Introduction
After Spinal Cord Injury (SCI), the sequential process of primary and secondary injury occurs. A few hours post-injury, spinal cord lesions contain inflammatory infiltrate, and undergo necrosis, edema and other micro-environment changes. As all we know, in the Central Nervous System (CNS), inflammatory mediators, such as proinflammatory cytokines, inducible nitric Oxide Synthase (iNOS), COX-2, et al., play a pivotal role in inducing inflammatory responses. Over time, secondary injury occurs and cytokines are up-regulated, which mediate and direct the inflammatory response, and ultimately influence axonal regeneration and functional recovery.
Secondary injury after the primary SCI is the major factor that causes damage on residual neural pathways and their functional loss [1]. The induced immune inflammatory response that occurs after ASCI has an important role in secondary injury. The expressions of a variety of inflammatory cytokines are increased after ASCI, which then mediate immune and inflammatory responses through the cytokine network to enhance cascading inflammatory responses. Doo C. Choi found acupuncture significantly reduced the expression of proinflammatory factors [2]. This study also showed that the damaged zone and its adjacent tissue contained a large number of activated neutrophils, lymphocytes and glial cells, which secreted a large amount of inflammatory factors, which then interacted to worsen the SCI [3,4]. TNF-α binding to TNF Receptor (TNFR) activates and accumulates inflammatory cells, activates endothelial cells and nerve cells, promotes the activation of NF-κB, promotes the secretion of IL-1β, IL-6 and TNF-α, releases cytotoxic oxygen (such as free radicals and proteolytic enzymes), induces the release of arachidonic acid and lipid peroxidation metabolites, damages cell membrane structures, worsens inflammation, increases blood-spinal cord barrier permeability (which further damages the injured spinal cord) and induces apoptosis through a variety of mechanisms [5]. IL-6 is a pro-inflammatory cytokine that might have an important role in the inflammatory regulation of the injured central nervous system. The secretion of IL-6 at the early stages of injury damages nerve cells. However, some studies also suggested that IL-6 had neurotrophic effects, could reduce tissue damage, promote the differentiation of neural stem cells into glial cells, promote the regeneration of neurons, and promote wound healing [6,7]. NF-κB is a transcription factor in the eukaryotic cell Rel/NF-κB family. The intensity of inflammatory cytokine gene expression determines the intensity of the inflammatory response, but the gene expression of inflammatory cytokines is regulated by the transcription factor NF-κB. Normally, the p50/p65 heterodimer and 1-kB form a biologically inactive trimer, and NF-κB activity is regulated by the 1 kB form [8].
The treatment of SCI is still very challenging for modern medicine, the failure of which can lead to multiple dysfunction and complications and thus a heavy burden on patients and their families. Therefore, how to improve and promote the recovery of motor and sensory functions has become the prime target of rehabilitation therapy of patients with SCI. Acupuncture is a therapy of Traditional Chinese Medicine that promotes the recovery of neural function without toxic side effects and has attracted significant domestic and international attention recently. Previous studies have found that Electro Acupuncture (EA) has been used for the treatment of spinal cord injury as it has been shown to significantly improve traumatic paralysis [9,10]. But there is little report on the treatment of spinal cord injury by elongated needle therapy. Elongated needle therapy belongs to kinds of acupuncture that its characteristic has fast conduction, Strong sense. So, elongated needle therapy has a good effect on the treatment of depth of disease. Studies have shown that acupuncture treatment for SCI was significantly effective, reduced both pain and improved the postoperative rehabilitation efficacy [11], and we found to treat urinary retention after spinal cord injury. The elongated needle therapy was better than general acupuncture method which is effective to increase the amplitude and incubate time of SCEP and improved urinary retention [12,13]. However, the molecular mechanism of elongated needle therapy in the treatment of Acute SCI (ASCI) is not fully understood. In this study, we hypothesized that elongated needle therapy would ameliorate functional outcome through inhibition of inflammation after ACSI.
Materials and Method
Experimental animals and grouping
Fifty-four healthy adult male Sprague-Dawley rats (weight 220-250 g) were purchased from the Experimental Animal Center of Xiamen University (Xiamen, China). With a controlled temperature (20 ± 2ºC) and a 12 h light/dark cycle (lights on from 7:00 AM to 7:00 PM). Food and water were available at libitum. After 1 week of adaptive feeding, rats were randomly divided into sham group, control group and elongated needle therapy group. This study was approved by Xiamen University Institutional Animal Care and Use Committee (Xiamen, China).
Animal model and surgical procedures
The modified Allen's method was used to develop a model of ASCI [14]. Before the experiment, animals were fasted for 8 h and the surgery were performed on animals in a random order. All animals in each group were anesthetized by intraperitoneal injection with 10% chloral hydrate (0.3 ml/100 mg). An incision about 2.5 cm long in the middle of the back of animals, fixed in the prone position, was performed aseptically. Skin and subcutaneous tissue layers were cut to expose two long cones above and below the cut, and the T9-T10 spinous process and all lamina were removed to expose a 0.5 cm-wide putamen. The sham group rats were only removed T9-T10 lamina but not exposed spinal cord, contusion injury of elongated needle group and control group were using the homemade impactor (Anhui, China). A Kirschner needle (10 g) was dropped by vertical free fall at 60 mm along the graduated duct, to hit a thin semicircular plastic disc with a diameter of 4 mm and width of 2 mm. After injury, the needle was removed quickly. This caused moderate damage to the dorsal horn of the spinal cord of the rats. The incision was sutured for all the rats.. The experiment was performed at 37 ± 0.5o<>C and the postoperative suture used 4-0 silk. Daily post-operative intraperitoneal injection of penicillin (80 U/d) was used to prevent infection. The rats were fed in separate cages at 200-250C with food and water at room temperature. Rat bladders were massaged 3 times a day to help urination until the establishment of reflex bladder emptying. To determine the success of the model, the following factors were observed: SCI was surrounded by edema, rat had tail reflection, both lower limbs and body had retraction-like fluttering and both lower limbs had flaccid paralysis after recovery from anesthesia. To determine the success of the model of sham surgery, Basso, Beattie and Bresnahan locomotor rating scale (BBB), were assessed immediately after surgery, if the score is 20-21 points, which indicates the sham operation successful.
Treatment method
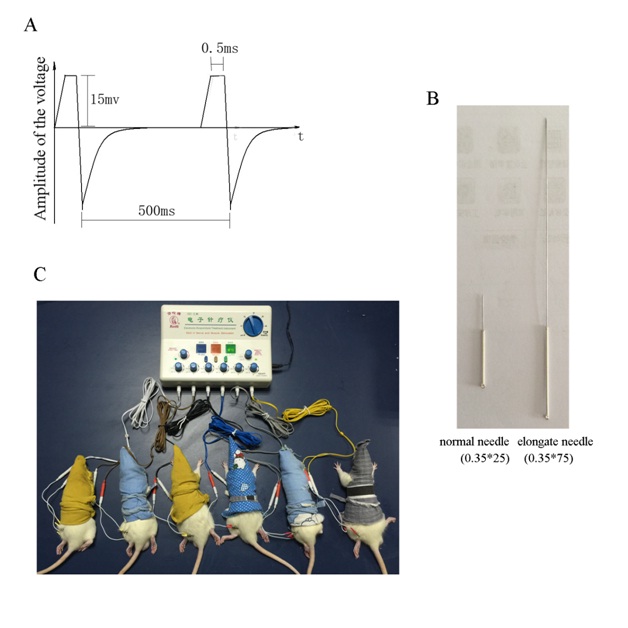
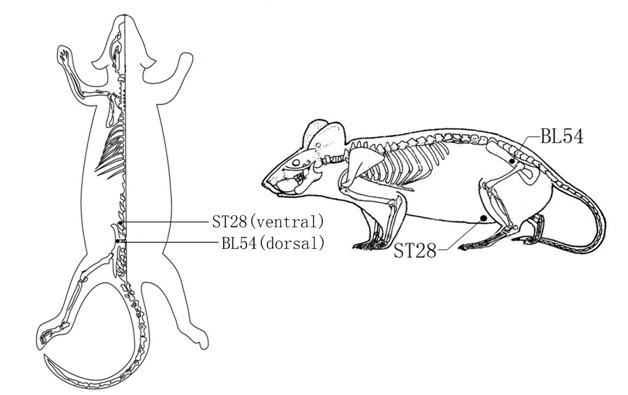
After the success of modeling, the control group was untreated. The sham and elongated needle therapy group immediately received acupuncture treatment after recovery from anesthesia (Figures 1A-C). Rats were fixed with self-made rat bags [15] (Figure 1C). Acupuncture points were selected according to the international World Health Organization (WHO) standard as follows (Figure 2): [“ST28 (Chibian)”]: the intersection of outside 1/3 and middle 1/3 connection of the large trochanter of femur and sacral coccygeal vertebra joint on the lower hip; [“BL54 (Water channel)”]: on the abdomen, about 2 cm from the third section above the connection of the thoracic sword and symphysis pubis midpoints (divided into 13 equal sections). Acupuncture was performed on both side of the rats body. Skin on acupunctured sites was disinfected and elongated needles (0.35*75 mm in diameter, Suzhou Hua Tuo Medical Instruments Co., Ltd. China, Su Zhou) as distinct from the normal acupuncture (Figure 1B) were acupunctured to a 2-3 cm depth, twisted for 1 min and stimulate for 15 minutes. “ST28” and “BL54” on the same sides formed a circuit when connected to a SDZ-II electrical stimulation instrument (Suzhou Medical Supplies Co., Ltd.) with the following therapeutic parameters: frequency of 2/100 Hz, current of 15 mV [16], stimulation for 15 min and elongated needle therapy once every alternate day (Figure 1A and C).
Model evaluation and movement function test
After the establishment of ASCI, the motor function scores of rats was assessed with the Basso Beattie and Bresnahan locomotor rating scale (BBB) in a random order [17]. After spinal cord injury, rat activity in an open field was assessed. Limited hind limb activity was observed and rats could not support their body weight and had to use their forelimbs to move. Rats with a score greater than 2 indicates failure of modeling and were removed from experiments, which would be added later under the same conditions (Rats with a score less than 2). On days 1, 3 and 7 after modeling, BBB scores were determined to study the recovery of hind limbs of rats with ASCI. Score standards, according to the number of movable joints of rat hind legs, co-ordination ability and fine joint activity, were divided into 21 levels. Higher scores indicated a better recovery.
Sampling of spinal cord tissue
Rat tissue sampling from the model and elongated needle therapy groups was done according at day 1, 3 and 7 after treatment; rats were assessed with the Basso, Beattie and Bresnahan locomotor rating scale (BBB) in a random order. Then, for the sampling, an overdose of chloral hydrate (0.3 ml/100 mg) was injected intraperitoneally. After the animal was anesthetized, injured spinal cord (two 0.5 cm regions above and below the injured segment) was quickly removed, placed on ice, immersed in liquid nitrogen, and then transferred to a -800C fridge (Haier, China) after 5 min.
Extraction of tissue homogenate
The spinal cord tissue was thawed on ice, and 3 ml of lysate was added to 1 g of tissue for ultrasonic homogenization in an ice bath and then centrifuged at 12,000 r/min for 15 min at 40C. After letting the sample stand for 20 min, 500 µl of centrifugal supernatant was stored at -200C until further usage.
Enzyme Linked Immunosorbent Assay (ELISA) analysis
Determination of inflammatory cytokines was carried out in accordance with the TNF-α, IL-6, IL-1β and NF-κB ELISA kit manufacturer’s protocol (TSZ, USA). Briefly, the T9-T10 segment of spinal cord tissue was removed and homogenized to harvest the supernatant. The extracted supernatant and standard samples at different concentrations were applied to wells (50 μl / sample) before closure of the plate membrane. Samples were then incubated at 370C for 30 min and washed five times with PBS. For each well, 50 μl of enzyme reagent was added and the preparation was again incubated and washed, followed by the procedure of color development. With zero correlation based on the negative control well at 450nm wavelength on a micro-plate reader, the standard curve was established based on the measurement results of the standard solution. The Optical Density (OD) for each well was measured and the actual concentration of each sample was determined.
Statistical analysis
All data collected in this study will be used to power future full-scale studies and analyzed using SPSS 16.0 Statistical Software (SPSS Inc., Chicago, IL, USA). Obtained data were expressed as the mean ± Standard Deviation (SD). Significant differences were assessed by two-tailed Student’s t test or one-way ANOVA followed by the Student-Newman-Keuls test, P < 0.05 indicated that the difference was statistically significant.
Results
Effect of modeling in rats
We used a total of 55 rats in this experiment. 18 rats were used in sham group and in sham surgery there was 100% success. In elongated needle group and control group a total of 37 rats are used. In which 1 rat died immediately after surgery. The total effective rate is 98%.
Behavioral observation and BBB scores
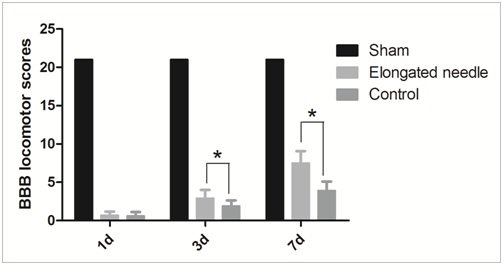
To determine the elongated needle therapy functional recovery improvement after SCI, BBB Locomotor Rating Scale was used to assess the functional recovery. The lower limbs of normal rats could move normally after recovery from anesthesia and they had a BBB score of 21. After injury, both the lower limbs of rats in the control group and elongated needle therapy group were unable to move after recovery from the anesthesia, showing delayed paralysis and a BBB score of 0. This indicated that the modelling was successful. One day after the operation, the muscle tension of the lower limbs of rats was increased with spastic paralysis and no joint activity was observed. 3 days after the operation, the muscle tension of the lower limbs of rats in both groups was decreased, compared with that on the second post-operative day and mild activities of 1-2 joints was observed. 3 days after the operation, the hip, knee and ankle joints of rats in the control group showed mild activity and three hip, knee and ankle joints of rats in the elongated needle therapy group had activities with a large range. In addition, the dominant paw of some rats had plantar touchdown, but without a heavy load. Rats exhibited immediately paraplegic with no observable hindlimb movement after surgery. This was followed by a gradual recovery with the time going, especially with the treatment of elongated needle. Elongated needle administration in rats showed a significant improvement in the BBB scale compared with control group (p < 0.05) on 3d, and elongated needle group is still higher than control group on 7d (Figure 3), but this improvement did not reach the level of sham one.
TNF-α, IL-6, IL-1β and NF-κB expression in ASCI rats
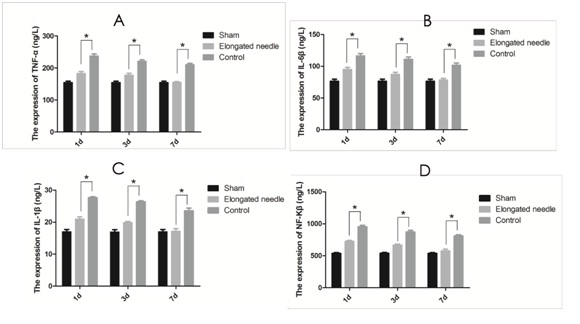
As shown in figure 4, there was low expression of TNF-α, IL-6, IL-1β and NF-κB in spinal cord tissues of normal rats; After SCI, and then gradually decreased. TNF-α belongs to the TNFR family. The expression of TNF-α in normal rats is little. Rats exhibited immediately increased of the expression of TNF-α in rats after surgery. IL-6 is a pro-inflammatory cytokine that might have an important role in the inflammatory regulation of the injured central nervous system. The expression of IL-6 in normal rats is little. Immediately after surgery the rats exhibited increased expression of IL-6. The expression of IL-1β in normal rats is little. Immediately after surgery the rats exhibited increased expression of IL-1β. NF-κB is a transcription factor in the eukaryotic cell Rel/NF-κB family. The expression of NF-κB in normal rats is little. After surgery the rats exhibited increased expression of NF-κB. This was followed by a gradual decrease with the time, especially with the treatment of elongated needle. Elongated needle administration in rats showed a significant decrease in the expression of TNF-α, IL-6, IL-1β and NF-κB compared with control group (p < 0.05) on 1d and Elongated needle group is still higher than control group on 3 and 7d (Figures 4A-D).and the expression level was close to the normal rats at 7 days.
Discussion
In our study we found that elongated needle therapy can suppress the expression of various inflammatory cytokines and thereby improved functional recovery after SCI with the time going.
As all we know, treatment of SCI remains a challenging topic in neuroscience. Many long-term studies have shown that acupuncture treatment can improve sensory and motor functions and alleviate advanced neurological dysfunction in patients with ASCI [18,19]. During our assessment, improvements of BBB score were observed in rats with SCI after acupuncture treatment for 7 days. Significant restoration of motor activities was observed of the spinal cord. Thus, Elongated needle therapy was considered to be effective in the treatment of ASCI.
After spinal cord injury, exposure to trauma, hypoxia, Lipopolysaccharide (LPS), radiation, cytokines (such as IL-1β, TNF-α) and other factors, protein kinase is activated through intracellular signal transduction to cause the separation of NF-κB from the trimer. After elongated needle treatment, stimulation, NF-κB is transported into the nucleus to induce target gene expression, which increases acute response proteins, neuropeptides, adhesion molecules and the production of cytokines (such as TNF-α, IL-6 and IL-1β amongst others) involved in the inflammatory process [6,20,21]. Many studies have shown that acupuncture has anti-inflammatory, analgesic and anti-lipid peroxidation effects. Furthermore, it can prevent cell damage and fight against apoptosis [22-25]. As indicated by this study, following SCI, there were significant elevations of pro-inflammatory factors such as NF-kβ, TNF-α, IL-1β and IL-6. After the application of ENT, levels of NF-kβ, IL-6, IL-1β and TNF-α in the injured spinal cord tissues significantly decreased, along with notable anti-inflammatory effects.
Pro-inflammatory cytokines, such as IL-6, TNF-α and others, were significantly increase at early ASCI stages and the cascading inflammatory response induced apoptosis and inhibits the recovery of neurological function [26]. If the cascade was blocked at an early stage of SCI by inhibiting NF-κB activation, inflammation and secondary injury might be reduced. Therefore, this might be an effective method to treat ASCI. A large number of studies have shown that acupuncture has anti-inflammatory, analgesic, anti-lipidperoxidation and cell damage prevention effects [27-29]. Its anti-inflammatory effects are achieved by inhibiting the proliferation and activation of T lymphocytes, neutrophils and monocyte-macrophages. It also inhibits calcium channels to decrease Ca2+ concentrations within inflammatory cells, which decreases the activity of Ca2+-calmodulin that inhibits the generation and release of multiple inflammatory mediators. This study found that compared with the model group, the content of inflammatory factors and NF-κB can be decreased obviously and the effect of the elongated needle therapy group is better than that of the control group. With the extension of time, the content of inflammatory factors and NF-κB in the elongated needle therapy group decreased more rapidly and the motor function of the Basso, Beattie and Bresnahan locomotor rating scale scores better than control group, promote the recovery of motor function in rats. After SCI, the expression and secretion of IL-1β, TNF-α and other inflammatory cytokines increased, which acted on NF-κB activation as a downstream cytokine to form a positive response. Because ASCI cause severe inflammatory process evolution during the early stages, early treatment should be implemented to maximize the effect of inflammatory inhibition. In this study, the elongated needle treatment was performed after SCI in the early. Furthermore, acupuncture treatment significantly reduced the concentrations of NF-κβ, IL-6, IL-1β and TNF-α in the injured spinal cord, which might be one mechanism of how elongated needle therapy promotes nerve cell survival and helps restore motor function during the later stages of SCI.
Although we found that elongated needle therapy can promote recovery after spinal cord injury, and inhibition of inflammation seems to have involved in this process. However, the mechanisms of spinal cord injury have many more, such as apoptosis, inflammation and neurodegenerative [30], whether the elongated needle treatment is also involved in this process, we do not know. Secondary multiple injury after spinal cord injury is the result of interaction of multiple factors. Therefore, when the exact mechanism of elongated needle treatment of Spinal Cord Injury (SCI) is clear, we can take more effective interventions to promote the recovery of spinal cord injury.
Conclusion
Elongated needle therapy would improve functional recovery via its inflammation-suppressing effect after acute spinal cord injury, these findings provide a theoretical basis for the clinical application of elongated needle therapy in the treatment of ASCI.
Acknowledgements
This study was supported by the Chinese medicine research Foundation of Zhejiang Province (Grant No 2008CB067 to Quan Renfu) and Natural science foundation of Zhejiang Province (Grant No LY15H270003 to Quan Renfu).