A Rare Case of Benign Osteochondromatous Lesion beneath the 3rd Metatarsophalangeal Joint
*Corresponding Author(s):
Ashish Vinodkumar BatraNewcastle Orthopaedic Foot And Ankle Clinic, Lambton, Australia
Tel:+61 497348579,
Email:ashishbatra13@gmail.com
Abstract
Extra skeletal osteochondroma is a rare benign soft tissue tumor. We report the case of a 50-year-old male who presented with a painful nodular mass in the plantar aspect of his left forefoot. Radiological findings showed ill-defined mineralization centered at the base of the proximal phalanx of third toe with no significant articular erosions or osteoarthrosis at the third MTP joint. Excision biopsy of the nodule was done. The lesion was sent off for histopathology, confirming diagnosis of benign osteochondromatous lesion beneath the left 3rd MTP joint with no evidence of malignancy. Intraoperatively, it was visible that the lesion was exclusively in soft tissue, there was no bony connection. There was no post-operative complication and no signs of relapse on 6 months follow up after surgery. In conclusion, an osteochondromatous lesion should be considered when a distinct, ossified mass is localized in the fibro-connective soft tissues of the distal extremities.
Keywords
INTRODUCTION
Extra skeletal osteochondroma is relatively rare benign soft tissue tumor. It is slow growing and mostly arises within the soft tissues of hands and feet. It presents itself as a small discrete calcified mass that rarely exceeds 2-3cm in its greatest dimension [13,14]. This tumor is not specific to either gender, or many studies show that it mainly occurs in patients that are 20 years or older with peak occurrence during the 3rd and 6th decades [14]. It can present itself in many ways initially. Few osteochondromas develop in an idiopathic manner and it is common to have the lesion in association with trauma [14,15]. Literature also shows that the selesions have developed post radiotherapy in children up to 10 years. Because of its variable and worrisome radiological features and histological presentation, it is usually mistaken for an osteosarcoma [13,14]. Local excision is known as the standard treatment if tumor is symptomatic [16].
We report a case of benign osteochondromatous lesion in the soft tissue on the plantar aspect of the left 3rd MTP joint and proximal phalanx.
CASE REPORT
On examination, he was a fit looking man who walked with a subtle limp. Getting up on tiptoes aggravated his limp. His left forefoot was well-aligned, but he had a hard-nodular mass beneath his 3rd MTP joint. This measured approximately 3 × 2cm. He had associated callus over the lesion on the plantar aspect of his left forefoot. He had an intact sensation and blood supply was satisfactory. His plain radiograph (Figure 1and 2) showed mineralization mimicking heterotrophic ossification centered at the base of the proximal phalanx of third toe with no significant articular erosions or osteoarthrosis at the third MTP joint. This picture was similar to heterotopic ossification in the soft tissues on the plantar aspect of the left 3rd MTP joint and proximal phalanx. It looked consistent with heterotopic bone secondary to trauma, as described. On CT scan (Figure 3A, 3B and Figure 4), there was an area of hyper-density in relation to the lateral aspect of the base of the proximal phalanx of the 3rd toe extending over around a centimeter. Separate to the phalanx and extending laterally between the 3rd and 4th toes and over the plantar aspect of the 3rd toe there was a mixed density calcified/soft tissue mass which in total measured 20mm × 24mm × 19mm. The soft tissue component was mainly medial. It measured 14mm × 14mm. The joint space was intact. There was no other focal abnormality.

Figure 1: X-ray antero-posterior and oblique view of left foot showing abnormal ossification around 3rdMTP Joint.

Figure 2: Lateral view of left foot showing ill-defined mineralization centered at the base of the proximal phalanx of 3rd toe.
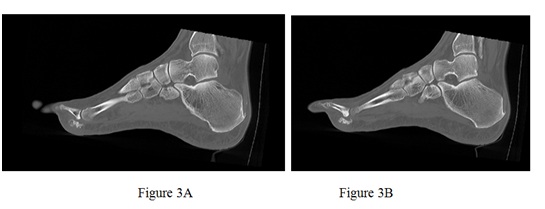
Figure 3: Lateral view of left foot showing ill-defined mineralization centered at the base of the proximal phalanx of 3rd toe.
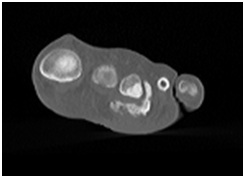
Figure 4: Coronal view of foot at metatarsophalangeal joint level showing hyper dense lesion beneath the 3rd MTP Joint.
On histopathology, sections were reported as benign osteochondromatous lesion within fibro connective tissue. The lesion showed hyaline cartilage, enchondral ossification and bone trabeculae. Many bone trabeculae showed osteoblastic rimming and occasional osteoclastic activity. Vascular congestion and pigment laden macrophages were present. There was no evidence of malignancy. These features were those of an osteochondroma which could be connected to adjacent long bone or purely soft tissue (soft tissue osteochondroma. During his last follow up, which is 6 months post-surgery, there were no signs of local recurrence?
DISCUSSION
Hypothesis that it originates from pluripotent cell lines derived from the joint synovium, tenosynovium, or connective tissue. Another theory states, that it originates from metaplasia tendon sheaths in the hands and feet [1,8,17-21]. There is one more theory, that extraskeletal osteochondroma arises from fibroblasts in the connective tissue distant from bone and joints because of unknown stimuli [21]. Extra skeletal osteochondroma generally presents itself clinically as a painless, slowly enlarging nodular soft tissue mass that is usually present for some time before diagnosis. In 20% patients however, the lesion is painful and tender, especially if located on the plantar side of the foot [14]. A case of a 49-year-old female was reported by Estil JC et al. [14], who had a slow-growing mass of 4 years duration, located on the plantar aspect of her left foot. The mass was slowly becoming more palpable as it increased in size and was progressively causing pain and discomfort during ambulation. Imaging studies revealed an ossified mass bearing no connection to any other structure on the plantar aspect of her foot. An excision biopsy was performed, and the easily dissectible mass, although much larger than its usual presentation, proved to be an extra skeletal osteochondroma. In 2015, Bilgin Y et al. [22], reported the case of a 56-year-old woman with an extra skeletal osteochondroma of the heel. In another case of slow-growing, relatively painful mass on the dorsal side of his right foot, in the 3rd toe web, reported by Kho et al. [23] found that an extraskeletal osteochondroma should be considered when a discrete, ossified mass is localized in the soft tissues of the distal extremities. Although cellular a typia is described on histological examination, there is no known malignant transformation or metastatic lesion. Marginal excision is the recommended treatment of choice, with preservation of the adjacent bone and soft tissue structures. A local recurrence rate of up to 18% has been reported, and such recurrence is best treated with re-excision.
In our present case of benign osteochondromatous lesion, the nodular mass was there beneath the 3rd MTP Joint. The clinic pathological and radiological features of our case excluded the likelihood of myositis, lipomatous lesion, tumoral calcinosis, ossifying fibro myxoid tumor, or malignancy which may present as discrete soft tissue masses. Although mature ossifications generally associated with a benign lesion, sarcomatous lesions such as synovial sarcomas, soft tissue chondrosarcoma and Osteosarcoma can also present with dense calcification and ossification [8]. Thus, close histopathology and clinical correlations are essential to differentiate a chondrosarcoma from an extra skeletal osteochondroma.
In conclusion, an osteochondromatous lesion should be considered when a distinct, ossified mass is localized in the soft tissues of the distal extremities. It has been reported that they have low risk of malignant degeneration. Marginal excision is the recommended treatment, with preservation of the adjacent bone and soft tissue structures.
REFERENCES
- Dahlin DC, Unni KK (1986) Bone tumors: General aspects and data on 8,542 cases, Part 131, 4th (edn). Thomas, Illinois, USA.
- Ozdemir HM, Yildiz Y, Yilmaz C, Saglik Y (1997) Tumors of the foot and ankle: Analysis of 196 Cases. J Foot Ankle Surg 36: 403-408.
- Blitz NM, Lopez KT (2008) Giant solitary osteochondroma of the inferior medial calcaneal tubercle: A case report and review of the literature. J Foot Ankle Surg 47: 206-212.
- Keser S, Bayar A (2005) Osteochondroma of the talar neck: A rare cause of callosity on the foot dorsum. J Am Podiatr Med Assoc 95: 295-297.
- Jackson KR, Gurbani B, Otsuka NY (2004) Osteochondromas of the talus presenting as intraarticular loose bodies: Report of two cases. Foot Ankle Int 25: 630-631.
- Gholamrezanezhad A, Basques K, Kosmas C (2018) Peering beneath the surface: Juxtacortical tumor of bone (part I). Clin Imaging 51: 1-11.
- Gholamrezanezhad A, Basques K, Kosmas C (2018) Peering beneath the surface: Juxtacortical tumors of bone (part II). Clin Imaging 50: 113-122.
- Papagelopoulos PJ, Savvidou OD, Mavrogenis AF, Chloros GD, Papaparaskeva KT, et al. (2007) Extraskeletal chondroma of the foot. Joint Bone Spine 74: 285-288.
- Spencer RJ, Blitz NM (2008) Giant extraskeletal osteochondroma of the plantar mid foot arch. J Foot Ankle Surg 47: 362-367.
- Sheff JS, Wang S (2005) Extraskeletal osteochondroma of the foot. J Foot Ankle Surg 44: 57-59.
- Nakanishi H, Araki N, Mukai K, Ohno H, Matsui Y, et al. (2001) Soft-tissue osteochondroma in the calcaneal pad: A case report. J Foot Ankle Surg 40: 396-400.
- Scarborough MT, Moreau G (1996) Benign cartilage tumors. Orthop Clin North Am 27: 583-589.
- Dahlin DC, Salvador AH (1974) Cartilaginous tumors of the soft tissues of the hands and feet. Mayo Clin Proc 49: 721-726.
- Estil JC Jr, Yeo ED, Kim HJ, Cho WT, Lee JJ (2013) A large extraskeletal osteochondroma of the foot. J Foot Ankle Surg 52: 663-665.
- Chung EB, Enzinger FM (1978) Chondroma of soft parts. Cancer 41: 1414-1424.
- Anthouli-Anagnostopoulou FA, Papachristou G (2000) Extraskeletal chondroma, a rare soft tissue tumor: Case report. Acta Orthop Belg 66: 402-404.
- Aslam MB, Haqqani MT (2006) Extraskeletal chondroma of parotid gland. Histopathology 48: 465-467.
- Gulati Y, Maheshwari A, Sharma V, Mattoo R, Arora D, et al (2005) Extraskeletal osteochondroma of the thigh: A case report. Acta Orthop Belg 71: 115-118.
- Kudawara I, Ueda T, Araki N (2001) Extraskeletal chondroma around the knee. Clin Radiol 56: 779-782.
- Lim SC, Kim YS, Moon YR (2003) Extraskeletal osteochondroma of the buttock. J Korean Med Sci 18: 127-130.
- Singh R, Sharma AK, Magu NK, Kaur KP, Sen R, et al. (2006) Extraskeletal osteochondroma in the nape of the neck: A case report. J Orthop Surg (Hong Kong) 14: 192-195.
- Bilgin Y, Karademir G, Anarat B, Salduz A (2015) Extraskeletal osteochondroma of the Heel: A case report. J Orthop Oncol 1: 101.
- Victor Ka-Siong Kho, Wen-Chih Chen (2010) Extraskeletal osteochondroma of the foot. J Chin Med Assoc 73: 52-55 .
Citation: Batra AV, Sullivan JO (2018) A Rare Case of Benign Osteochondromatous Lesion beneath the 3rdMetatarsophalangeal Joint. J Orthop Res Physiother 4: 038.
Copyright: © 2018 Ashish Vinodkumar Batra, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.