ABSTRACT
Background
This study aimed to determine the measurement of spinal canal and spinopelvic parameters in Congolese population of Kinshasa.
Materials and methods
212 clinically asymptomatic were enrolled during 2014-2015; 138 subjects (65.1%) were male and 74 (34.9%) were female of matching age between 18 and 30 years.
Radiological study consisted of simple anteroposterior and lateral radiographs as well as computed tomography of the lumbar spine.
The following spinopelvic parameters were measured PI (Pelvic Incidence), Lumbar Lordosis (LL), Sacral Slope (SS) and Pelvic Tilt (PT).
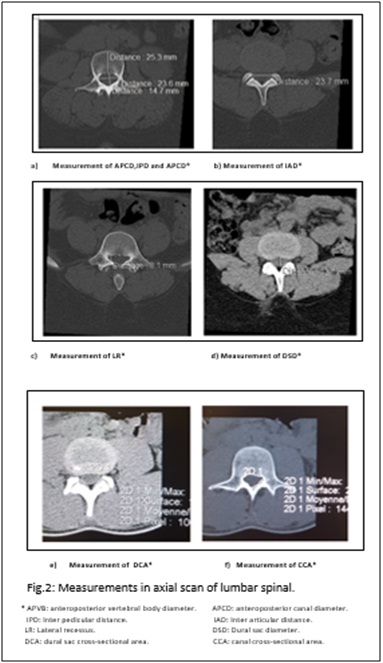
Measurements in axial scan included midline Anteroposterior Vertebral Body diameter (APVB), midline Anteroposterior Canal Diameter (APCD), midline Dural Sac Diameter (DSD), Dural sac Cross-sectional Area (DCA), Canal Cross-Sectional Area (CCA), Interarticular Distance (IAD), Interpedicular Distance (IPD), Foraminal Height (FH) and Lateral Recess (LR). The Lumbar Ratio (LR) was calculated by dividing APCD by APVB.
Results
The mean ± SD of the measurements at the narrowest level except L5-S1 was:
APCD = 15.12 ± 2.30 mm, IPD = 20.31 ± 3.50mm, LR = 5.35 ± 1.40 mm, IAD = 16.32 ± 2.22mm, DSD = 12.12 ± 2.11mm, FH = 18.50 ± 1.7mm, DCA = 169.27 ± 48.54mm2, CCA = 251.80 ± 36.10mm2 and R = 0.54 ± 0.02.
The mean ± SD spinal and pelvic parameters were: LL = 61.1 ± 9.7°, PI = 54.4 ± 7.8°, SS = 41.0 ± 8.4° PV = 13.2 ± 6.5°.
Conclusion
The report is the first to present the normal radiological anatomy of different diameters of the lumbar spinal canal among adult Congolese population. These diameters are smaller than the measurement in Caucasian population.
KEYWORDS
Congolese; Lumbar spinal canal; Measure; Spinopelvic parameter
Introduction
In the purpose of establishing normal dimension of the spinal canal, some authors have measured the spinal canal’s diameter. That has been the case of Hinck et al., in Caucasians Latino America [1], Eisenstein et al., among black and white people in South Africa [2], Amonoo-in kuofi et al., among Nigerians [3], Orthan et al., among Turks [4], Ongolo et al., among Cameroon [5] and Nirvan et al., among India [6]. Racial and ethnic variations have been noted [7].
Few years ago, sagittal parameters of the spine have become inescapable and have constituted a revolution in the diagnostic and therapeutic of spinal disorders [8]. However, in Democratic Republic of Congo (DRC), the profile of the spinal canal and sagittal parameters has never been documented.
The purpose of this study is to determine the normal range of different diameters of canal and sagittal spinal in normal Congolese population.
Materials and Methods
Subjects
212 clinically normal adult males and females of matching age between 18 and 30 years were selected for the present study. The subjects were volunteers from various city of Kinshasa.
Exclusion criteria were: past or present back pain, presence of spinal diseases, spinal configuration anomalies, history of spinal traumatism, metabolic diseases, pregnancy.
Collection of demographic and medical data
At each selected topic, the demographics (age and sex) and clinical (height and weight) information were collected. Body Mass Index (BMI) was calculated as weight in kilograms (kg) divided per the square of height in meters (m).
Radiological study
Radiological study consisted of simple anteroposterior and lateral radiographs in standing position as well as computed tomography of the lumbar spine. Special care was taken to visualize both femoral heads on this x ray. CT (Computed Tomography) scans performed with patients in the supine position using Somaton Sensation 64 (Siemens, Germany).
Spinopelvic parameters (Figure 1), the morphological type of the canal spinal, the spinal canal configuration and the different measures by a single observer.
The following spinopelvic parameters were measured using the worldwide principal protocol [9]:
- PI (Pelvic Incidence) is measured as the angle between a line drawn perpendicular to the sacral end plate at its midpoint of the femoral head axis;
- Lumbar Lordosis (LL) is the sagittal Cobb angle measured between the superior end plate of L1 and the inferior end plate of L5;
- Sacral Slope (SS), angle between the horizontal and sacral plate;
- Pelvic Tilt (PT), angle between the vertical and the line through the midpoint of the sacral plate to femoral heads axis.
Most measurements in this study were based on those in published studies [9-11] in CT. Cuts below the pedicles were made through the highest part of the intervertebral foramina and the following parameters were measured (Figure 2): midline Anteroposterior Vertebral Body diameter (APVB), midline Anteroposterior Canal Diameter (APCD), Canal Cross-Sectional Area (CCA) and Interpedicular Distance (IPD). These cuts were made at the level of the middle of disc and are concerned with the intervertebral articulation and the following parameters were measured: midline Dural Sac Diameter (DSD), Dural sac Cross-sectional Area (DCA) and Interarticular Distance (IAD). The others cuts were made to measure Foraminal Height (FH), the Lateral Recess (LR).
The lumbar Ratio (R) was calculated by dividing APCD by APVB. Likewise, measurements that were less than the mean - 2 SD were considered to be “below normal”.
Reproducibility
106 patients were randomly selected for evaluation of inter observer variability of measurement by two independent observers. To obtain intra observer variability, the same measurement was repeater after 1 month. The intra and inter observer reliability was excellent (Kappa = 0.92) and (Kappa = 0.64) right respectively.
Statistical analysis
Statistical analysis was performed using SPSS 20.0 for windows (SPSS Inc. Chicago, IL, USA).Data are expressed as percentages and the mean ± standard deviation. The relationship between two continuous variables was assessed using a bivariate correlation method (Pearson’s correlation).
Results
Description of the study population
The study population consisted of 212 subjects with a median age of 24.2 ± 2.2 years old (74 female’s and138 male’s). Weight, height and BMI means of participants were 56.8 kg, respectively, 167.3 cm and 20.5 kg/m2. Three out of 10 (29.7%) were lean (BMI < 18.5 kg/m2), overweight and obesity were however 8.5% and 1.4% respectively (Table 1).
Quantitative measurements
The mean ± SD of the measurements at the narrowest level except L5-S1 and the minimum dimension are summarized in table 2. The normal value are: APCD ≥ 10.5 mm, IPD ≥ 16 mm, LR ≥ 2.5 mm, IAD ≥ 11.5 mm, DSD ≥ 7.5, DCA ≥ 70 mm2, CCA ≥ 179 mm2 and TR ≥ 0.50.
Spinal and pelvic parameters of the sagittal balance of the pelvis-spine complex
The mean ± SD minimum and maximum spinal and pelvic parameters are summarized in table 3. The average lordosis was 61.1 ± 9.7°, pelvic incidence was 54.4 ± 7.8°, 41.0 a sacral slope of ± 8.4° and pelvic version 13.2 ± 6.5°.
There was a close correlation between sacral slope and pelvic incidence (r = 0.61), lumbar lordosis and sacral slope (r = 0.64), lumbar lordosis and pelvic incidence (r = 0.68) (Table 4).
Discussion
The average age of the study population was 24.2 years of which 65.1% were male against 34.9% female with an average size of 167.3 cm, an average weight of 56.8 and a BMI of 20.5 kg/cm (Table 1). The male dominance can be explained in this random sample that by easy acceptability of men at risk and exclusion of women in cases of amenorrhea, or the date of the last unknown rules.
The youth of our sample was justified by the fact that bone growth is usually completed at the age of 17 years and maximum of 30 years in that before this age the risk of bone degeneration is low.
The main result of this research was to determine reference values of lumbar spinal canals. The threshold values defining the anatomical lumbar stenosis were: DAP < 10.5 mm DIP < 16 mm, LP < 2.5 mm, DIA < 11.5 mm, DFD < 7.5 mm, DF < 15 mm, C / V < 0.50, SC < 179 mm
2 and SD < 70 mm
2These values are well below the values proposed by the classical treatises. Indeed, for classical treatises of French literature, DAP has values:
- Normal value ≥ 15 mm
- Closeness on: 13 and 14 mm
- Closeness absolute ≤ 12 mm [10-15].
For the DFD, cited the normal dimensions of at least 11 mm [10-15].
In English literature, the “Atlas of radiology measurement” by Keats TE and Silstrom C. Mosby 2001 [16] cites as normal value ± 16 mm 3 in L4 of DAP.
These reference values are no less indicative as severe strictures are not incompatible with the absence of symptoms and, conversely, even normal dimensions on supine exams can be significantly reduced by the static conditions or dynamics of standing. In addition, the statistical standard does not necessarily correspond to the boundary between normality and pathology: an individual whose actions deviate more than two standard leads do not mean a sick individual.
Analysis of the sagittal balance of the spine is a fundamental step in the understanding and treatment of many spinal pathologies. One objective of this work was to determine the physiological values of pelvic and spinal parameters of sagittal balance of the spine and to study their interrelations. Hyperlordosis of African described by Courson in 1963 [16] before a clinical aspect of high-lumbar curve corresponds to different values of the pelvic and spinal sagittal balance parameters of the lumbar spine?
The average values of the main angular parameters considered were: lumbar lordosis 61.1 degrees (± 9.7), sacral slope 41.0 degrees (± 8.4), pelvic Version 13.2 degrees (± 6.5) and 54.4 degrees pelvic incidence (± 7.8). There was a close correlation between sacral slope and pelvic incidence (r = 0.61), lumbar lordosis and sacral slope (r = 0.64), lumbar lordosis and pelvic incidence (r = 0.68).
Morphotype pelvic spinal black Africans present values comparable to the literature [8] and meets the same provisions of anatomical and functional interdependence of sagittal balance of the lumbar spine.
Conclusion
The report is the first to present the normal radiological anatomy of different diameters of the lumbar spinal canal among adult Congolese population. These diameters are smaller than the measurement in Caucasian population.
Ethics and Disclosures
The protocol for the study was approved by the institutional review board of Kinshasa university hospital (ESP/CE/009/2016). Informed consents have been obtained in writing from patients, and all clinical investigations were conducted according to the principles expressed in the declaration of Helsinki. The patients have given their consent for publications of the clinical details.
There was no funding received for this study and there was no conflict of interests.
Figures
Figure 1: Spinopelvic parameters in lateral radiography of lumbar spine.
Figure 2: Measurements in axial scan of lumbar spinal.