particular activity, and the activity itself constitutes a reward, a sense of fulfillment, the reaching of a goal, the completion of a motivational cycle [23]. When participation in a sporting activity is controlled by external reasons as, for example, the desire for a trophy, we talk about extrinsic motivation [22]. It is generally believed that sportsmen are simultaneously driven by both intrinsic and extrinsic reasons, only the relation of the two is not the same in all cases. However, it is considered that intrinsically-motivated sportsmen generally persist longer in the activities than extrinsically-motivated sportsmen because the reasons for external activity cease to exist by achieving an external goal [24].
The analysis of the responses resulted in the establishment of two categories of motivational source: personal motivation and incentives from the environment.
Personal motivation
Participants cited intrinsic motives that prompted them to engage in the practice of tennis. Some of them noted that it was particularly useful for their state of health (...I wanted to play tennis, primarily because of health... (2) ...I suffer from severe pain and sports do me good-good to my health (2)). Ciliga et al., [25] note that the modern way of life, in addition to the many positive aspects to its effect on man and the quality of his life, also has a negative impact on his mental and physical status. They state that the research results of a number of authors dealing with the significance of physical exercise indicated that playing sports helps an individual today to preserve and improve health and eliminate the negative effects. It is believed that each person should and must engage in physical activity in order to function better in today’s modern society with all its features. Some of the participants clearly stated this belief/attitude (...I wanted to improve my mental and physical abilities (1)). As we see, people with disabilities want, through engagement in tennis, to improve their mental and physical abilities and that is their intrinsic motivation. The other aspect of intrinsic motivation that participants cited is a simple desire to play tennis because this form of sport is simply the one they want. (...sport was always my desire... I also play basketball, but I like tennis very much (5)). Here we see that disability as such does not have a decisive role, but the inner motivation does i.e., the desire for playing sports had existed before the occurrence of disability, and continued after the occurrence of disability.
Extrinsic motivation or incentives from the environment
The inclusion of people with disabilities in activities related to kinesiology is a prerequisite for their best possible adjustment. Kinesiological activities are those that mitigate the changes in behavior that almost always occur after the occurrence of disability [26]. This is why the practice of tennis is presented in rehabilitation centers, schools, etc. It is very important that people with disabilities become familiar with the opportunities offered to them because they are often not interested and think that everything is beyond their capabilities [27]. By watching the practice of wheelchair tennis in their environment, people with disabilities come to the realization that it appears to be useful for their personal well-being (...I was introduced to tennis at the time of rehabilitation in the spa (2) or in my school there was a presentation of tennis in a wheelchair and I was then encouraged to play sports... helps my health... I really like that sport (4)). Some of the sportsmen realized that they can actually socialize in tennis and achieve the same results as healthy people (...with my friends who are healthy I started playing tennis, then I found out about it and so started playing tennis (5)). Peer groups and friends of children with disabilities and grown-ups with disabilities are also important sources of motivation for practicing tennis. That is very important for the integration and social inclusion of people with disabilities, and affects the formation of positive attitudes towards people with disabilities. Negative attitudes and prejudices contribute to the social exclusion of people with disabilities, their isolation and difficulties in accessing community resources [28].
Benefits of practicing tennis for people with disabilities
The analysis of the interviews resulted in three categories of benefits of practicing tennis by people with disabilities:
Thematic map 2 (Figure 2)
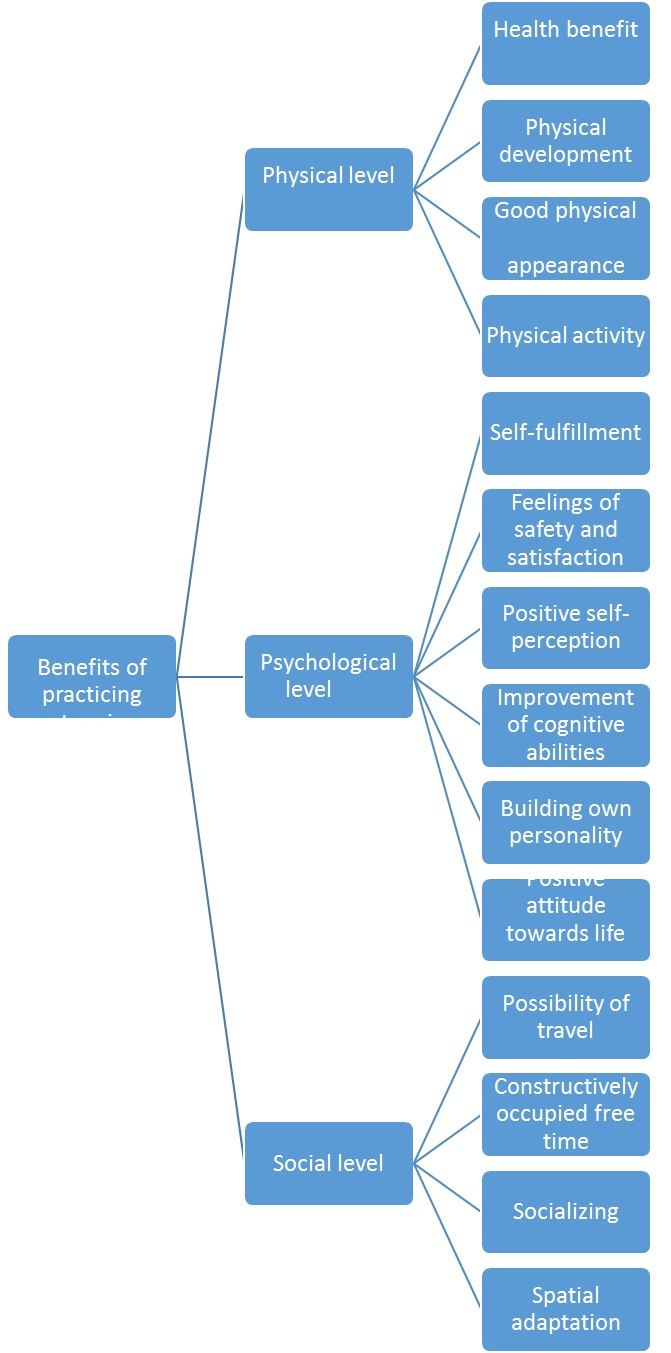
Benefits on the physical level
The World Health Organization as an organization under the umbrella of the United Nations acts as a coordinating body of international public health, and has a great role in promoting physical activity. On 10th May 2002 [29], the United Nations launched a global initiative to mark the International Day of Physical Activity as a continuation of World Health Day, which was given the theme of “Physical Activity for Health” (“Agita Mundo-Move for Health”) to raise awareness throughout the whole world of the importance of regular physical activity in maintaining and improving health and well-being. Since then, that day has continued to be marked every year by the Member States around the world. Daily physical activity of moderate intensity is recommended, lasting 30 minutes for adults and at least 60 minutes for children and young persons [29-31]. Our participants stated the importance of exercising through tennis for the physical development of people with disabilities (...when I started to practice tennis I was underdeveloped, and now I see that I am much better developed... (4) ...I got quite strong (4)). Participants just emphasize how important physical activity is, and how practicing tennis has a good impact on their physical appearance (And if you’re not into sports, you get fat. I play tennis to sweat (5) ...I know a lot of people who do not do sports, so they put on weight (4)). So, the participants regularly stress the importance of physical activity (First i would recommend... tennis, we sweat a lot, and we are active (5)).
The importance of regular physical activity in primary and secondary prevention of chronic diseases such as diabetes, obesity, osteoporosis and cardiovascular disease has been particularly emphasized [32], as has its contribution to mental health and better internal and external balance, which enhances the psychosocial status of man because prevention is better than cure [33]. Comments to this effect from participants in this study are notable: usefulness for health (In a special way it is useful (to practice tennis) for my health... (2) ...and for the health... (5)).
The importance of regular physical activity in primary and secondary prevention of chronic diseases such as diabetes, obesity, osteoporosis and cardiovascular disease has been particularly emphasized [32], as has its contribution to mental health and better internal and external balance, which enhances the psychosocial status of man because prevention is better than cure [33]. Comments to this effect from participants in this study are notable: usefulness for health (In a special way it is useful (to practice tennis) for my health... (2) ...and for the health... (5)).
Benefits on the psychological level
By participating in physical activity, an individual effect a positive change on a psychological level, which contributes to the development of a positive ‘self-concept’ [34,35]. The concept of self is called by Susan Harter [36] calls this a multidimensional construct in which the individual may have different perceptions of his competence, and simple participation in tennis activities for tennis players contributes to creating a sense of their own competence in that area.
Understanding the concept of self-perception, with respect to an individual’s lifetime, has changed over the years. Many theorists engaged in the development of this concept used to speak only about those aspects which they considered to be essential in a particular period of life. Yet a few authors who focused on development throughout life have greatly influenced the modern concept of the development of self-perception. Today it is considered to be not innate, but acquired and developed throughout life. It unfolds on the principle of the concrete, contains physical attributes approaching the abstract, and contains psychological attributes [37]. Thus, participants in our research point out (...with tennis I want to show that we, the disabled, are not “weaklings”, but can be stronger fighters than some “healthy persons” (1)), which actually points to positive self-perception. Participants also pointed out that practicing tennis gives them a sense of security and satisfaction (...I would recommend that all sportsmen practice their desired sport (3); In this way, we feel better and it gives us security... (2)) and it is very important that people with disabilities, through engagement in tennis, feel a sense of personal fulfillment (It is very important that people with disabilities practice their desired sport (2)). Petz [38] defines emotions as experiences caused by an external or internal situation, characterized primarily by the fact that they are mostly pleasant or unpleasant, and sometimes ambivalent. Man daily perceives the world that surrounds him, reacts positively to what is around him or does not, and acts accordingly. In addition to the enhanced emotional feelings that result from practicing tennis, participants themselves point to the improvement of cognitive abilities (...you have to be at a high level of concentration, which helps a lot (1)). Furthermore, practicing tennis impacts on the construction of one’s own personality according to the statements of participants (...patience... hard work ... tennis can be ‘replicated’ from the court to daily life (1)). Practicing tennis participants also see it as an opportunity for positive attitudes towards life, without whining over the past (...you have no time to think about things, worry about the past... (3) Tennis...presents my lifeline (2)). Tennis, for tennis players, is evidently an important component of their emotional health because by participation in tennis activities they feel happiness, pleasure and enjoyment and it helps them to develop a positive approach to life.
Understanding the concept of self-perception, with respect to an individual’s lifetime, has changed over the years. Many theorists engaged in the development of this concept used to speak only about those aspects which they considered to be essential in a particular period of life. Yet a few authors who focused on development throughout life have greatly influenced the modern concept of the development of self-perception. Today it is considered to be not innate, but acquired and developed throughout life. It unfolds on the principle of the concrete, contains physical attributes approaching the abstract, and contains psychological attributes [37]. Thus, participants in our research point out (...with tennis I want to show that we, the disabled, are not “weaklings”, but can be stronger fighters than some “healthy persons” (1)), which actually points to positive self-perception. Participants also pointed out that practicing tennis gives them a sense of security and satisfaction (...I would recommend that all sportsmen practice their desired sport (3); In this way, we feel better and it gives us security... (2)) and it is very important that people with disabilities, through engagement in tennis, feel a sense of personal fulfillment (It is very important that people with disabilities practice their desired sport (2)). Petz [38] defines emotions as experiences caused by an external or internal situation, characterized primarily by the fact that they are mostly pleasant or unpleasant, and sometimes ambivalent. Man daily perceives the world that surrounds him, reacts positively to what is around him or does not, and acts accordingly. In addition to the enhanced emotional feelings that result from practicing tennis, participants themselves point to the improvement of cognitive abilities (...you have to be at a high level of concentration, which helps a lot (1)). Furthermore, practicing tennis impacts on the construction of one’s own personality according to the statements of participants (...patience... hard work ... tennis can be ‘replicated’ from the court to daily life (1)). Practicing tennis participants also see it as an opportunity for positive attitudes towards life, without whining over the past (...you have no time to think about things, worry about the past... (3) Tennis...presents my lifeline (2)). Tennis, for tennis players, is evidently an important component of their emotional health because by participation in tennis activities they feel happiness, pleasure and enjoyment and it helps them to develop a positive approach to life.
Benefits of practicing tennis on the social level
Sport is not possible without free time, where sport is not a man’s professional activity [39]. Thus today, in the field of sports, we note several sports systems [40]:
• Professional sport, where sport appears as a profession or the main occupation of participants
• Amateur sport that is typically of a lower quality, in which participants usually satisfy their basic human needs and seek to preserve or improve their physical and mental health
• School sport that is characterized by a well-developed system of selection, with a system of training from young age and a competitive system
• Recreational sport in which a company provides appropriate facilities and personnel, and program participants generally participate in the cost of implementing an exercise program
Many sports for people with disabilities, in which people with physical and mental disabilities participate, are based on existing sports, and are adapted to the needs of people with disabilities, so they are known as “adapted or customized sports”. “Adaptation refers to the movement, physical and sports activity” [41]. There are also, none the less, sports for people with disabilities that are not a version of an existing sport but are specially “designed” for people with disabilities.
Physical activity and sports are an important part of free time today as is shown by a study carried out in Denmark, according to which one of the main modern leisure activities is playing sports [42]. However, according to the results of a study conducted in Pula, Croatia, girls of 18 (graduation grade) use only 10% of their free time for sports or other recreational activities [43]. Our participants indicated that tennis enables them to constructively occupy their free time (... occupy our leisure time... (5)). Playing tennis always includes a social element as well - socializing (...we socialize a lot... (5)) and possibility of travel (...you travel around the world. I’ve been to the whole world and all continents (3)). To be able to experience those benefits, spatial adaptation of the courts for people with disabilities is necessary (...here access to the courts is well adapted to meet our needs. We have also an adapted toilet, which is very important... (5)). The importance of ensuring that infrastructure and facilities are accessible to people with disabilities will become more evident below: physical barriers in particular affect practicing tennis for people with disabilities and can present substantial obstacles for them.
• Professional sport, where sport appears as a profession or the main occupation of participants
• Amateur sport that is typically of a lower quality, in which participants usually satisfy their basic human needs and seek to preserve or improve their physical and mental health
• School sport that is characterized by a well-developed system of selection, with a system of training from young age and a competitive system
• Recreational sport in which a company provides appropriate facilities and personnel, and program participants generally participate in the cost of implementing an exercise program
Many sports for people with disabilities, in which people with physical and mental disabilities participate, are based on existing sports, and are adapted to the needs of people with disabilities, so they are known as “adapted or customized sports”. “Adaptation refers to the movement, physical and sports activity” [41]. There are also, none the less, sports for people with disabilities that are not a version of an existing sport but are specially “designed” for people with disabilities.
Physical activity and sports are an important part of free time today as is shown by a study carried out in Denmark, according to which one of the main modern leisure activities is playing sports [42]. However, according to the results of a study conducted in Pula, Croatia, girls of 18 (graduation grade) use only 10% of their free time for sports or other recreational activities [43]. Our participants indicated that tennis enables them to constructively occupy their free time (... occupy our leisure time... (5)). Playing tennis always includes a social element as well - socializing (...we socialize a lot... (5)) and possibility of travel (...you travel around the world. I’ve been to the whole world and all continents (3)). To be able to experience those benefits, spatial adaptation of the courts for people with disabilities is necessary (...here access to the courts is well adapted to meet our needs. We have also an adapted toilet, which is very important... (5)). The importance of ensuring that infrastructure and facilities are accessible to people with disabilities will become more evident below: physical barriers in particular affect practicing tennis for people with disabilities and can present substantial obstacles for them.
CONCLUSION
Tennis played by people with disabilities in Croatia is a sport in development and it includes people with disabilities from the Homeland War and civil persons with disabilities. Motives for inclusion in this sport can be divided into intrinsic and extrinsic. Intrinsic motives are affected by the health of people with disabilities, improving psychological and physical abilities, the desire to practice sport and the need for integration into a peer group. As extrinsic motives it is possible to identify environmental influences: rehabilitation facilities, the presentation of tennis in schools and incentives from the internet.
The benefits that accrue to tennis players with disabilities are reflected at three levels: physical, psychological and social. On the physical level the benefits of tennis are as follows: usefulness for health, better physical development, contribution to a better physical appearance and better physical activity. On the psychological level it contributes to the fulfillment of the desire for sports, contributes to a positive self-concept, gives a sense of security and satisfaction, improves cognitive skills, contributes to the building of the personality and contributes to a positive view of life. At the social level, tennis provides constructive engagement in the individual’s free time, socializing, and the possibility of travel and, which is important for all other benefits, good and well-adapted infrastructure.
This study is the first one conducted in Croatia and could be a starting point for further research on a larger sample which could combine both qualitative and quantitative methodologies to investigate this area. The results of this research have clearly shown, in practical and theoretical terms, the potential for improving the quality of life for tennis players with disabilities.
The benefits that accrue to tennis players with disabilities are reflected at three levels: physical, psychological and social. On the physical level the benefits of tennis are as follows: usefulness for health, better physical development, contribution to a better physical appearance and better physical activity. On the psychological level it contributes to the fulfillment of the desire for sports, contributes to a positive self-concept, gives a sense of security and satisfaction, improves cognitive skills, contributes to the building of the personality and contributes to a positive view of life. At the social level, tennis provides constructive engagement in the individual’s free time, socializing, and the possibility of travel and, which is important for all other benefits, good and well-adapted infrastructure.
This study is the first one conducted in Croatia and could be a starting point for further research on a larger sample which could combine both qualitative and quantitative methodologies to investigate this area. The results of this research have clearly shown, in practical and theoretical terms, the potential for improving the quality of life for tennis players with disabilities.
REFERENCES
- Standardna pravila o izjedna?avanju mogu?nosti za osobe s invaliditetom (1999) Zagreb: Državni zavod za zaštitu obitelji, materinstva i mladeži.
- Buljevac M, Majdak M, Leutar Z (2012) The stigma of disability: Croatian experiences. Disabil Rehabil 34: 725-732.
- Benjak T (2011) Izvješ?e o osobama s invaliditetom u Republici Hrvatskoj. Zagreb: Hrvatski zavod za javno zdravstvo, Služba za epidemiologiju kroni?nih masovnih bolesti.
- Preambula (2007) Konvencija o pravima osoba s invaliditetom. Države potpisnice ove Konvencije.
- Nacionalna strategija jedinstvene politike za osobe s invaliditetom od 2003. do 2006. godine. Narodne Novine 13/2003.
- Nacionalna strategija izjedna?avanja mogu?nosti za osobe s invaliditetom od 2007. do 2015. godine. Narodne Novine.
- Leutar Z, Hlupi? S, Vladi? J, ?aljkuši? M (2015) Metode socijalnog rada s osobama s invaliditetom, Pravni Fakultet, Sveu?ilišta u Zagrebu.
- Leutar Z, Buljevac M, Mili? Babi? M (2011) Socijalni položaj osoba s invaliditetom u Hrvatskoj. Zagreb: Ministarstvo obitelji, branitelja i me?ugeneracijske solidarnosti.
- World health organization (1986) International Classification of Impairments, Disabilities and Handicaps. Release Institute of Public Health Croatian.
- World health organization (2001) Interanacional classification of Functioning, Disability and Health (ICF). World health organization, Geneva, Switzerland.
- World Health Organization (2007) International Classification of Functioning, Disability and Health - Children and Youth Version. ICF-CY. World Health Organization, Geneva, Switzerland.
- Mihanovi? V (2011) Invaliditet u kontekstu socijalnog modela. Hrvatska revija za rehabilitacijska istraživanja 47: 72-86.
- Leutar Z (2008) Internal script Zagreb Law Faculty, Department of Social Work.
- Leutar Z, Štambuk A (2007) Invaliditet u obitelji i izvori podrške. Hrvatska revija za rehabilitacijska istraživanja 43: 47-61.
- Petrinovi?-Zekan L, Ciliga D, Trkulja-Petkovi? D (2011) Research on sport activity in persons with disability in Croatia. Proceedings Book: 6th International Conference on Kinesiology: Integrative Power of Kinesiology, Opatija, Croatia, September 08-11, 2011.
- Lugonji? S (2011) Sport osoba s invaliditetom (Graduate Thesis). Studijski centar socijalnog rada Pravnog fakulteta Sveu?ilišta u Zagrebu.
- Diaper NJ, Goosey-Tolfrey VL (2009) A physiological case study of a paralympic wheelchair tennis player: reflective practise. Journal of Sports Science and Medicine 8: 300-307.
- Vrdoljak J (2013) Tenis u invalidskim kolicima i njegov utjecaj na osobe s invaliditetom. Zagreb: Kineziološki fakultet Sveu?ilišta u Zagrebu.
- Gilbert B, Jamison S (1994) Winning Ugly: Mental Warfare in Tennis -- Lessons from a Master. Simon and Schuster, New York, USA.
- Braun V, Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3: 77-101.
- Lepan Ž, Leutar Z (2012) Važnost tjelesne aktivnosti u starijoj životnoj dobi. Socijalna ekologija 21: 203-223.
- Beck RC (2003) Motivacija. Teorija i na?ela. Jastrebarsko: Naklada Slap, Croatia.
- Novak I (2006) Sportski marketing i industrija sporta. Knjižnica i ?itaonica ?Fran Galovi?? Koprivnica.
- Milanovi? D (1997) Priru?nik za sportske trenere. Zagreb: Fakultet za fizi?ku kulturu.
- Ciliga D, Trkulja-Petkovi? D, Delibaši? Z (2006) Kvaliteta rada u podru?ju sportske rekreacije osoba s invaliditetom. Stru?ni Radovi Unutar Teme. Pg No: 282-285.
- Trkulja Petkovi? D (1996) Prilog boljem razumijevanju stresa invalidnih osoba. Sport za sve, XIV 96: 29-31.
- Leutar Z, Ogresta J, Mili? Babi? M (2008) Obitelji osoba s invaliditetom i mreže podrške. Zagreb: Pravni fakultet Sveu?ilišta u Zagrebu, Croatia.
- Najman Hižman E, Leutar Z, Kancijan S (2008) Stavovi gra?ana prema osobama s invaliditetom u Hrvatskoj u usporedbi s Europskom unijom. Socijalna ekologija: ?asopis za ekološku misao i sociologijska istraživanja okoline 17: 71-93.
- World health organization (2002) The world health report 2002 - Reducing Risks, Promoting Healthy Life. World health organization, Geneva, Switzerland.
- World health organization (2007) Steps to health: A European framework to promote physical activity and health. World health organization, WHO Regional Office for Europe, Copenhagen, Denmark.
- Filip?i? T, Filip?i? A (2009) Time characteristics in wheelchair tennis played on hard surfaces. Kinesiology 41: 67-75.
- Warburton DE, Nicol CW, Bredin SS (2006) Health benefits of physical activity: the evidence. CMAJ 174: 801-809.
- Declaration and recommendations of the World Forum on Physical Activity and Sport (1995) Quebec, UNESCO.
- Bungi? M, Bari? R (2009) Physical Training and Some Aspects of Psychological Health. Croatian Sports Medicine Journal 24: 65-75.
- Valesco JV, Fuentes JP (2015) Rewiew of sport science research specialized on wheelchair tennis. 65: 14-15.
- Brajša-Žganec A, Raboteg-Šari? Z, Franc R (2000) Dimensions self-concept of children against perceived social support from different sources. Social research journal for general social issues 6: 897-912.
- Lackovi?-Grgin K (1994) Samopoimanje mladih. Jastrebarsko: Naklada Slap.
- Petz B (2005) Psihologijski rije?nik, Naklada Slap.
- Probert A, Crespo M (2015) Sociology of tennis: research on socialisation, participation and retirement of tennis players, ITF Choaching and Sport Science Review 65: 19-20.
- Milanovi? (2006) Teorijske osnove sporta i sportskog treninga. In: Heimer S, Medicina sporta. Zagreb: Kineziološki fakultet sveu?ilišta u Zagrebu Pg no: 45-98.
- Ciliga D, Trkulja-Petkovi? D (2000) Prilago?ene tjelesne aktivnosti djeci s invaliditetom. In: M. Andrijaševi? (eds.). Zbornik radova Znanstveno-stru?nog savjetovanja “Slobodno vrijeme i igra”. Zagreb: Fakultet za fizi?ku kulturu Sveu?ilišta u Zagrebu; 24-26. Pg No: 155-157.
- Je?ud I, Novak T (2005) Leisure Time of Children and young people with behavioral problems: Qualitative / Ivana Je?ud, Tihana Novak. Sociological: Journal Croatian Sociological Society 37: 77-90.
- Vrbanac D (2000) Struktura djelatnosti u slobodnom vremenu u?enica gimnazije Pula. In: Andrijaševi? M (eds.). Zbornik radova Znanstveno-stru?nog savjetovanja “Slobodno vrijeme i igra”. Zagreb: Fakultet za fizi?ku kulturu Sveu?ilišta u Zagrebu; 24-26. Pg No: 97-100.
Citation: Leutar I, Vrdoljak J, Leutar Z (2017) Wheelchair Tennis and Its Impact on People with Physical Disabilities. J Phys Med Rehabil Disabil 3: 015.
Copyright: © 2017 Ivan Leutar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Journal Highlights
© 2026, Copyrights Herald Scholarly Open Access. All Rights Reserved!