Body Form and Body State, Considered for a Fuller Clinical Framework
*Corresponding Author(s):
Edwin Chau Leung YuHong Kong Institute Of Integrative Medicine, The Chinese University Of Hong Kong, Hong Kong
Email:yuchauleung@gmail.com
Abstract
Former articles have described the gist of the body. The neural, perfusional, and interconnective fascial elements provide the basic adaptive three dimensions in the body since before birth to adulthood as their formation mode each other under similar mechanic-chemico-biological cues into the contextual assembly of the body. With the organ systems operating and self-vitality subsystems adaptively moulding, the individual lives while body form, body state, and body disposition are manifest. For these, there may be irregularities and abnormalities, but the person has the capacity to be snug and fit in living. Defining health or disease depends on sufficiency to live for life’s sake, apart from normality standard for clinician’s sake. Most previous understanding of diseases have concentrated on abnormalities but neglect how the whole person shades from normality shifting to abnormality. With more overlapping findings in health and disease conditions recognized, this paper tries to bridge what is yet not covered in orthodox medicine. A new body map could emerge and diagnosis should more comprehensively bridge these dichotomized normality and naturalistic approaches. The body form and body state is described from its understanding to its deviations and irregularities. The clinical framework is put forward for clinicians not to miss the main four domains. The clinical framework to be more comprehensive should include looking at the disease generally and locally as well as examining the body for the elaborate details in form makeup and body state in terms of a conglomerate profile. Lacking one of these four clinical domains in clinical presentation may greatly bias treatment methods. This understanding would also help developing better therapy modalities and can bridge Chinese and Western Medicine.
Keywords
Body state and form; Chinese medicine; Core regularized vs regulated; Deficit body state; Four domain clinical framework
Introduction
The body view is now well depicted in orthodox medicine. Despite this authenticity, there is in fact a variety of body views when this word body should include the body and mind. Recent research strives to break down the dichotomy between body and mind as arisen since Descartes [1-3] and the brain and body depicted as one organized system [4]. The relation between body and mind and their wholesome integrality is controversial. However, recent papers discussing in simple physiological terms have depicted the body and mind together without separation [5-8]. A new body map could emerge in time to bridge what all along in orthodox medicine suffered for the gaps.
Summarizing features of the complex body map, being too cumbersome, is usually done for a purpose. Diagnosis of a disease is needed orthodoxically, labeling for a problem necessary to package lists for clearer attention even legally, and some for understanding needs a picture. All these need algorithms or methods. Clinically, the assessment is to get a representative picture to proceed to management. Currently, medicine has progressed in many directions. But in fact, and from lesion to complexity treatment, it may variously follow a lesion-based, multi-causal, holistic, or integral approach [5] that necessitate a fuller body map. The complex body mapping for a sharp anatomical or functional lesion, or weighing the many causes, or for a broad dimension of whole problems, or a body state to find the critical impact point is in reality quite different. Amongst the new body mapping, this paper selects the most important two aspects, body form and body state, to describe further.
The Body Form and Body State
The body form, the body state, and the body disposition could comprehensively describe the whole person for how a person lives snug and fit in health or disease [6]. All these may deviate or be deflected throughout the years. As an individual presents oneself to the environment, and the body serves to confront the surrounding with dynamic capabilities, the body form, structure and related functions have developed as one in meeting up with evolutionary living demands. As an individual may develop body compositions variously right for or non-conforming to his own being through life, it really depends on his body form, body state, and body disposition in relatedness to his environment as for whether he lives sufficiently well and effective.
Considering the body form, the human body has arrived to its current external form with its interactive musculoskeletal framework through meeting multiple evolutionary demands as external geometric constraints and mechanical forces in the ecological system have influenced morphogenesis [9,10]. Genetic variations provide substrate for evolutionary adaptivity through flexibility of a population in the face of changing environments. Phenotype consists of observable properties, such as morphology, development, or behavior. In human, genetic variations is not the main cause for phenotypic differences. Human studies have shown that about 90% of genetic variation can be found within diverse populations over the continents; while only about 10% of genetic variation really separates the populations [11,12]. Any two humans may differ on average at only about 1 in 1,000 DNA base pairs (0.1%). Phenotype plasticity is demonstrated by 'the ability of individual genotypes to produce different phenotypes when exposed to different environmental conditions’ [13]. Environmental cues may elicit responses that are mediated by physiological and developmental events [14]. The phenotypic development may be shaped at certain life stages particularly in sensitive periods with a greater impact than other stages [15,16]. While heightened phenotypic plasticity occurs mostly early in life [17], sensitive periods in later developmental stages are also common [18].
Internally, parallel mechanisms evolve to build up a snug internal environment to fit the complex external needs. With the organs and cells supporting operation, the self-vitality subsystems in the whole individual adapting to the body-environment changes [7] depict the body state. The way the individual acts, actuates and reacts is his body disposition.
External Form – mouldability in environments
The tendo-musculo-skeletal elements establish the body form. Function and structure are related and governed by basic underlying stability, control, flexibility and cost-economy. To command domains and terrains, the integrated whole body with axial core strength and stability as well as appendicular locomotor power are essential in actions and actuational endeavors. The body form has developed and varied as it met up with living demands.
For the form to meet the external surroundings, adaptive mouldabilty facilitates functional stability and activity as a dynamic process [10]. Adaptive mouldabilty in the formed parts is allowed even with the rigid chest cage [19], and in the developing parts such as the sacral base of the spine which is not fused until the age of 25–30 years [20,21]; the whole spine being allowed to adjust to postures until twists and turns are settled to fit the individual’s surrounding circumstantial mode of living. Deeper inside, bone shape continues to change in response to load through moulding its internal structure of relatively pliable cartilage and stronger bone ossification changes during development [22]; even in aging [23,24]. At the outermost borderzone, meeting the immediate environment, the skin displays mechanics showing how much it is in a state of complex in-plane heterogeneous tension patterns, which depend on individuals, their age, body location and position [25]. In fact, skin tension lines occur within the skin as a result of growth and remodeling mechanisms [26].
Internal State - remodelling inside out
The internal system of an individual consists of all the hardware organs and overlaying systems and networks in the individual, consciously or subconsciously operating or controlling internal and external flow of messages and operations while subserving every vitality functions and interfaces needed for living. The multi-various internal features are mainly embodied in organ systems. The segregated organs installed in place and the well-recognized organ systems ensure efficient and effective operation of dedicated functions. While the body faces the variable environments throughout life, life-vigor systems are configured over these operating organ systems, adaptively coordinating and remodelling for meeting life processes. In reaction or in anticipation, these systems interact and interrelate to allow the individual to face life for catering needs effectively. Functional modes configure the interplay of organ complexes as some five self-vitality subsystems including the food handling system for acquisition, the situational option-generation system, the cultivated action-for-life system, the saliency allocation-for-endeavor system, and the patternable energy-process driver, together with deep bio-strata. These are summarized in an overview [5], which relates them to similar Zang organs that Chinese medicine describes. They are organized to provide direction and control of adaptive activities, increasing body efficiency, and to strengthen steadfast interfacing of body to environment during activities and challenges through life. As whole body systems, they to a certain extent focus consistencies and in a way build up integrity of the individual as one in life, while frugally minimizing and maximizing energy and resource in balance to output appropriately.
The neural, perfusional, and interconnective fascial elements (NPI) provide the basic adaptive three dimensions in the body [6]. Before birth, their interrelated formation mold each other under similar mechanic-chemico-biological cues as a contextual assembly of the body [8]. After birth, even into adulthood, they form the mutually sustaining matrix responding to surroundings [7,27]. As the individual grows and develops in integral entirety, core responses are well patterned to maintain the person as a whole for a stabilizing core. Since birth, the body is equipped such that the body core can continually match its environment without losing its formation and strength. These comprise righting reflexes [28] and righting behaviors up to oriented grasp of surrounding environment [29-31] stabilized within a mode of righty processes. Righting reflexes externally to return the upright body position and righty behaviors to restore oneself inside out would act instantaneously to core deviations. Since birth, core responses include remodelling mechanisms to return the body in snug positions after engaging in modes to fit the environment [7]. Later in life, well-patterned dynamics of closely associated and coordinated neural and perfusional elements provide body preparedness towards actuational endeavors [6]. All five self-vitality subsystems evolve with continuous remodelling and reorganizational modules as they mature [7] wherewith such repeated remodelling develop further well-patterned dynamics followed by other maturational changes that allow the body core to maintain its firm formation while continually matching its environment.
Final Product - Human Being
The body formation of an individual as the external presentation to the environment confront and fit its variability, while the body mechanisms as the internal representations remain snug and stable in supporting capabilities. Body form grossly looks the same over the human species, and the endowed individual after birth is bounded in a protective and reactive skin mantle towards the surrounding environment. Inside, the whole from embryological development up to the mature structured body with its profile of organs and organ systems is shaped. These structures grossly look the same for body makeup, while the setup of multi-various external and internal features actually contribute to his integral entity. With the organ systems operating and self-vitality subsystems adaptively moulding, the individual lives while body form, body state, and body disposition are manifest. When the body matches and further adaptively moulds itself to the various environments, concomitant biological, psychological and emotional changes occur and may be viewed as reactions expressed out. The body networks develop in rings after rings of build-ups throughout life [32]. Nevertheless, burdens such as minor genetic defects, flaws in the phenotype, and body irregularities exist (Figure 1), such that the body with its constituted phenotypic would function sufficiently well only when these burdens on the body core do not overwhelm the balance to overcome life conflicts. Defining health or disease depends on a normality standard for clinician’s sake and for sufficiency to live for life’s sake.
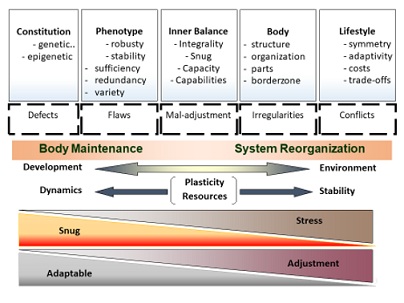 Figure 1: Re-Organizational Burden on the Body Core to Match Environment.
Figure 1: Re-Organizational Burden on the Body Core to Match Environment.
The body poised functionally at the energy-efficient body state tends to achieve snug by autonomously maintaining activities with least stresses. To live effectively and efficiently between dichotomous needs of body energy conservation and expensive output to fit surroundings, the individual automatically set up a mode of living wherewith the body can go over repetitive circumstances by changing just a small extent, and return to the neutral position can be ready and fast. This individual poise consists of the stance externally and the homeostatic mode internally, as these are constantly remodeled. Response modes over repetitive situations would effectively and efficiently tune the concerned body parts to work out the habitual resource allocation, mental preparation, required form changes and internal coordination mechanisms in coping similarly. This body preparedness towards actuation with ready and matching mechanisms to act and react to surrounding variations and disturbances would avoid off-matching and extraneous movements and mental strain that mean unnecessary energy spray and extra costs. Encountering similar situations, adjustments calls for only minor tuning up and least extra input of energy and resources be required. Thereby, the body stays snug and returns to good balance easily. A snug body generally provides further capacity for adaptiveness [6].
Sufficiency to stay well-maintained is of course influenced by resources and demands. Lifestyles affect one's body makeup. Functions served and interactions inside out according to the adequacy or superfluous inputs would determine the makeup or arrangement and organization. Overly demanded, even the body structure would change. Generally, these adaptive changes often occur and incur fixed body changes subtly.
Deviations From Its Primary Constitution
Currently, medicine seeks to define normality by approaches that call in the idea of uniformity of physical and psychological functioning across individuals, and diagnosing any disease requires a standard of reference, which is the state of health or normality [33]. Nevertheless, the biological man displays such variations in form and state manifestation with differences in their magnitude of response to environmental stimuli. Conceptualization of normality can have a naturalistic or normative approach [34]. In this paper, it should probably at this point, forget about defining normality [35] but concentrate on what is abnormal. Before that, one should understand the deviations.
While current medicine seeks to define problems and disease, the whole body should be assessed. Then in addition to linear analysis of disease, the whole body state and matching dynamics should be assessed in a full diagnosis [36] (Figure 2).
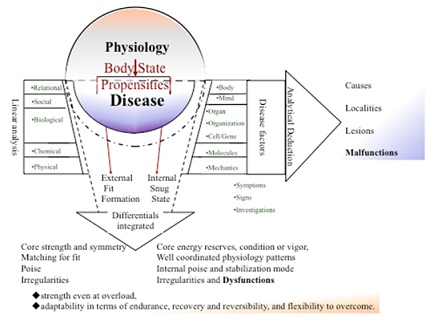 Figure 2: Current medicine seeks to define problems and disease (blue part). Analysis of disease can be done linearly. Yet the whole body should be assessed (whole circle). Both approaches together should be assessed for a full diagnosis.
Figure 2: Current medicine seeks to define problems and disease (blue part). Analysis of disease can be done linearly. Yet the whole body should be assessed (whole circle). Both approaches together should be assessed for a full diagnosis.
Body Form Irregularities
Organisms establish and maintain regularities, patterns of functioning and behaviors in meeting the changing environments and demands of living [37]. Medicine should strive to seek specifications that are objectively preferable for every individual given his or her own biology, environment and mode of life. On the other hand, each individual is constantly changing, and his self and surrounding environment must be in matching modes at often times.
It is in this perspective that deviations be understood before simply labelling whether they are abnormal. The external form grossly looks the same for every individual, but the internal features that contribute to the integral entity are much more multi-various. For the individual entirety, the resilience to environment is first strengthened in early years by endowed biological robustness [38,39]. When this declines through life, it is sustained through maturing well-patterned dynamics [7]. The body always trying to match and once not set would be easily overturned, and also expensive. Yet, over-set and being rigid, body-matching-environment cannot be well done. The body seeks to be regularized. With regularized internal or external environment, regulation becomes easier. Deviations may have arisen from not well regularized or not well regulated so much that the body or life would deviate or be made deviated from an established course or accepted standard.
Over this final product of normality for living, deviations from the original neutral internal or external position can be understood. Confirmation could assess how fast the body can react and how much it can reverse back, and how snug it is and how fit it is. When in time subtle body form and body state are changed, there would need more tools to judge its entangled involvement of other body parts and possible progression. To start with, the core is assessed for simplicity. Finally when things become really abnormal then the clinicians is easy to judge. Stability mechanisms work well to stay good the core. Yet when core deviations are marked, body irregularities would increase and manifest in the body form and the body state.
Body Form irregularities
- Core strength and symmetry with actions and reactions from the periphery is recognized through the effectiveness to perform and overcome tasks and encountering living processes. When core is well maintained as strong and stable, the matching for fit to environment would sustain it and environments would at most deviate it in a trajectory good for life, its poise internally and externally equilibrated, conditioned in right tension, and snug for fit living.
- Irregularities are abnormalities, distortions, malformations and misshapes in the core and peripheral forms that increase susceptibility to poor living and disease outcomes.
Body State irregularities
- The body set state is the setup inside the body at a time and duration of life as the individual stabilizes his body for reacting to the environment [6,7]. Variables contributing to this core state include the individual’s energy reserves, condition or vigor, physiology including metabolic rates, hormone levels, and immune state. With these together well coordinated with good reserves, a robust stabilizing mechanism is installed to react to any expected and unexpected forces from the surroundings. Mechanisms, including body state's energy, memory consolidation, and a stabilization mode worth remodeling on, would build up with reserves to reoptimize the body itself, supporting the core with strength and capacity to meet situations and even stresses with less traumatic confrontations.
- After deviations set in, the body may be moded into a propensity, a tendency to change its setup in the same direction, reoptimizing itself to a different setup. There would be discernable body state change and adaptive state-dependent behaviors or set state-conditioned signs appear.
Decompensated Stage
- As the body continually keeps matching to the surrounding, handling fluctuating levels of variables may not be sufficient to keep for consistency or for core strength and stability. Inadequate reserves and capacity often leads to reduce output for capabilities or to confronting situations with more stresses, which even can becoming traumatic.
- When body form and body state is so maladapted to produce non-snug, non-matching, non-fit outputs, the body loses its homeostatic consistency and becomes decompensated. Stimuli like simple nociceptive stress (mechanical, chemical, thermal, biological) could initiate the process of inflammation. Susceptibility increases. Progress to disease is imminent.
Charactizing Body Form And State Deviations
While a diagnosis from a person's symptoms and signs is made with the medical context, deviations should be characterized with the life context additionally to see its significance. Global and local problems may both exert influence. The core as the center of our body is particularly relevant, functioning to stabilize, though peripheral or local problems sometimes could significantly affect the whole. As far as the body form or body state affect snug and fit dynamics for living and for life or ability to reoptimizing itself, whether it be related to energy reserves, body condition, good reserves, or stabilizing mechanisms, the deviations would be significant.
Form deviations
Form Deviations are related to body vigor or movement. Concerning movements, it is best referenced on a coordinative system between the axial and appendicular orientations. The “core” muscles include many muscles supporting the lumbo-pelvic-hip complex. Core stability may be viewed as the ability to stabilize the spine as a result of pertinent local muscle activity [40]. The pelvis, the thoracic cage, the spine and lower limbs then would together harness for the diversity of human body and locomotor dynamical mechanics with core stability and strength for power to overcome surroundings and terrains.
Concerning body vigor, the skeleto-musculo-fascial structure is an interconnectivity array of differently differentiated connective tissues (CT) with bi-directional muscle-CT communication acts as a continuum of fascia tensile system [8,41]. This endomysial myofascia net reacts as a whole, tuning up and maintaining the stability of the axial-appendicular system for postural patterns strung up. When body vigor is reduced, the whole body stability is recessed.
Form alignment and deviations
These may be evaluated through the individual's performance including posture, acts, actuations, tasks, feats and skills, and it is important to well observe how the body energy and resourcefulness meet and react to these between routines to challenges. --- should be important.
The symmetrical body core tends to display certain degree of asymmetry, and asymmetrical components are common.
In reference to standards, markers such as the degree of twist and deviation curves over the spine, the angles of scapula wings, the opening of the pelvis, as well as others symmetrical surface contour markers would be the prime sites to observe and note for their deviation limits.
In terms of movements, deviations could be viewed under four forms:
- Basic body movements are locomotor, non-locomotor, and actuational movements. The stance, the sway at walking, the symmetry of lift at running, the pose and angles among others should demonstrate their basic dynamics and misdirectional limits. These may seed for core dysfunction.
- Augmentative movements arise with actuational or manipulative movements when the body seeks to augment a focused limited range, thereby instituting an alternative movement pattern to replace the former natural function that might be felt not as effective. The motion segmentation to start with put out a better performance than a natural pose based on its advantageous position threshold. For example, the forward head posture with poking chin, which is too often seen from unduly long computer work, or driving, or carrying heavy backpacks, can be seen particularly in people who are propulsive and assertive to thrust forward their head even in ordinary walking.
- Compensatory movements would be used to achieve fulfillment of functional motor performance when a normal movement pattern is not well present when the naturally endowed neuromuscular action strategy is no longer a viable option for the move [42].
- Lags or lack of movement segments from real loss or started particularly when augmentative movements become so biased that components of the movement patterns of the former natural function are suppressed, limited and scarce.
Assessing degrees
Fundamental movement patterns of an individual that require a balance of mobility and stability, including neuromuscular-motor control may be assessed with the individual placed in extreme positions [43,44]. Those unable to perform the movements for balance of mobility and stability would be deemed utilizing compensatory movement patterns during their activities, even sacrificing efficient movements for inefficient ones in order to perform at high levels.
In terms of snug and fit, the amount of compensatory poses and movements that manifest would demonstrate how the core has deviated or core strength is insufficient. Serious deviations projected up would involve adjacent body parts or extremities, limiting their functional activity and ability to lift, pull, and push weighty objects, and even perform activities of daily living.
Looking for degrees of abnormalities certainly includes the amount of changes in architecture. The symmetry of shoulders would be an easily observable landmark. Elevated shoulders (from overuse or misuse of the shoulders always using that one side to hold objects) is almost certainly an initiator to asymmetry. But notably many have shoulders higher on the left. Uneven shoulders would have a variable significance noting the diaphragm and lung are bigger on the right side than on the left and would influence the shoulder posture and form. However as it exerts pull and shift to the ribcage, and as the rib cage and pelvis work together, the effects follow a similar path to the spine and the spine is rotated or bent. In another example, the one-sided frontal shoulder with the humoral head pushed forward frontally is an augmentative alternative strategy when many individuals having a tendency to push forward. It would screw the scapula and spine in twists which may even end up in subscapularis tear [45] or ipsilateral facial distortions. Also, asymmetrical sports such as tennis, golf, and baseball are especially likely to cause uneven shoulders and postural imbalances. There are of course other causes of uneven shoulders including poor posture, dropped shoulder that even can cause lower cervical radiculopathy [46]. Similarly, peripheral abnormalities such as winged scapula and valgus knees or changes in relative function would be watched, such as observable shifting of knee patella out of place as the leg bends or straightens, where repetitive overuse cause injury with the IT band tight, irritated, or inflamed. Joints of course are observed for their optimum position, and changes during acceleration and deceleration.
Body state deviating integrity assessed
The discernable body state is observed through the manifest features of the body set state as well as understanding comprehensively the energy reserves, condition or vigor, physiology including metabolic rates, hormone levels, immune state, and stabilization mode, thus appreciating the support, strength and capacity of the core. To note, at one time, it was hoped that the advance of the Human Genome Project would solve all the diseases with understanding of gene set for each individual. It was soon observed that relying heavily on genetics could only work out only a monocausal and deterministic understanding of the relationship between genes and disease [47]. On a systemic level, the big data approach of ‘All of Us’ research program (AoU) [48] has been an attempt towards seeking a data set for all body data about intersection of lifestyle, environment and biological make-up as the key to understand diseases and disorders.
As the body core and as a whole act and react in relatedness to environment, adaptive state-dependent behaviors or set state-conditioned signs may be observed, and these may be associated with body state change. These comprise variously the manifestation in skin color changes and complexion, and other consistent features in its informational state when the body confronts and tackles the surroundings.
In brief, the body develops certain tendencies through its poised body state as a propensity, a readiness for certain dispositional aptness. The propensity would be global or local, as the body state tunes to environmental aspects variously including physical, chemical, biological and social contexts. Studies in animals [49] and humans [50,51] have shown that the individual behavior will be different depending on the core body state, with relations to fitness. Personality could emerge as an adaptation to individual differences in core state variables [52-54].
For estimating the body state deviations or irregularities as it meets the surroundings, one may consider choosing a listing of every key and minor changes, or alternatively a mapping of the system characteristics, a more totalistic picture. System biology gives a fair view but not necessary fully related. While omics develop biomarkers to inflammatory or other stress, the list is not necessary totalistic; they may not add up. In this regard, we may enlist Chinese medicine constitution concepts to enhance our understanding to look at propensity. Constitution could be a difficult word to comprehend with current medical science. Nevertheless, analysis of body constitution has been in practice in most complementary and alternative systems of medicine [55-57]. However viewed, it remains a basic concept. General responses to environmental conditions are believed as often related to a combination of physiological, developmental, and behavioral attributes. Therefore, psychotypes or somatotypes were classified in attempts to define their associations and correlations even to pathological conditions. The best known three somatotypes were endomorphy, mesomorphy, and ectomorphy [58]. Western medicine probably frustrated for this pursuit as early attempts to delineate its associations too imprecise. Regardless of the possible confusion over the variety of implication of the word “constitution” [59], the body constitution has been viewed in the past as homeostatic, relatively constant throughout life. In Chinese Medicine (CM), constitution is defined as an integrated, relatively stable and natural specialty of individual in morphosis, physiological functions as well as psychological conditions formed on the basis of innate and acquired endowments in his/her life process, and determines the susceptibility to some pathogenic factors as well as tendency towards pathogenic modes [60].
Body state deviations
Repetitive aggregates of tendencies become a moulding dynamics towards the direction and magnitude of those forces. Sometimes, as in patterns of compensation, this process of re-modeling the body increases inefficiencies and can even lead to injury and/or dysfunction.
An unbalanced CM constitution was found in more than two thirds Chinese general population and the distribution of the unbalanced types between different populations with different gender, age, marital status, occupation, educational level and residential region were significantly different [61].
This so called constitution in fact is the body state with a propensity. It changes in life, unlike the former view of the word as being homeostatic. Its balance was relatively higher in younger people especially soldiers compared with old groups [62,63]. Lifestyle-related unhealthy attitude with alcohol use, drug intake and stress control, were prone to unbalanced body states [64]. Long-term working under noisy environment as in airplane service staffs also can mode the individuals into imbalance body states [65]. Individuals at high cardiovascular risk was assessed on the basis of physical signs, personality, body symptoms, and the susceptibility to environmental changes and body constitutional propensity changes were found associated with physical inactivity, [66]
After all, there can be a clear body state discernable even by any practitioner. It is a deficit state. The body after a long time putting out but not meeting reserves will cause this body deficit, when the middle phalanges are sunken, and when worsened more, the cheeks sunken. This is far different from wasting because the nutritional state is good, and at its early stages the cheek can be plump. This deficit state would reduce energy and often cause mental stress.
Body form and state deviations
While the body state as a propensity is autonomously remodeled and with the individual constantly reconstructing it, body form and state changes often come together in changes, though one may be more obvious. The changes to react to physico-chemico-biological environmental aspects are almost tuned autonomously in an instant or in weeks. Long term life-dispositional changes in body state and body form would occur with committed work or with augmentative actuational life particularly, even affecting the vitality systems.
The body tends to maintain an adapting or positioned suspense with a forwarding stance. Functional stability is a dynamic process. To preserve its integral functionality, the organized unit living in congruity with least incompatibility would be effective and more cost efficient. The internal reactive and anticipatory body responses are trying to establish homeostasis, and at times of extra uncomely demands, regulated as heterostasis, allostasis, hormesis and adaptive homeostasis [67-70]. The body form, body state, and body disposition are interrelated in daily living. Some are more stable and act in support. Some are more adaptable and act and react. In the front end, the individual is facing situations with core and match responses by motive and emotive behaviors. Inside, the body core continually keeps matching to the surrounding, dealing with fluctuating levels of variables for consistency. More and more is now recognized that the body systems are overlapping and the whole system of the body react physiologically and pathologically [4,32]. Functionalities at all body levels catering for demand would affect the whole nervous and perfusion and interconnectivitiy fascia dimensions [7,8]. When the core-vs-match processes and neuro-vascular setup, which ensure one snug to fit in different terrains, become insufficient to continual demands, it calls for for even shifts or new body changes even in constitutional propensities, psychotypes and adaptive structural types.
The shift of body changes off the neutral position of the primary constitution is especially obvious when ageing magnifies the deviating frame. Declining hormones would tend to make up a different body and mind. The pelvises of females begin to constrict in later adulthood [71]. With age, bones tend to shrink in size and density, and together with muscle weakening and poor postures, many people especially women became a bit shorter after the 40s with concomitant curving and twisting of the spine and related twisted muscle layers [72]. The many internal changes led to changes in poise and readiness through the years. Physical forces and changes in the mechanical properties of cells and tissues contribute to development, cell differentiation, physiology, and disease. In response to mechanical demands and biological signaling, bone geometry alters throughout all ages of life [73]. Age-related changes in human trabecular bone architecture include decreased trabecular strength and changes in collagen structure. A shift in the balance to a higher tissue mineral content will generally yield stiffer but more brittle bones. Micro-damages even occur and exponentially extend with age [74,75]. Bone micro-crack with their densities and lengths increase [76] and their propagation broaden with age [77].
Indulgent computer use with related posture problems has led to a lot of achy body deviations. The office environment pushing multitasking works in people with inadequate sleep have stressed and led many mental and neurohumoral changes, even into deficit body states. Derangements in fascial alignment shifted knee and neck as well as spinal curvatures out into ill-snug positions. On the other hand, lags or lack of movement because of inadequate strength from overexertion and sleeplessness or as suppressed by augmentative movements affect form and state reciprocally. The orderly or well-patterned contextual assembly of the three neural, vascular and interconnective fascial dimensions is often altered.
Clinical Significance
Modern health care increasingly emphasizes looking for findings before the body falls into the disease stage. Defining health or disease depends on all along a normality standard for the sake of clinicians. Now one can also use the above according to each individual given his or her own biology, environment and mode of life to also consider health or disease for the sufficiency to live for the sake of patient's life.
Delineating normal or abnormal would depend on the whole body setup. While certain irregularities can be determined as definitely abnormal, many others cannot be judged in isolation. Only with more related parameters together in the body as an integral unit can one determine the significance. Degrees of change would add impact for judging abnormality.
Estimating such in the body formation would be finding out how good the body complexity is organized to cater for living as well as how many elements are deranged and amounting to induce further dysfunctional structures and mechanisms. Not off balance at a moment may not mean poor balance yet to suffer since the capacity or resourcefulness of the body can cover up, or unaligned body parts may shift position and work with a proxy center.
Minor deviations are often ignored as if safely done. The body state and body form should be viewed together clinically. For example, asymmetries are frequent in the body and slighted or neglected until its degree of change (e.g. sustained angle in spine) is believed to predispose to its falling apart. Yet, facial symmetry was found associated with socioeconomic status (SES) in childhood (as it should refer probably to poorer health) [78], while this association became not significant at midlife (as the body state matures stronger). With age, older people mostly are not able to maintain a healthy spinal vertical tilt presentation. Yet, while facial symmetry increases with age [79], symmetrical men when aged experienced less cognitive decline [80-82]. Symmetry may be a reflection of developmental stability in a man’s body and body state strength [83] to support mental capacity.
Handedness and its genetic influences are associated with structural asymmetries of the cerebral cortex [84]. Going further, repetitive heavy use of the body asymmetrically may lead to different scenarios.
The body form and internal organs to start with at early life may look the same for everyone. At later stage of life, the form looks more or less the same, but already often achy with pains. In fact, the body form and formation have changed, only not often observable. There are body irregularities due to change in alignment and concealed blocks or jamming constraints that can be assessable.
Energy support, alignment and other factors useful to assess
Alignment to gravity, work and life integrated: Body asymmetrical components could be a falling off alignment from traction or inherent weakness. Apart from this toppling off, asymmetrical components could be supporting each other and constraining each other as one part of the body initiated the asymmetry. The parting may arise from movements or poise. Sided-dominance in visual dominance or one-sided food chewing would be associated with other asymmetrical supporting components. Simply, asymmetrical parts are not necessarily abnormal.
Over a constantly presenting environment, the neutral position becomes fixed but not necessarily at its original right position. For example, an expert cricket player often has marked body asymmetries. In such rotation sport, asymmetry is developed over the shoulders, in cricketers for pitching, while abdominal asymmetry is produced with greater thickness of obliquus internus abdominis on the non-dominant side. However, when not matched integrally as a whole, symmetry or lack of asymmetry of abdominal muscle is associated with low back pain in cricket fast bowlers [85]. Abdominal muscle morphology is of course symmetrical in the general population. Simply, NORMAL for the population may not be normal for the individual. The whole alignment system is good only when integrated.
While muscle strength asymmetry of lower limbs increases with age, and asymmetry difficult to be ascertained, active individuals showed stronger body composition symmetry than the controls, even in middle-aged and older adults [86,87].
The individual's performance depends on the body energy and resourcefulness: Energy resourcefulness is incipient or potential. In footballers, long term exposure to high-impact gravitational loads to the support limb improves preferentially bone mass and structure, contributing greatly to bone strength relative to the kicking limb exposed mainly to the high-magnitude muscular loads [88]. Energy training makes stronger players even with necessary asymmetry.
Another scenario for body changes is when inadequacies set-in. Aging and declining body state affect body with further firm and state changes. Weakened body may have many more causes. The deficit body state described above even more so.
At the end, stiff or over-compliant myofascial tissue can set in and could influence the magnitude of intermuscular force transmission and may have a significant effect on muscle mechanics [89- 91].
Blocks or constraints: At its best, the maintenance of core symmetry and mobility for sustaining good counterbalance with the surroundings, and the peripheral actuational mechanisms for performing and overcoming tasks and actions should be important. The poise should be regulated as being contingent to ongoing environments. The composing fascia and tendo-musculo-skeletal makeup and setup should be vibrant enough, and the skin and borderzone pliable for adaptive moulding. All in all, the best is that the body tissue and fascia are well connected and organized, the bones well placed, and the skin well spread. When the muscles move well, the whole person will fold and work well, and then the body will be fine and effective.
Locally, blocks and constraints can arise in the fascial-musculo-skeletal makeup even deep down and in the outermost skin. Integration of the bones and muscles is important. Intercalation, tension, positions off, or interrelations unmatched between parts could have significance each by itself, while a strong core may reduce their dysfunctional manifestations. Generally, clinical parameters with increased tissue “tension/density”, positional “asymmetries”, “restricted” mobility, and “tenderness” are simply seen as abnormal. But one should look for earlier signs. The upper limbs for well-aimed movements should be free through the multi-dynamic shoulders. Frontal shoulder being misplaced overtly cause constraints. Decoupling of the thoracic and pelvic through more lumbar vertebrae regions in humans and versatile musculature around the waist endowed for greater mobility in all body planes, allowing a wider adaptive range of biomechanical capabilities [92]. Poor integrated alignment blocks this mobility even in remote parts when longstanding.
The body core would be functioning in optima with conditioned dynamics to produce unstrained effectiveness as well as amenable to restitution, a restoration of proper order. The associated neurohumoral mechanisms and reconditioning patterns formation and adjustments drive as well as stabilize behavior and functional processes for living well. Uncongenial substances inside organ systems or in vessels blocks full function. Cholesterol plaque is one example amongst many. Notably, the fascia penetrates various organs and major functions of CTs include binding and supporting, protecting, insulating, storing reserve fuel, and transporting substances.
Body form, body state, and body disposition in relatedness to environment matters: Having positive effects on daily life activities [93-95], trunk control and core stability is built for being snug especially gained during sitting, standing and lying, while limb locomotion and skill formation are built for being fit to the surrounding environment where ecology factors have more impact [95]. Ill snug cause problems to fit. Mal-fit cause problems leading to ill snug. Snug and fit dynamics are important for living and for life [6,96,97].
Most stresses are borne through the axial skeleton down the pelvis to the lower extremities. A finer spinal control from muscular, neural, and skeletal elements and postural feedback with body energy resourcefulness would be required both for maintaining an upright posture and related diversity of locomotor mechanics. The whole integral person counts.
From snug and fit to mal-snug mal-fit
Looking on body form, ‘vibrancy’ is observed from demonstrating movement efficiency and the range of motions involved in creating given movement patterns as well as significant aerobic or anaerobic ability (i.e., endurance or strength), adaptability to cope with various situations, challenge and balance tests. For the body state, capacity is observed when any great magnitude of change in environment or actuational endeavor is not followed by the necessary internal stress during adaptation involved. The body patterns are well coordinated enough to significantly handle (i.e., endurance or strength), and cope with various challenging situations, challenge and tests. More snug, more fit.
‘Normality’ is effectively clarified after uncovering and evaluating the specific details. For body form, general and local muscular strength, strength imbalance, endurance, and flexibility, particularly noting that muscular endurance are muscle group-specific (e.g. legs for cyclists), and flexibility is joint-specific. Understanding the textural composition and architecture of each locality as well as how functional and agile they act in integrated balance would furnish the full picture and attributes of the body formation. For the body state, apart from general and specific body parameters measured, understanding the textural composition of each system and parts as well as how functional and flexible they act in response would furnish the full picture and attributes of the body state profile. Assessment would need to clarify strength even at overload, adaptability in terms of endurance, recovery and reversibility, and flexibility to overcome.
‘Abnormal’ changes may be global and local, and compensatory positions and patterns may develop. At one end, at the deficit state, the whole body depleted by sleeplessness or wasteful use over long term can be sunken, with form and state affected. Notably the resourceful or depleted body may utilize various righty strategies or compensatory mechanisms or develop alternative workout paths with a different focus. When aged, people may just suffer from the much-retarded ability to return from any change. Slow to get better, easy falling out. A vibrant body certainly can still have local abnormalities.
Judging needs a better framework
Between abnormalities, normality, and vibrancy, there are clearly a lot of overlaps, and clinical signs would particularly be in gray zones. A conglomeration of signs would mark the status better. Somehow, a triviality event of change may make many changes throughout the immeasurable whole. There could be sensitive dependence of the initial conditions particularly when the initial setup is unstable [97]. The compounding impact of a small change can be significant. From the characteristics of the body, including the mode of performance of functions, the activity of metabolic processes, the manner and degree of reactions to stimuli. For integrated alignment, more studies need to be developed in future.
The body at a certain instant would be assessed for its deviations from neutral primary form or constitution, sharpness at adapting to environment, flexibility and capacity to change, and its reversibility back. Notably, body form and state are interrelated in all these matters: how fast it can act and react, does the body to-tally revert back to its neutral, and is it the primary or secondary constitution when neutral. Body disposition also causes constraints.
Whether allowed for by the body or by the poise or by the environment. The body allowed is its capacity: body in deficit or surplus accountable. The poise allowed is its flexibility: the stubborn character and lubricated fascial strength accountable. The environment allowed is its tension: its textural and dynamic stresses accountable. The main determinant is at assessing the body or body-mind in relatedness to environment to evaluate its health and disease status. The interpretational need to relate to environment in essence means more emphasis for understanding coupling system inside out to get parameters that reflect its state of external adaptive mode, the real organization in terms of management science and biological science, the meaning of surplus and depletion in body state, and how the body rise and fall in various compartments particularly the fascial folds. More can be studied on blocks within, and on the displacing causes to discompose form and state as derangements. It shows that one needs to take courage to take in systemic biology concepts such as robustness (maintaining a system despite perturbations), plasticity (shifting between different functional levels), homeodynamics (balancing the effects of ageing) and fragility (increased sensitivity to perturbations) and related concepts – and not just the idea of normality – to capture properties specific to health and disease.
The Full Clinical Framework As For Not To Miss
Principalities now described, methods yet to be expanded. Even though details in the enhanced clinical method need much longer to learn, the use of the above considerations can already help clinical progress and treatment. For example, in COVID infection, rebound is thought simply related to Paxlovid. But notably the rebound cases tend to have body states more fragile [98]. Similarly, long COVID brain symptoms actually resemble sleeplessness or anxiety-depression. Opening through the current framework would enlighten by check-ing if computer games frequency is associated to predispose these patients for such problems, a neglected direction for clinical research.
After the lengthy coverage yet to add more exhaustive details, a framework is summarized to put forward clinically what to watch (Figure 3).
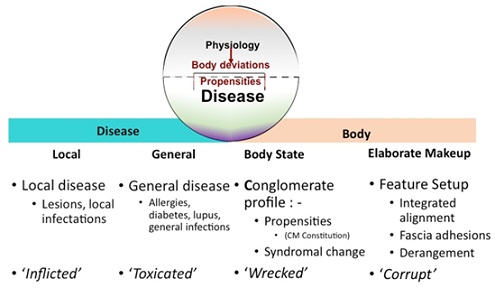 Figure 3: The Four Domain Clinical Framework, not to miss any domain in clinical reports.
Figure 3: The Four Domain Clinical Framework, not to miss any domain in clinical reports.
Four Domain Framework
Find the lesion to see the disease changes: Medicine over the years has rightly emphasized looking for lesions. Clinicians have been used to assess lesions, faulty changes or dysfunctions. A disease as such would then be studied in depth for its pathophysiology. Much has been advanced on details in infection, outer environment, nutrition, genetics, immunity, molecular biology, or the mechanism of disease. The meticulous view comes from understanding of the disorders of the physiological system and the organ system up to molecular views. Allowed an analogy, they may be quoted for one as local ‘Inflictions’.
General diseases are analyzed: These are the disease problems well studied in many directions. Being complex, etiology is generally looked for to simplify the picture. Allergies, diabetes, lupus, infections are thus managed. Allowed an analogy, the complex issues may be quoted under one as generally ‘Toxicated’.
Look at the body whole, Body State: This body state is one aspect this paper tries to bridge for the need to assess as it includes capacity, deviations, reaction modes, energy reserve and deficit budgets, setup, ill- snug and mal-fit functions. The form and state deviations may occur together but assessment should try to weigh their relative impact. State deviations are the conglomerate state displaced to a syndromal malady or pattern. Allowed an analogy, they may be quoted for one as ‘Devastated’.
Look at the Elaborate Makeup of the Body Form: The form commonly assessed may not show much significance. Rather, assessing for form deviations would be clinically useful. Form deviations are assessed particularly for poor alignment, loss of integrated alignment, blocking adhesions and constraints. Given an analogy, they may be quoted for one as ‘Corrupted’.
Clinical framework not to miss any of the four clinical domains
The use of the Four Domain Framework can be understood in some examples. Understanding is enhanced in COVID as described above. In stroke patients, presenting a case well detailing the lesion and associated problem is the usual practice clinically. But in fact not knowing if the patient is wrecked as "devastated", or “corrupted” management would be totally insufficient. Though some may justified that other routine assessment and tests should have covered and shown the issues, yet not all medical personnel would be managing with the same goal united. Only with the full diagnosis covering the disease and the body status could let us concern and concentrate on its entirety and manage correctly.
There are many more such examples to illustrate. The full diagnosis sometimes is simple. But as chronic diseases become common, the framework stands to make clinicians to watch for all four domains.
The body, layer by layer, up to the surface, whether it is in terms of physique, body details, body integrality, or the whole, there are many points that can be noted [5], and as it becomes infinite three-dimensional all the way, so a lot of details are derived [6]. The NPI domains are moulding with body form and body state in relatedness to the environment [8]. The fascia layer with loose tissue and dense tissue is elastic, and fills the whole body as a network of sinewy structures that contribute to stabilization of action platforms to generate power. In general, this fascia structure is often changing, remodelling and energy dependent. So are the neural vascular coupling functionalities. From the outer borderzone, through the middle layer of blood vessels, nerves and fascia that support the inner body and the borderzone layer to interrelate and react to the environment, the body is related to the whole outside world, with a collective response [7]. With the body borderzone related to the whole outside world, with a collective response as outside world interactions transmit cues and information, and with the inner body regulating the outer and inner, temperature and humidity, and monitoring immune stimulants and substrates, allergic reactions, etc, the NPI dimensions would under the influence of gravity, or pulled by one’s own behavior, tune up and work out global and specific needs of the body for the whole situation. The balance adjustment becomes effective from inside out.
There is a perfect order and function of each of them. To list everything not 'normal' would be inefficient and ineffective. This is particularly so for the body concerned, even worse in complex disorders when the body state is perturbed. Yet the body especially its body state would not be depicted just by details that are not totalistic. A picture of it in terms of relatedness to environment could key out important directions for management [2,36].
Whether in snug or fit, the body tarries in health or disease. Body assessment should allow one to see where the body is shattered and wrecked, what displace changes of will power, body quality substantial changes, and deficit states, apart from seeing if there is any abnormality, imbalances, excess or deficit. The four domain clinical framework is the primary coverage for clinical reports.
References
- René DR, Florent SF, Homine D (1662) Apud Franciscum Moyardum & Petrum Leffen. Open Library, USA.
- Zhuang P (2020) A Comparative Study of Views on Body Between Traditional China and the West — with comments on comparison between Merleau-Ponty and Mencius. Revue de littérature comparée 376: 461-470.
- Liu S, Zhu JJ, Li JC (2021) The interpretation of human body in traditional Chinese medicine and its influence on the characteristics of TCM theory. The Anatomical Record 304: 2559-2565.
- García IP, Parada FJ (2020) Measuring the Brain-Gut Axis in Psychological Sciences: A Necessary Challenge. Frontiers in Integrative Neuroscience 13: 73.
- Yu ECL (2020) From Body Mantle to Internal Core - a Parallel Framework to Organ Systems. J Altern Complement Integr Med 6: 129.
- Yu ECL. (2021) From Core and Mantle to Primary Integrality - A Brief Introduction of the Fit and Snug States. J Altern Complement Integr Med 7: 177.
- Yu ECL (2021) Neuro-vascular reserve in developing snug and fit buildup. J Integ Med 10: 49-59.
- Yu ECL (2021) Body NPI Dimensions, the Neural, Perfusional, and Interconnective Matrix. ACAM 9: 71-78.
- Tarannum N, Singh R, Woolner S (2022) Sculpting an Embryo: The Interplay between Mechanical Force and Cell Division. J Dev Biol 10: 37.
- Yu ECL, Wong K (2022) Mouldability of the Body Core in Adaptive Form. J Altern Complement Integr Med 8: 222.
- Jorde LB (2019) Genetic Variation and Human Evolution.
- Sforza LLC, Menozzi P, Piazza A (1994) The History and Geography of Human Genes. Princeton University Press, Princeton, USA.
- Pigliucci M, Murren CJ, Schlichting CD (2006) Phenotypic plasticity and evolution by genetic assimilation. J Exp Biol 209: 2362-2367.
- Fusco G, Minelli A (2010) Phenotypic plasticity in development and evolution. Philos Trans R Soc Lond B Biol Sci 365: 547-556.
- Bateson P (1979) How do sensitive periods arise and what are they for? Anim Behav 27: 470-486.
- Fawcett TW, Frankenhuis WE (2015) Adaptive explanations for sensitive windows in development. Front Zool 12: 3.
- Durnam LG, McLaughlin KA (2020) Sensitive periods in human development: charting a course for the future. Cur Opin Behav Sci 36: 120-128.
- Walasek N, Frankenhuis WE, Panchanathan K (2022) An evolutionary model of sensitive periods when the reliability of cues varies across ontogeny. Behav Eco 33: 101-114.
- Masharawi Y, Rothschild B, Dar G, Peleg S, Robinson D, et al. (1976) Facet orientation in the thoracolumbar spine: Three-dimensional anatomic and biomechanical analysis. Spine Phila Pa 29: 1755-1763.
- Tondury G (1970) Angewandte und Topografische Anatomie.Stuttgart: Thieme, USA;
- Vleeming A, Schuenke MD, Masi AT, Carreiro JE, Danneels L, et al. (2012) The sacroiliac joint: an overview of its anatomy, function and potential clinical implications. J Anat 221: 537-567.
- Berendsen AD, Olsen BR (2015) Bone development. Bone 80: 14-18.
- Boskey AL (2010) Coleman R. Aging and bone. J Dent Res 89: 1333-1348.
- Boskey AL, Imbert L (2017) Bone quality changes associated with aging and disease: a review. Ann N Y Acad Sci 1410: 93-106.
- Limbert G (2017) Mathematical and computational modelling of skin biophysics: a review. Proc R Soc A 473: 20170257.
- Pawlaczyk M (2013) Age-dependent biomechanical properties of the skin. Postepy Dermatol Alergol 30: 302-306.
- Andreone BJ, Lacoste B, Gu C (2015) Neuronal and vascular interactions. Annu Rev Neurosci 38: 25-46.
- Yu ECL (2020) CORE-vs-MATCH MODEL for Autism and Neuro-Developmental Disorders. J Paediatr Neonatol 2: 112.
- Yu ECL (2019) Salient Grasp of Situations as a Mechanism Against Stress for Zang Liver. Chinese J Med Res 2: 27-30.
- Wright CE, Marino VF, Belovsky SA, Chubb C (2007) Visually guided, aimed movements can be unaffected by stimulus–response uncertainty. Exp Brain Res 179: 475-496.
- Perry CJ, Sergio LE, Crawford JD, Fallah M (2015) Hand placement near the visual stimulus improves orientation selectivity in V2 neurons. J Neurophysiol 113: 2859-2870.
- Yu ECL (2020) Developing Autism, The Parts Become The Whole. Scholars' Press. USA.
- Amador E (1975) Health and Normality. JAMA 232: 953-955.
- Rudnick A (2000) The ends of medical intervention and the demarcation of the Normal from the pathological. J Med Philos 25: 569-580.
- Catita M, Águas A, Morgado P (2020) Normality in medicine: a critical review.Philos Ethics Humanit Med 15: 3.
- Yu ECL (1998) The basic clinical diagnostic framework synergized. Review articles. Chinese Medical Journal 111: 460-465.
- Canguilhem G (1943) Le normal et le pathologique. Presses Universitaires de France, France.
- Whitacre JM (2012) Biological robustness: paradigms, mechanisms, and systems principles. Front Genet 3: 67.
- Sokac AM (2019) Mechanical Networks Have Robustness Built into Their Topology, Too. Developmental cell 50: 527-528.
- Faries MD, Greenwood M (2007) Core training: stabilizing the confusion. Strength Cond J29: 10-25.
- Dieter B, Huang Y, Gabor T, Sun L (2019) Continuum linking bone and myofascial bag for global and local body movement control on Earth and in Space. A scoping review. Reach 15: 100030.
- Metzger AJ, Dromerick AW, Holley RJ, Lum PS (2012) Characterization of compensatory trunk movements during prosthetic upper limb reaching tasks. Archives of physical medicine and rehabilitation 93: 2029-2034.
- Cook G, Burton L, Hoogenboom BJ, Voight M (2014) Functional movement screening: the use of fundamental movements as an assessment of function - part 1. Int J Sports Phys Ther 9: 396-409.
- Cook G, Burton L, Hoogenboom BJ, Voight M (2014) Functional movement screening: the use of fundamental movements as an assessment of function-part 2. Int J Sports Phys Ther 9: 549-563.
- Yu ECL, So TH (2022) Chinese-Western Interplay (ed.2): 171-173. ISBN 978-988-8484-76-8.
- Latif AAA (2011) Dropped Shoulder Syndrome: A Cause of Lower Cervical Radiculopathy. J Clin Neurol 7: 85-89.
- Zwart H (2007) Genomics and self-knowledge: Implications for societal research and debate. New Genetics and Society 26: 181-202.
- NIH Partners With 14 Community Groups (2017) Healthcare Associations on Outreach for All of Us Program. GenomeWeb, USA.
- Sih A, Mathot KJ, Moirón M, Montiglio P, Wolf M, et al. (2015) Animal personality and state–behaviour feedbacks: a review and guide for empiricists. Ecol Evol 30: 50-60.
- Schiralli K, Brazil K, Franklin P, Spadafora N, Jbouri EA (2019) Evolutionary personality psychology. In Encyclopedia of Evolutionary Psychological Science 1-13.
- Me?edovi? JM (2020) Big Five traits as (mal)adaptive behavioural responses to harsh and unpredictable environment: Further evidence for the state dependent evolution of personality. Psihološka istraživanja 23: 23-41.
- Wolf M, Weissing FJ (2010) An explanatory framework for adaptive personality differences. Phil Trans R Soc B 365: 3959-3968.
- Dingemanse NJ, Wolf M (2010) Recent models for adaptive personality differences: a review. Phil Trans R Soc B 365: 3947–3958
- Biro PA, Stamps JA (2008) Are animal personality traits linked to life-history productivity? Trends Ecol Evol 23: 361-368.
- Muthiah K, Ganesan K, Ponnaiah M, Parameswaran S (2019) Concepts of body constitution in traditional Siddha texts: A literature review. J Ayurveda Integr Med 10: 131-134.
- Shura ANA (2020) Diagnosing using Chinese medicine methods. Advanced Hematology in Integrated Cardiovascular Chinese Medicine 3: 97-104.
- Sun Y, Zhao Y, Xue AS, Chen JP (2018) The theory development of traditional Chinese medicine constitution: a review. J Trad CM Sci 5: 16-28.
- Sheldon WH, with Stevens SS, Tucker WB (1940) The Varieties of Human Physique. Harper and Brothers, USA.
- Pivnicki D (1964) A consideration of constitutional concepts. Psychiatric Quaterly 38: 346-689.
- Wang Q (2005) Traditional Chinese Medicine Constitutionology. People’s Medical Publishing House, Beijing, China.
- Wang Q, Zhu YB (2009) Epidemiological investigation of constitutional types of Chinese medicine in general population: base on 21 948 epidemiological investigation data of nine provinces in China. J Tradit Chin Med Pharm 24: 7-12.
- Guo JS, Chen SW, Bai J (2012) Investigation and analysis on the types of traditional Chinese medicine constitution of 924 cases of military pilots. J Basic Chin Med 18: 675-678.
- Zhou DF (2010) Experience of Professor Minghui Yang in Treating Latent Disease. Chinese PLA General Hospital & Postgraduate Medical School, China.
- Yang Y, Xu H, Liu QS (2011) The lifestyle of health/sub-health status and the effect to Chinese constitution in urban residents. Chin Arch Tradit Chin Med 29: 1963-1966.
- Ma XY, Chen JS, Gao SL, et al. (2012) Investigation and analysis on TCM constitution of military airplane service staff in longterm noisy environment. Clin J Med 40: 683-685.
- Wang Y, Wu XY, Wang HHX, Li YT, Fu Y, et al. (2021) Body Constitution and Unhealthy Lifestyles in a Primary Care Population at High Cardiovascular Risk: New Insights for Health Management. Int J Gen Med 14: 6991-7001.
- Sterling P (2012) Allostasis: A model of predictive regulation. Physiology & Behavior 106: 5-15.
- Mattson MP, Calabrese EJ (2014) Hormesis: what it is and why it matters. In: Mattson MP, Calabrese EJ (Eds,), Hormesis: A Revolution in Biology, Toxicology and Medicine. Humana Press Inc., USA.
- Davies KJA (2016) Adaptive homeostasis. Mol Aspects Med 49: 1-7.
- [70] Fontana L, Atella V, Kammen DM (2013) Energy efficiency as a unifying principle for human, environmental, and global health. F1000 Res 2: 101.
- [71] Huseynov A, Zollikofer CP, Coudyzer W, Gascho D, Kellenberger C, et al. (2016) Developmental evidence for obstetric adaptation of the human female pelvis. PNAS, 113: 5227-5232.
- [72] Walston JD (2020) Common clinical sequelae of aging. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th Philadelphia, PA: Elsevier; chap 22.
- Goldman HM, McFarlin SC, Cooper DM, Thomas CD, Clement JG (2009) Ontogenetic patterning of cortical bone microstructure and geometry at the human mid-shaft femur. Anat Rec (Hoboken) 292: 48-64.
- Schaffler MB, Choi K, Milgrom C (1995) Aging and matrix microdamage accumulation in human compact bone. Bone 17: 521-552.
- Ferlengez ZS, Kennedy OD, Schaffler MB (2015) Bone microdamage, remodeling and bone fragility: how much damage is too much damage? Bonekey Rep 4: 644.
- Vashishth D. (2007) Hierarchy of bone microdamage at multiple length scales. Int J Fatigue 29: 1024-1033.
- Currey JD, Brear K, Zioupos P (1996) The effects of ageing and changes in mineral content in degrading the toughness of human femora. J Biomech 29: 257-262.
- Hope D, Bates T, Penke L, Gow AJ, Starr JM, et al. (2013) Symmetry of the face in old age reflects childhood social status. Econ Hum Biol 11: 236-244.
- Linden OL, He JK, Morrison CS, Sullivan SR, Taylor HOB (2018) The Relationship between Age and Facial Asymmetry. Plast Reconstr Surg 142: 1145-1152.
- Bates TC (2007) Fluctuating asymmetry and intelligence. Intelligence 35: 41-46.
- Penke L, Bates TC, Gow AJ, Pattie A, Starr JM, et al. (2009) Symmetric faces are a sign of successful cognitive aging. Evol Hum Behav 30: 429-437.
- Brown WM, Usacka A (2019) The Face of Early Cognitive Decline? Shape and Asymmetry Predict Choice Reaction Time Independent of Age, Diet or Exercise. Symmetry 11: 1364.
- Dongen SV, Gangestad SW (2011) Human fluctuating asymmetry in relation to health and quality: A meta-analysis. Evol Hum Behav 32: 380-398.
- Sha Z, Pepe A, Schijven D, Castillo AC, Carrión-Castillo A, Roe JM, et al. (2021) Handedness and its genetic influences are associated with structural asymmetries of the cerebral cortex in 31,864 individuals. PNAS 118: 211309511.
- Gray J, Aginsky KD, Derman W, Vaughan CL, Hodges PW (2016) Symmetry, not asymmetry, of abdominal muscle morphology is associated with low back pain in cricket fast bowlers. J Sci Med Sport 19: 222-226.
- Stagi S, Moroni A, Cremasco MM, Marini E (2021) Body Composition Symmetry in Long-Term Active Middle-Aged and Older Individuals. Int J Environ Res Public Health 18: 5956.
- Trivers R, Fink B, Russell M, McCarty K, James B, et al. (2014) Lower Body Symmetry and Running Performance in Elite Jamaican Track and Field Athletes. PLoS ONE 9: 113106.
- Hart NH, Nimphius S, Weber J, Spiteri T, Rantalainen T, et al. (2016) Musculoskeletal Asymmetry in Football Athletes: A Product of Limb Function over Time. Med Sci Sports Exerc 48: 1379-1387.
- Smeulders MJ, Kreulen M (2007) Myofascial force transmission and tendon transfer for patients suffering from spastic paresis: a review and some new observations. J Electromyogr Kinesiol 17: 644-656.
- Yucesoy CA, Huijing PA (2007) Substantial effects of epimuscular myofascial force transmission on muscular mechanics have major implications on spastic muscle and remedial surgery. J Electromyogr Kinesiol 17: 664-679.
- Huijing PA, Voermans NC, Baan GC, Busé TE, Engelen BG, et al. (2010) Muscle characteristics and altered myofascial force transmission in tenascin-X-deficient mice, a mouse model of Ehlers-Danlos syndrome. J Appl Physiol 109: 986-995.
- Schilling N (2011) Evolution of the axial system in craniates: Morphology and function of the perivertebral musculature. Front Zool 8: 4.
- Haruyama K, Kawakami M, Otsuka T (2017) Effect of core stability training on trunk function, standing balance, and mobility in stroke patients. Neurorehabil Neural Repair 31: 240-249.
- Valdés RC, Calafat CB, Farrés MG, Gómez FMC, Valiño MH, et al. (2015) The effect of additional core stability exercises on improving dynamic sitting balance and trunk control for subacute stroke patients: a randomized controlled trial. Clin Rehabil 30: 1024-1033.
- Ting LT, Jie LM, Qian LY, Na ML, De JC (2018) Effects of core stability exercise on rehabilitation in stroke patients with hemiplegia: a meta-analysis. TMR Non-Drug Therapy 1: 41-52.
- Jones KE, Benitez L, Angielczyk KD, Pierce SE (2018) Adaptation and constraint in the evolution of the mammalian backbone. BMC Evol Biol 18: 172.
- Lorenz EN (1963) The Predictability of Hydrodynamic Flow. Transactions of the New York Academy of Sciences 25: 409-432.
- Yu ECL (2022) HKCPF Scientific Talk - Chinese medicine in combating COVID 19 infection.
Citation: Yu ECL (2022) Body Form and Body State, Considered for a Fuller Clinical Framework. J Altern Complement Integr Med 8: 287.
Copyright: © 2022 Edwin Chau Leung Yu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.