Substance Use among Women and Children in Afghanistan: The Complexities of an Important Public Health Issue
*Corresponding Author(s):
Abdul Subor MomandDepartment Of Obstetrics And Gynecology, University Of North Carolina At Chapel Hill, North Carolina, United States
Tel:+1 9194485641,
Email:subor@email.unc.edu
Abstract
National surveys of substance use among those living in Afghanistan show multiple substances are easily accessible and commonly used in combination. Substance use in Afghanistan is complex, compounded by the fact that almost half (48%) of the population is comprised of youth under 15 years of age. The number of women and children who report substance use has increased alarmingly over the last decade and a half. And while substance use disorder treatment services have expanded in Afghanistan’s urban areas, there is still a need for evidence-based and culturally appropriate substance use prevention and treatment programs in rural areas. To fulfill the country’s constitutional obligation, which includes an increase in the provision of prevention and treatment programs, there is an obvious need for institutions to strengthen and refine the coordination of counternarcotics efforts.
Keywords
Afghanistan; Children; Substance use; Women
INTRODUCTION
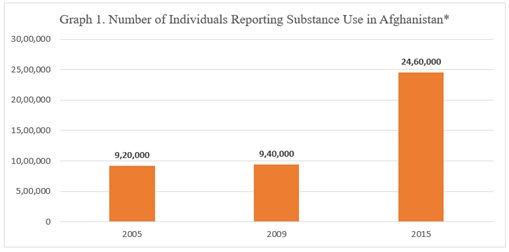
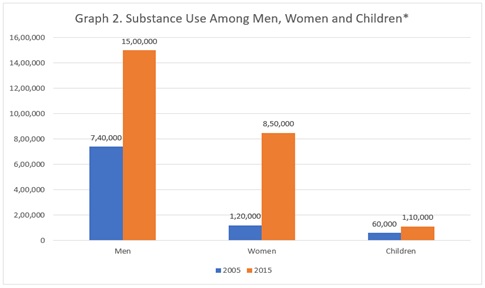
Afghanistan and its people have strained under conflict for many decades. As security steadily declines and government infrastructure ebbs and flows, the country faces multiple public health challenges. Narcotics/substance production, cultivation and availability remain challenges for the nation’s security and stability and they have received greater attention than the related and urgent issue of problem substance use [1]. Problem substance use is one of the most critical health challenges faced by men, women and children in Afghanistan. As seen in table 1, from 2005 to 2015, three substance use surveys were conducted in Afghanistan; however, the differing methodology of these surveys leads to results that cannot be compared across time. In spite of limitations, as seen in graph 1, there are patterns of how substance use has increased in the population. All surveys suggest that substance use is more prevalent in men than women and children, as seen in graph 2. In 2005, the first substance use survey conducted in Afghanistan estimated that 3.8% of all age groups were using substances, and the most commonly used were hashish, opium, heroin and pharmaceutical drugs [2]. In 2009, a follow-up survey showed that 8% of the population, ages 15-64 years, was using substances and since 2005 there has been a 53% increase in the number of regular opium users and a 140% increase in the number of heroin users. The 2009 survey also showed that 50% of parents who were using opium were also giving opium to their children to ease opioid withdrawal, as well as a means to control children’s behavior and/or hunger [3]. In 2015, the Afghanistan National Drug Use Survey [4] found that 11% of the Afghanistan population tested positive for substances by using confirmed biological testing and 7.3% were estimated to use substances. The national adult substance use rate was 12.8%; more than double that of the global substance use rate of 5.2% [5]. The most common substances used in Afghanistan are opioids (4.9%) followed by cannabis (2.2%) and prescription sedatives (almost 1%) [4]. Among individuals using substances, 40% reported using two or more than two substances simultaneously in the past 12 months [3]. Further, Afghanistan is facing significant substance use problems among its youth, with at least one person in every three households reporting substance use [4]. The drivers of rising illicit substance production and substance use may include the ravages of four decades of war, easy access to cheap substances, limited access to substance use disorder treatment [3], prevalent poverty, severe gender inequality, ever increasing civil insecurity, movement of refugees, internal displacement, urban crowding, corruption, an absence of timely or predictable justice and overall lack of stable governance [1]. Responses to these drivers have been fragmented and are in need of more effective coordination. This commentary provides a unique look into substance use among women and children in Afghanistan with an eye toward future action and improved cross-sector coordination.
|
Name of Survey |
Methodologies Used |
|
Afghanistan drug use survey 2005 |
Cross-sectional survey in which they interviewed 1,480 key informants and 1,393 individuals who use substances. The respondents were randomly selected in 32 provincial capitals, 30 district centers and 152 villages. The focus of this survey was on substance use in all age groups. |
|
Drug use in Afghanistan: 2009 survey executive summary |
Cross-sectional survey interviewed 2,614 drug users and 2,614 key informants. Key informants were those having knowledge of drug use in their communities such as teachers, health care workers, police and community leaders. Key informants provide contacts those they knew to be regular users of substances. Those who used substances regularly during the past 12 months and 30 days were defined as individuals who were regular substance users. Respondents were based in all 32 provincial capitals, covering 354 district centers. The focus of this survey was on problem substance use. |
|
Afghanistan national drug use survey 2015 |
This survey combined results of two surveys conducted in urban and rural areas of Afghanistan over the period 2012-2014. This survey used the household-based sampling method and collected hair, urine and saliva from 10,549 men, women and children from approximately 3,000 households and then tested the samples in a lab for substance traces. |
Table 1: Details of survey methodologies.
*Data are from the Afghanistan Drug Use Survey 2005, Drug Use in Afghanistan 2009 Survey, and Afghanistan National Drug Use Survey 2015.
*Data are from the Afghanistan Drug Use Survey 2005, Drug Use in Afghanistan 2009 Survey, and Afghanistan National Drug Use Survey 2015.
WOMEN AND SUBSTANCE USE
Afghanistan is home to 31.6 million inhabitants, with 71.5% of the population living in rural areas, 23.7% living in urban areas, and 4.8% estimated to be nomadic. Of the total population, 49% are female [6]. The overall literacy rate is 31.74%, with females less literate than males (17.61% vs. 45.42%) due to the severe cultural obstacles females face [7]. Within the span of a decade, the number of women estimated to use substances skyrocketed 608%, from 120,000 [2] in 2005 to 850,000 [4] in 2015. The three most common substances that women use are opioids (6.7%), sedatives (1.5%) and cannabis (1.5%) [4]. Another significant [3] finding is that among women who use opium, 78% report having given opium to their child (ren) and/or another family member. Women who are users of substances are more likely to be widowed or divorced, have had little formal education, and are more than twice as likely to be unemployed compared to women who do not use substances [3]. Ingesting substances is the most common (69%) way women report using a substance, as it is considered to be more socially acceptable than other routes of administration and implies the substance is for medical purposes. More than half (52.2%) of women report that they were exposed to substances for the first time by a close family member, especially a husband and almost half of women who report using substances are unemployed. Of those who report being employed, most they work as carpet weavers or in the professions of embroidery or farming [8].
Being born female in Afghanistan can be an added life hardship given that tremendous gender inequality exists. Thus, when girls or women use substances, there is a double stigma and prejudice against them, even if their own family members introduce them to substances. Such a situation occurs, in part, due to a patrilineal society where notions of honor and shame create separate and unequal gender roles. In this cultural system, which emphasizes that women bear their family’s honor, women lead a life of seclusion and chastity and men control and govern women’s relationships with the outside world. On the one hand, bearing family honor can be a protective factor to prevent substance use. On the other hand, the introduction to substances by family or male “protectors” can make it even harder for females to find and utilize treatment help. Further, women face gender inequality in the labor market. Though women play an important role in all dimensions of agricultural production, including in opium production and they are often the main source of household income through opium or other domestic work, such as carpet weaving, women rarely control the marketing of their products. Marketing is most often managed by male relatives.
Women in Afghanistan face constitutional equality but legal inequality. Great discrepancies exist between civil law, customary law and Islamic Law-as well as the informal justice system, which tends to grant women even fewer rights. Years of conflict and violence have further eroded the protection of women’s rights and a culture of impunity reigns as far as violence is concerned, including violence against women inside and outside the household. The present deteriorating security situation in many parts of the country constitutes the most serious obstacle to promoting rule of law, reducing the harms of substance use, improving respect for human rights and the introduction of legal reform, which would benefit women more than any other group in society [9].
The fertility rate in Afghanistan is 5.3 births per woman and the size of the average household is 8 people [10]. Usually women in Afghanistan are the main caregivers for the entire family. Thus, when a woman’s substance use becomes problematic, it can have a radiating effect and compromise a family stability. While active, harmful substance use by any household member can be destabilizing for a family, Afghanistan lacks any enforced child protection system to ensure that children are physically and mentally safe. A decade ago, woman who were using substances were not visible in society, but the situation has changed. It is more common to see women using substances in hotspot areas where many people use substances (e.g. under bridges).
CHILDREN AND SUBSTANCE USE
Afghanistan has one of the youngest and fastest growing populations in the world. Almost half (48%) of the population is under the age of 15 years, while adults age 65 years or older represent only 3.7% of the nation’s population. Having such a young population is both an opportunity and a threat [11]. A ‘youth bulge’ is an opportunity for economic development, if youth are provided with education and skills training, yet it also poses a threat as an insurgent group can easily use uneducated youth for their own purposes. Each year, 400,000 youth enter the Afghanistan job market, but the opportunities for an economically rewarding job are limited [11] and even more limited for females.
The 2005 substance use survey estimated that 60,000 children in Afghanistan were using substances [2], but in 2015 that number jumped to 110,000 [4], an 83% increase. In addition to direct substance use, Afghan children are facing challenges regarding second- and third-hand opioid smoke. Findings from a 2008-2011 study, conducted by International Narcotics and Law Enforcement Affairs, that compared 20 homes where heroin/opium was smoked with 10 control homes, indicated that children as young as nine months old had detectable amounts of morphine in their hair samples. For example, in a sample of hair from a 10-year-old girl, there was 8350 pg/mg morphine, 4652 pg/mg codeine and a heroin metabolite 6-acetylmorphine concentration of 5607 pg/mg. Even large amounts of opioids were detected in the air and surface samples of homes where opium was smoked which poses risk to children (and all household members) of third hand exposure. Of the hair samples from children in homes where opium was smoked, 74% of children ages 2-14 years tested positive for opiates [12]. Among children ages 0-14 years who were tested in Afghanistan, 9.2% were positive for psychoactive substances and 90% were exposed through either their environment or by caregivers who gave them substances [4].
Substance use disorders appear to be more problematic with early onset use, as there is an increased likelihood of damage to the developing brain from the use of many psychoactive substances [13]. The larger the number of adolescents and young adults exposed to experimenting with alcohol, tobacco and illicit psychoactive substances, as well as controlled psychoactive medications, the larger the rate of increase in a vulnerable population at risk of developing addiction [14].
In addition to substance use, children living in Afghanistan are also exposed to war and trauma. For example, among a sample of children interviewed in Afghanistan, 82.4% reported at least one war-related event during their lifetime and 48.6% reported experiencing at least one war-related event in the past year [15]. Children also reported experiences of trauma in their home life. Further, 10.3% of Afghan children ages 5-14 years are involved in child labor, 15% of girls marry before 15 years of age and 40% marry before the age of 18 years. About 74.4% of children ages 2-14 years are disciplined violently and face aggression and/or physical punishment. Thus, there is a need for urgent actions to protect children from such situations [16]. One study found that children seeking substance use treatment have suffered serious social and psychological problems that need intense attention and at the same time treatment in a residential setting has been shown to reduce the severity of the problems by the time of treatment discharge [17].
EMERGING OF NEW SUBSTANCES AND POLICY ISSUES
Despite having the highest in-home opiate production rate in the world and relatively common cannabis production, another significant problem on the Afghanistan horizon is the production of amphetamine-type stimulants and synthetic substances. Methamphetamines are notably increasing in use across the country in addition to opiates [18]. The President of Afghanistan, Ashraf Ghani, told a Turkish news channel during an interview in July 2019 that “the relation of [the] Taliban with the criminal economy is a global issue [and] a regional issue and now [the production of] crystal methamphetamine is going to surpass that of heroin” [19]. While opium poppy cultivation has not decreased, synthetic substance production is soaring. Thus, Afghanistan is coming under the double burden of opium and methamphetamine production.
Nowadays, no one can deny the existence of substance use in Afghanistan. The alarming increase among women and children in the prevalence of substance use can be seen across the country. As noted earlier, the prevalence among women increased 608%, while the prevalence among children increased 83%. The government is responsible for counter narcotics, as described in the 2004 Constitution of Afghanistan, Article 7: “The state shall observe the United Nations Charter, inter-state agreements, as well as international treaties to which Afghanistan has joined and the Universal Declaration of Human Rights. The state shall prevent all kinds of terrorist activities, cultivation and smuggling of narcotics and production and use of intoxicants [20]. But the efforts of counter narcotics have not been effective and the counter narcotic law of Afghanistan has been revised four times since 2003 [21], without proper enforcement. The fight against illicit narcotics does not appear to be a consistent priority either for the Afghan government or for the international community. In fact, in 2019 the Ministry of Counter Narcotics, which was the leading agency for counter narcotics policies during the past 15 years, was dissolved [22].
FUTURE OPPORTUNITIES FOR ACTION
Substance use in Afghanistan is sky rocketing and poses risks for current and future generations. There is a crucial need for evidence-based and culturally appropriate substance use prevention and treatment programs. Afghanistan is making strides in training the treatment provider workforce. Education and treatment coverage have been expanded in urban areas, but there is still a tremendous need for prevention and treatment services in rural areas, where most of the population resides. Afghanistan has been a country that values education and education is needed for all of its citizens, both girls and boys. Thus, investing in universal education that includes literacy and numeracy for all children has the potential to create promise for the country’s future. There is a need to develop socially acceptable skilled and unskilled employment opportunities for both women and men in order to promote economic stability. Another way forward is to integrate skills enhancement training and vocational training with the provision of micro-credit, supported by market surveys and training in accounting. Because the Ministry of Counter Narcotics no longer exists, there is a need for a strong institution to coordinate the cross-cutting issues of counter narcotic activities and the fulfillment Afghanistan’s constitutional obligations. The president’s office should take the lead to effectively coordinate and monitor counter narcotic activities and bring cohesion to government efforts and international aides. Special attention needs to address the production of amphetamine-type stimulants and every effort should be made to prevent this emerging issue as early as possible. To address substance cultivation and problem use in Afghanistan, gender equality and the economy must advance. As the counter narcotic effort is a multi-sectorial issue, there is a crucial need for better coordination among different governmental and non-governmental counterparts. And most importantly, there is a need to concentrate on underlying economic and security issues to help address the substance use problem. By harnessing the economic power of youth and women, Afghanistan has an opportunity to move forward in the fight against substance use.
REFERENCES
- Todd CS, Macdonald D, Khoshnood K, Mansoor GF, Eggerman M, et al. (2012) Opiate use, treatment, and harm reduction in Afghanistan: Recent changes and future directions. Int J Drug Policy 23: 341-345.
- United Nations Office on Drugs and Crime (2006) Afghanistan drug use survey 2005. United Nations Office on Drugs and Crime, Vienna, Austria. Pg no: 1-17.
- United Nations Office on Drugs and Crime (2009) Drug use in afghanistan: 2009 survey executive summary. United Nations Office on Drugs and Crime, Vienna, Austria. Pg no: 1-19.
- SGI Global (2015) Afghanistan national drug use survey. SGI Global, Alexandria, USA. Pg no: 1-24.
- Ministry of Counter Narcotics (2015) Afghanistan Drug Report 2015. Ministry of Counter Narcotics, Kabul, Afghanistan. Pg no: 1-99.
- National Statistics and Information Authority (2019) Afghanistan Statistical Yearbook 2018-19. National Statistics and Information Authority, Kabul, Afghanistan. Pg no: 1-274.
- UNESCO (2020) Enhancement of Literacy in Afghanistan (ELA) Programme. UNESCO, London, United Kingdom.
- Afghanistan Independent Human Rights Commission (2008) Effective factors associated with drug addiction and the consequences of addiction among afghan women. Afghanistan Independent Human Rights Commission, Kabul, Afghanistan. Pg no: 1-26.
- United Nations Assistance Mission in Afghanistan (2018) Reports on women’s rights and the elimination of violence against women. United Nations Assistance Mission in Afghanistan, Kabul, Afghanistan.
- Central Statistics Organization (2017) Afghanistan Demographic and Health Survey 2015. Central Statistics Organization, Kabul, Afghanistan. Pg no: 1-501.
- UNFPA (2014) Afghanistan state of youth report 2014. UNFPA, New York, United States.
- Goldberger BA, Martin DM, Gold M (2010) Opium Smoke: The Study of Second- and Third-Hand Exposure in Women and Children of Afghanistan. NES, Inc., Folsom, California. Pg no: 1-6.
- Squeglia LM, Jacobus J, Tapert SF (2009) The influence of substance use on adolescent brain development. Clin EEG Neurosci 40: 31-38.
- Lubman DI, Yücel M, Hall WD (2007) Substance use and the adolescent brain: A toxic combination? J Psychopharmacol 21: 792-794.
- Catani C, Schauer E, Neuner F (2008) Beyond individual war trauma: Domestic violence against children in Afghanistan and Sri Lanka. J Marital Fam Ther 34: 165-176.
- SAYARA (2017) Evaluation of Afghanistan’s Child Protection Action Network. SAYARA, Kabul, Afghanistan. Pg no: 1-131.
- Momand AS, Mattfeld E, Morales B, Ul Haq M, Browne T, et al. (2017) Implementation and evaluation of an intervention for children in Afghanistan at risk for substance use or actively using psychoactive substances. International journal of pediatrics. Pg no: 1-10.
- United Nations Office on Drugs and Crime (2017) Afghanistan synthectic drugs situation assessment. United Nations Office on Drugs and Crime, Vienna, Austria. Pg no: 1-36.
- TRT World (2019) Afghan president rejects interim government as way forward. TRT World, Be?ikta?, Turkey.
- ICOIC (2004) Constitution of Afghanistan. ICOIC, Kabul, Afghanistan.
- Afghanistan Ministry of Justice (2005) Counter narcotics drug law. Afghanistan Ministry of Justice, Afghanistan. Pg no: 1-55.
- Special Inspector General for Afghanistan Reconstruction (2019) Quarterly report to the United States congress. Special Inspector General for Afghanistan Reconstruction, Virginia, United States. Pg no: 1-27.
Citation: Momand AS, Jones HE (2020) Substance Use among Women and Children in Afghanistan: The Complexities of an Important Public Health Issue. J Addict Addictv Disord 8: 33.
Copyright: © 2020 Abdul Subor Momand, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.