WISH-Type Hip Brace for Patients with Osteoarthritis of the Hip
*Corresponding Author(s):
Hideomi WatanabeDean, Faculty Of Health Care, Takasaki University Of Health And Welfare, Takasaki, Gunma, Japan
Tel:+81 81273521291,
Fax:81273521985
Email:watanabe-h@takasaki-u.ac.jp
Abstract
We developed a user-friendly WISH-type hip brace that reinforces the hip joint by preventing up- and outward movement of the femoral head. This brace increased the strength of steps, provided propulsion enhancement, and augmented postural control to increase maximum excursion. These direct effects improved hip function scores, especially for pain scores. Functional mobility analysis revealed that the brace supports the hip during external and/or abduction movements in turning to the sound leg side. The brace augments the effects of muscle power around the affected hip. A short-term longitudinal study showed improvement in the abduction muscle strength of the affected limb with little interaction with the sound limb. There are so far few side effects of the WISH-type hip brace; thus, it is a suitable intervention for aged patients with complications of high-risk factors for surgery.
Keywords
Hip; Osteoarthritis; WISH-type hip brace
Introduction
Hip Osteoarthritis (OA) is a common joint disorder in aged women. Dynamic lateral instability develops in patients in roughly the third decade of life [1]. An invasive surgical approach, such as Total Hip Arthroplasty (THA), is the most common treatment [2,3]; however, a previous study showed that operative application should be avoided for younger patients [4]. There are few studies that investigated bracing effects. This review focused on the hip-bracing approach as a conservative intervention. This approach has several advantages such as cost-saving and avoiding surgical risks in aged patients.
WISH-type hip brace
Age-associated muscle weakness around the hip joint results in the dynamic lateral instability observed in elderly people [1]. Dynamic lateral instability develops in patients with hip OA, especially female patients [1], and is associated with various symptoms that cause difficulties in performing normal daily activities [5]. Manual internal pressure on the great trochanter relieves the pain during the stance phase of stepping in most patients with hip OA. Wakayama Medical College designed an S-form hip brace for patients with hip OA [1]. The design concept was to reinforce the hip joint by preventing up- and outward movement of the femoral head [1]. Although this brace provided an early alleviative effect [1], the prototype for the WISH-type hip brace was not widely used because of discomfort. Thus, a lighter and more concise WISH-type hip brace was developed.
The WISH-type hip brace is described as follows: “The WISH-type S-form hip brace has been made on basis of the design concept of Wakayama Medical College type, as demonstrated previously [1]. In the original Wakayama Medical College type, the pelvic potion of the hip brace holds it at the right position against pelvis to prevent rotation of the brace, and provides a fulcrum of the lever though a lateral bar. The lateral bar possesses a single joint allowing hip flexion and extension near the peripheral edge. Another joint allowing hip abduction is located at the peripheral edge, and thus the combination of these two joints restricts only hip adduction. The peripheral joint provides a fulcrum between the S-form bar as a power point and greater trochanter pad as a working point. Through a universal joint, the third joint allows the pad face to trochanter correctly, and the pad then pushes the greater trochanter inward when the affected limb is abducted or bears weight. To make the weight lighter and improve the brace more concise, here we utilized Thrust Bearing Hip Joint Assembly, Variable Abduction (Fillauer LLC, Chattanooga, TN) as the lateral bar. An upper extended bar was fixed inside to the lower hip joint bar. Then the greater trochanter pads as well as the universal joint were removed, and instead the greater trochanter pad was fixed directly to the upper extended bar attached to the lower hip joint bar, though a co-polymer polypropylene material. Furthermore, an S-form bar holding the thigh was replaced by co-polymer polypropylene material with continuity to the greater trochanter pad. The resultant brace weighed around 0.9 kg, and the lateral prominence due to lateral bar was reduced. The modified type of the brace was designated as the WISH type, since users’ hope as well as ours is “WISH” to be free from pain.” [6] (Figure 1). After the patients equip a WISH-type hip brace, they are recommended to walk at least a half hour every day for the purpose of strengthening the muscles around the hip joint, which sustains and augments the effect of the brace.
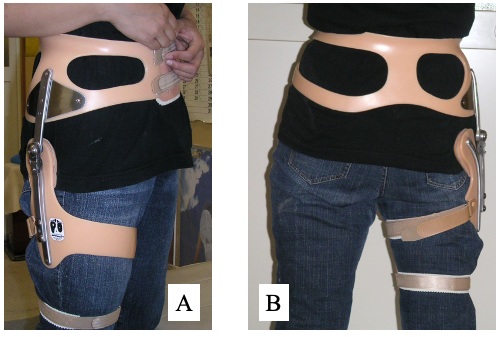 Figure1: Lateral (A) and posterior (B) views of a WISH-type hip brace. The brace can be equipped under pants (see photos of wearing in ref. 6).
Figure1: Lateral (A) and posterior (B) views of a WISH-type hip brace. The brace can be equipped under pants (see photos of wearing in ref. 6).
Direct effects of the WISH-type hip brace
The WISH-type hip brace was applied for patients in whom the hip pain induced during the standing period was reduced by manual pressure onto the great trochanter. Patients immediately reported feeling alleviation of weight-bearing pain when the hip brace was equipped for the first time. To elucidate the direct biomechanical effects of the brace equipment, gait analysis using a force plate was performed and the authors reported shortened time of one step, stronger step, and that the center of gravity of the body shifted to the contralateral side [7]. Especially, a significantly stronger vertical reaction force at the first peak and earlier switch from backward to forward reaction force vectors were obtained [7]. The relief of pain on the stance phase introduced by the brace may result in strong steps in the early stance phase and enhancement of the efficacy of propulsion force by shortening the duration of the braking motion [7].
To evaluate the effect of the brace on postural control in the standing position, a cross test was conducted using a force plate [8]. The hip brace demonstrated a direct effect of augmenting the maximum excursions of the center of gravity in both the medial-lateral and anterior-posterior directions [8] (see photos of testing in ref. 8). Augmentation of the power output of the muscles around hip by the brace may support the movement required for resistance against upper body mass leaning, which allows the excursions to be extended [8]. This improvement was found a few months after the brace application; however, when the brace was applied for the first time, although the brace augmented the muscle strength of the braced leg in both hip flexion and adduction, the improvement was not found [8]. This indicates that the muscle output induced by the brace application was insufficient to improve postural control when applied the first time; however, the improvement of the postural control required the accumulative power output attained by daily muscle exercise.
Indirect effects of the WISH-type hip brace
In most patients, active walking exercise encouraged by the direct improvements in gait biomechanics resulted in a significant improvement of hip scores such as Harris Hip Score [9] and Japanese Orthopaedic Association score [10] by 1 month after equipping the hip brace [6].
Significant improvements of functional mobility were obtained at 3 months follow-up assessment. Time to complete the Timed Up & Go Test (TUG) was improved significantly for patients with bilateral hip OA [11,12]. On the other hand, for patients with unilateral hip OA, significant improvement of TUG was observed in only turning UN braced Leg Inside (ULI) after 6 months, but not Turning Braced Leg inside (BLI) [12]. Furthermore, the improvement was independent of the application of the brace at the assessment. Throughout this study, a significant difference between the mean time of TUG with and without the brace was not detected at each follow-up assessment [8]. This research provides important evidence for the therapeutic effects of the brace being biomechanical effects on walking and turning phase, and indirect balance and muscle power of the lower half of the body, which may be accumulated. Firstly, key evidence for biomechanical effects was obtained by the finding that for patients with unilateral hip OA, improvement in TUG was reported in only turning ULI, but not BLI [12]. This indicates that the brace may support hip function during external and/or abduction movements in turning to the sound leg side on walking. Secondly, in patients with functional mobility improved by the brace, there was a significant negative relationship between TUG and Harris Hip Score [12]. In addition, the improvement of TUG was independent of the application of the brace at assessment throughout the whole period of this study; thus, TUG improvement was demonstrated even when assessment was performed without brace equipment [12].
Throughout the results obtained so far, an important role of the brace is to augment the effects of muscle power, especially that obtained by daily walking as an indirect effect. A short-term longitudinal study revealed improvement in the abduction muscle strength of the affected limb by daily walking exercise with the brace, and that this occurred with little interaction with the sound limb [13].
Limitations
The surgical interventions for patients with painful hip osteoarthritis, such as traditional THA, have developed and improved in terms of quality of implants and operative techniques. This brace does not replace the surgical managements forever, but rather prolongs the timing of the operative interventions. One patient walked too much because of the good feeling after the application of the brace, and showed a resultantly lower hip score, resulting in THA [6]. On the other hand, a patient with a Harris score of less than 70 (poor category), who required loxoprofen sodium every day before application of the brace, enjoyed daily life for 15 years before the patient underwent THA (personal communication). Therefore, an analysis using THA as a dead point is necessary. Another key limitation is strong dependency on the skills by the prosthetist who realizes the concept of the brace. We experienced a patient with a brace with loose adjustment that resulted in pain and reduced hip functions.
Conclusion
The most important advantage of this bracing treatment is the absence of side effects reported thus far. Furthermore, there are many patients with hip OA with severe pain, who are aged and/or have many complications that are high risk factors for invasive operation with general anesthesia. This bracing approach is a suitable intervention for such patients.
Acknowledgement
This work was supported in part by a Grant-in-Aid for Young Scientists JP18K17710 (E.S.) from the Japan Society for the Promotion of Science.
Conflict of Interest
All authors declare that there are no conflicts of interest.
References
- Kawamura T (1983) Development of the S-form Hip brace of Wakayama Medical College Type for osteoarthritis of the hip. J Jpn Orthop Ass 57: 1665-1679.
- Falez F, Papalia M, Favetti F, Panegrossi G, Casella F, et al. (2017) Total hip arthroplasty instability in Italy. Int Orthop 41: 635-644.
- Petis S, Howard JL, Lanting BL, Vasarhelyi EM (2015) Surgical approach in primary total hip arthroplasty: Anatomy, technique and clinical outcomes. Can J Surg 58: 128-39.
- Maradit-Kremers H, Larson DR, Noureldin M, Schleck CD, Jiranek WA, et al. (2016) Long-term mortality trends following total hip and knee replacement: A population-based study. J Arthroplasty 31: 1163-1169.
- Steultjens MP, Dekker J, van Baar ME, Oostendorp RA, Bijlsma JW (2000) Range of joint motion and disability inpatients with osteoarthritis of the knee or hip. Rheumatology 39: 955-961.
- Sato T, Yamaji T, Inose H, Sekino Y, Uchida S, et al. (2008) Effect of a modified S-form hip brace, WISH type, for patients with painful osteoarthritis of the hip: a role in daily walking as a hip muscle exercise. Rheumatol Int 28: 419-428.
- Yamaji T, Usuda S, Sato E, Sato T, Sekino Y, et al. (2009) Biomechanical analysis of gait for patients with painful osteoarthritis of the hip treated with WISH-type hip brace. J Orthop Sci 14: 423-30.
- Sato E, Yamaji T, Sato T, Hasegawa M, Shirakura K, et al. (2016) Effect of the WISH-type hip brace on postural control in patients with osteoarthritis of the hip: Evaluation using the cross Test. Kitakanto Med J 66: 103-110.
- Harris WH (1969) Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J. Bone Joint Surg 51: 737-755.
- Imura S (1995) Evaluation Chart of Hip Joint Function. J Jpn Orthop Assoc 69: 860-867.
- Sato T, Yamaji T, Inose H, Sato E, Yoshikawa A, et al. (2009) Extended application of WISH type S-form hip brace for patients with bilateral painful osteoarthritis of the hip: Report of two cases. Prosthet Orthot Int 33: 173-178.
- Sato E, Sato T, Yamaji T, Watanabe H (2012) Effect of the WISH-type hip brace on functional mobility in patients with osteoarthritis of the hip: Evaluation using the Timed Up & Go Test. Prosthet Orthot Int 36: 25-32.
- Sato E, Yamaji T, Watanabe H (2019) Effects of the WISH-type S-form hip brace on muscle strength in patients with osteoarthritis of the hip: A short-term longitudinal study. Prog Rehabil Med 4: 20190015.
Citation: Watanabe H, Sato E, Yamiji T, Chigira Y (2021) WISH-Type Hip Brace for Patients with Osteoarthritis of the Hip. J Phys Med Rehabil Disabil 7: 64.
Copyright: © 2021 Yusuke Chigira, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.