Clinical Characterization of the Pilot Sample of an Online Short-Term Therapy for Internet Use Disorder
*Corresponding Author(s):
Lara BasenachDepartment Of Education And Psychology, Freie Universität Berlin, Habelschwerdter Allee 45, 14195 Berlin, Germany
Email:l.basenach@start-ptc.de
Abstract
Rationale: Internet Use Disorders are associated with substantial intraindividual and societal impairments. For the treatment of addictive online behaviors, a novel online short-term therapy was implemented and embedded in the randomized controlled trial Stepped Care Approach for Problematic Internet use Treatment (SCAPIT; ID: DRKS00025994). Although data collection for the SCAPIT study is ongoing, baseline data collected from the pilot sample of an online short-term therapy were analyzed to provide preliminary information on clinical characteristics of treatment recipients.
Methodology: Data collection was conducted via an eCRF (electronic Case Report File). The German version of the compulsive internet use scale (CIUS) was applied in order to assess symptomatology of Internet Use Disorder. Sociodemographic data, psychopathological and intraindividual characteristics from the pilot sample (N = 20) of the SCAPIT online short-term therapy were descriptively examined and correlations with symptoms of Internet Use Disorder were analyzed.
Results: Recorded symptom severity of Internet Use Disorder (MCIUS= 36.30; SDCIUS = 6.4) was high and the majority exhibited psychopathological comorbidity (n = 14; 70.0%).Video and Streaming Use Disorder (n = 7; 35.0%) and Social Network Use Disorder (n = 7; 35.0%) were the most prevalent manifestations of behavioral addictions.
Discussion: Findings proof feasibility of online intervention for Internet Use Disorder and provide valuable information regarding clinical characteristics of recipients of a novel online treatment approach. Based on the clinical characterization, challenges in the treatment of behavioral addictions are outlined and implications for online interventions are discussed.
Keywords
Clinical characterization; Internet use disorder; Online therapy
Introduction
The use of internet applications and contents can manifest in dysfunctional, time-expanding behaviors associated with widespread negative impairments [1] and decreased well-being [2]. In absence of a standard nomenclature for disorders due to addictive online behaviors, the term Internet Use Disorder (IUD) has been suggested [3]. The umbrella term includes disorders related to the use of online computer games, online gambling, social networking platforms, online pornography and shopping platforms, as well as nonspecific behavioral addictions predominantly performed online [3].
In the 11th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-11), Gaming disorder (F6C51), analogous to Gambling Disorder (F6C50) was listed in the category for disorders due to behavioral addictions, distinguishing between exclusively or predominantly online and offline behaviors [4]. Other manifestations of IUD have not previously been included in the clinical nomenclature as distinct disorders [5]. Nevertheless, in terms of dependency potential and associated impairments of psychosocial functioning, substantial evidence is emerging for Social Network Use Disorder, Pornography Use Disorder (predominantly online), and Shopping Disorder (predominantly online) [6]. These online addictions can be assigned to the category for other (un) specified disorders due to addictive behaviors (F6C5Y).
The introduction of a category for disorders due to behavioral addictions in ICD-11 highlights the recognition of the clinical significance and the associated aversive consequences at both individual and societal levels [4]. The SARS-CoV-2 crisis accompanied by pandemic-related deprivations, appears to have created societal conditions that potentiated the risk for manifestations of online behavioral addictions for vulnerable groups [1,7,8]. Thus, distinct increase in online activities [7,9,10] and addictive online behaviors was noted under the impact of the SARS-CoV-2 pandemic [11]. Further, results of a recent study on links between IUD and well-being further highlighted, that enhanced internet use due to SARS-CoV-2 pandemic elevated levels of IUD and, in turned, resulted in decreased well-being [2]. Consequently, the clinical significance of IUD and associated public health implications appear to have intensified among deprivations of the SARS-CoV-2 pandemic [7]. However, the widespread expansion of online activities and resulting improvements in digital literacy due to the pandemic may facilitate access to digital health resources, providing important new digital opportunities for preventive and therapeutic interventions. Therefore, an expansion of psychosocial services appears to be appropriate in order to comprehensively establish digital interventions and to create low-threshold access pathways for those affected by IUD [8].
The randomized, two-arm, parallel-group, observer-blind trial Stepped Care Approach for Problematic Internet use Treatment (SCAPIT; German: SCAVIS) is designed to empirically evaluate online-based, severity-adapted interventions for a functional use of the internet (ID: DRKS00025994). Embedded in the SCAPIT research project is an online-based short-term therapy for the treatment of IUD, which is based on a standardized manual of behavioral therapy for computer game and internet addiction [12,13]. As part of the scientific monitoring of the pilotphase of the online short-term therapy for IUD, a clinical characterization of the recipients was conducted. The pilot phase sample comprised the first 20 participants enrolled in the online short-term therapy. Sociodemographic data, psychopathological and intraindividual characteristics from the pilot sample of SCAPIT online short-term therapy were descriptively investigated and correlates with symptomatology of IUD were analyzed. Sociodemographic data comprise age, gender, marital status, ethnicity, educational/vocational/academic background, professional activity. Intraindividual parameters included self-efficacy experience and compulsivity. At the psychopathological level, comorbid mental disorders, level of depression, symptoms of social phobia along with affectivity and impairments of psychosocial functioning were recorded. Regarding behavioral addictions, symptomatic severity of IUD, preference for internet-enabled medium and onset of online activity over the life time were surveyed.
Ethics
The SCAPIT study was positively reviewed by the ethics committees of the University of Lübeck (reference: 21-068), the Freie Universität Berlin (reference: 015.2021) and the ethical camber Rhineland-Palatine Mainz (reference: 2021-15907). Study-related changes were submitted in form of amendments to the ethics committees of the consortium centers. All participants have previously consented in writing to general processing of the data collected.
Methodology
- Sample acquisition
The nationwide acquisition of the pilot sample took place from October 2021 to January 2023, embedded in the SCAPIT study. Due to the pandemic-related constraints, the targeted terrestrial acquisition was largely transferred to the online setting. Posts and videos were shared in online platforms such as Instagram, Facebook, YouTube, and Twitter in order to educate about addictive internet use and motivate interested individuals to participate in the SCAPIT study. In cooperation with an association of statutory health insurance companies, further recruitment activities included articles in member magazines, lectures and presentations at health days, in which company employees were informed about the content and procedure of the SCAPIT study. Moreover, recruitment included newspaper articles, radio and television, as well postings and clips of influencers. In addition, affected individuals with symptoms of IUD who sought psychotherapeutic help in the participating clinical consortium centers were recruited.
- Inclusion/exclusion of participants
The pilot phase sample comprised the first 20 participants included within the online short-term therapy. The online stepped care approach, provided via the smart@net app, contains a screening, and a subsequent assignment to a prevention or an intervention module [14]. To be eligible for participation in the in the SCAPIT study, prospective study participants were required to provide digital informed consent within the smart@net app, be aged between 16 and 67 years, and have a smartphone. Study participants scoring ≥ 21 points on the Compulsive Internet Use Scale (CIUS; [15]) in the app-based screening, were randomly assigned to intervention or control condition, respectively. The intervention module included stepped interventions according to the severity of pathological internet use. Further information on the SCAPIT study procedure can be found in the study protocol [14].
Participants in the intervention condition were included in the pilot sample of online short-term therapy if one of the two conditions were fulfilled: (1) Lack of success in the previous intervention module 2 of the stepped care approach in terms of a CIUS score ≥ 21 and presence of 3 criteria for disorders due to predominantly online behavioral addictions sensu DSM-5 or one criterion sensu ICD-11, a clinically treatable symptomatology defined as5 criteria for disorders due to predominantly online behavioral addictions sensu DSM-5 or 3 criteria sensu ICD-11. (2) The presence of at least 6 criteria for disorders due to predominantly online behavioral addictions sensu DSM-5 also resulted in immediate enrollment in the pilot phase of online short-term therapy [14]. Inclusion in the pilot phase sample further required a public health insurance and the submission of the following signed documents: Treatment contract, therapy contract and treatment objective agreement, confidentiality statement. Access pathways to the pilot phase of online short-term therapy are presented in figure 1.
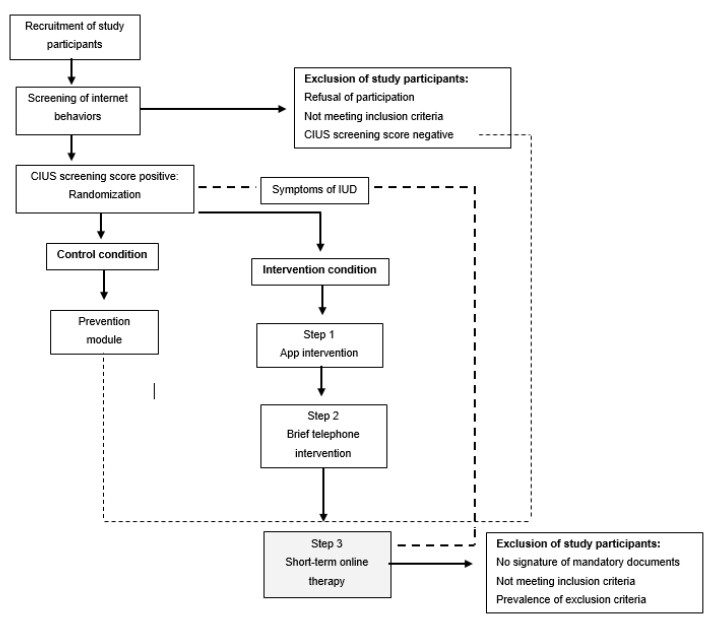 Figure 1: Flow chart of access pathways to the pilot phase of online short-term therapy (in accordance with [14]).
Figure 1: Flow chart of access pathways to the pilot phase of online short-term therapy (in accordance with [14]).
Language barriers that may interfere with understanding of the intervention content and a receipt of (psycho) therapeutic help within the last 4 weeks led to exclusion from the pilot sample. Further, the following exclusion criteria were defined a priori: Unstable psychopharmacotherapy, modification of psychotropic medication dosage in a period of 17 weeks before or during the piloting phase, seeking therapeutic treatment, distinct impairment in global functioning (GAF score < 40), presence of a depressive episode according to BDI-II score ≥ 26, or diagnosis of alcohol/drug dependence, borderline/antisocial/schizoid or schizotypal personality disorder, schizophrenia, schizoaffective/ bipolar disorder, and organic mental disorder. If one of the specified disorders has been diagnosed in the course of life and is not accompanied by an ostensible symptomatology at the current time, inclusion in the pilot phase may be possible after a careful examination of the patient's ability to receive the treatment. Signs of suicidality or acute crisis situations also caused exclusion from the pilot sample, as the online-based implementation of the therapy prevented immediate personal support in emergency situations. Indications of the presence of an exclusion criterion, such as a BDI-II sum score ≥ 26, justified a detailed case discussion, under the supervision of HS and KW.
- Data collection
Data analysis focused on the first survey time point at the beginning of the pilot phase of the online short-term therapy. A comprehensive baseline diagnostic assessment was performed to screen for possible exclusion criteria and to ensure referral to an alternative treatment setting in case of severe comorbidities. Therefore, participants in the pilot phase received a test psychological diagnostic procedure in form of a standardized electronic Case Report File (eCRF). The online-based survey was encrypted and pseudonymized on the basis of an Identification Number (ID), which enabled the data to be clearly assigned. The encrypted eCRF was sent during the first individual session via the video-based therapy platform viomedi.de to enable data protection-compliant transmission. In addition, the global level of functioning of the recipients was evaluated with an expert rating by the treating clinician.
- Survey instruments
The eCRF comprises the German versions of self-report measures. An overview of all survey measures and data collection points is presented in the study protocol [14]. The survey instruments included in the analysis are listed in table 1, comprising the following dimensions: Symptom severity of IUD and behavioral data of internet use, depression, anxiety and social phobia symptomatology, affectivity, self-efficacy expectancy, compulsivity, comorbid psychopathologies. Symptomatology of IUD was assessed using the German version of the Compulsive Internet Use Scale (CIUS; [15,16]). The self-report instrument measures core elements of internet addiction with 14 items including the following symptom domains: Loss of control (items 1, 2, 5, and 9), withdrawal (item 14), coping (items 12 and 13), mental and behavioral capture (items 4, 6, and 7), inter- and intrapersonal conflicts (items 3, 8, 10, and 11). Item responses are based on a five-point Likertscale (0: Never, 1: Rarely, 2: Sometimes, 3: Often, 4: Very often), resulting in a total score of between 0 and 56 points. Validation studies demonstrate high internal consistency (Cronbach's α = 0.87 - 0.89) of the instrument [16,17]. The AICA-S, evaluated by Wölfling and colleagues [18], was applied as an additional instrument to survey online activities, the most intensively used internet medium, and the number of years for which the internet has been used. Recorded online activities contained the following: Gaming, shopping, chatting, writing e-mails, pornography, gambling, communities, information research, (video) streaming. The self-report instrument showed high internal homogeneity (Cronbach's α= .88; [19]).
|
Title (Author, year) |
Brief description of the instrument |
|
CIUS [16] |
14 items to address symptom severity of problematic internet use. |
|
AICA-S [18] |
15 items to assess internet use behavior and symptoms of IUD. |
|
BDI-II [20] |
21 items to measure severity of depressive symptoms. |
|
SCL-90-R Subscale: Compulsivity [21] |
10 items to survey compulsivity. |
|
LSAS [22] |
24 items, divided into subscales (avoidance; fear), to elicit extent of social phobia. |
|
SWE [23] |
10 items for screening self-efficacy expectancy. |
|
PANAS [24] |
10 items each on dimensions of positive and negative affectivity. |
|
PHQ-D [25] |
Assessment of the following mental disorders: somatoform disorders, affective disorders, anxiety disorders, eating disorders (bulimia nervosa; binge-eating disorder) and alcohol abuse. |
Table 1: Applied self-report instruments.
Notes: CIUS = Compulsive Internet Use Scale; AICA-S = Assessment for Computer game and Internet Addiction; BDI-II = Becks Depression Inventory; SCL-90 R = Symptom Checklist-90 Revised; LSAS = Liebowitz Social Anxiety Scale; SWE = Self-Efficacy Scale; PANAS = Positive and Negative Affect Schedule; PHQ-D = Patient Health Questionnaire.
Additionally, the German version of the Global Assessment Scale of Function (GAF; [26]) was applied to assess psychosocial functioning levels. The GAF scale is divided into 10 levels to measure psychological, social, and occupational functioning on a dimensional scale (1: Lowest functioning level, 100: Highest functioning level). Sociodemographic data were also documented using the eCRF, including questions about family background, life history, educational and occupational history, and previous somatic and mental illness.
- Statistical analyses
Statistical data analysis was performed with SPSS version 29 (IBM Corp., Armonk, NY, USA). Descriptive data included absolute and relative frequencies as well as Mean (M) and Standard Deviations (SD) at metric scale level. For correlation analysis, the chi-square test (χ2 tests) respectively exact Fisher-Freeman-Haltontests (for more than 20% cell frequencies with values <5) were calculated for nominally scaled variables. Cramer's V (V) was determined as the effect size for variables with more than two categories. At the metric scale level, bivariate Pearson product-moment correlation analyses were performed [27]. A significance level of 5% was set for the statistical calculations.
Results
- Description of pilot phase sample
The pilot sample included 20 individuals participating in the online short-term therapy. The average age of the participants was 32.30 years (SD = 10.18), ranging from 20 to 57 years. The percentage of males was 70% (n = 14). The majority of participants had no migration background (n = 17; 85%). Subjects were primarily employed (n = 11; 55%), or students/ trainees (n = 8; 40%). Regarding socio-familial context, participants were mostly unmarried (n = 16; 80%) but in permanent partnerships (n = 14; 70%) and had no children (n = 14; 70%). Table 2 displays further sociodemographic data.
Recruitment to the SCAPIT study occurred for the majority of participants due to posts on social media (n = 6; 30%), advertisements on information platforms (n = 5; 25%), or on recommendations from related persons (n = 5; 25%). Recipients further participated in the study through referrals from outpatient addiction services (n = 2; 10%). One subject was motivated to participate through recruitment activities at the workplace (n = 1; 5%), along with proactive searches for disorder-specific online interventions (n = 1; 5%).
|
Variable |
Quantityn (%) Total (N = 20) |
Male (n = 14) |
Female (n = 6) |
|
Gender Male Female Diverse |
14 (70.0) 6 (30.0) 0 (0.0) |
|
|
|
Migration background No Yes |
17 (85.0) 3 (15.0) |
11 (78.6) 3 (21.4) |
6 (100.0) 0 (0.0) |
|
Family status Married Unmarried Divorced |
3 (15.0) 16 (80.0) 1 (5.0) |
3 (21.4) 11 (78.6) 0 (0.0) |
0 (0.0) 5 (83.3) 1 (16.7) |
|
Children No Yes |
14 (70.0) 6 (30.0) |
10 (71.4) 4 (28.6) |
4 (33.3) 2 (66.7) |
|
Relationship status Firm partnership No permanent partnership |
13 (65.0) 7 (35.0) |
10 (71.4) 4 (28.6) |
3 (50.0) 3 (50.0) |
|
Residential status Living with othersa Living alone |
12 (60.0) 8 (40.0) |
10 (71.4) 4 (28.6) |
2 (33.4) 4 (66.7) |
|
Highest Occupational qualification No high school diploma High school diploma Completed professional qualification Graduated Bachelor study Graduated Master study |
0 (0.0) 3 (15.0) 7 (35.0) 5 (25.0) 5 (25.0) |
0 (0.0) 3 (21.4) 5 (35.7) 2 (14.3) 4 (28.6) |
0 (0.0) 0 (0.0) 2 (33.3) 3 (50.00) 1 (16.7) |
|
Professional activity Unemployed Employed Student/ Trainee PhD Student |
0 (0.0) 11 (55.0) 8 (40.0) 1 (5.0) |
0 (0.0) 7 (50.0) 6 (42.9) 1 (7.1) |
0 (0.0) 4 (66.7) 2 (33.3) 0 (0.0) |
Table 2: Sociodemographic characteristics of the pilot sample.
Annotations. aOthers = Partners, roommates, parents. (N = 20).
- Internet use disorder
Based on self-report data, all of the participants in the pilot phase showed an IUD (N = 20; MCIUS= 36.30; SDCIUS = 6.4), which was on average above the cut-off value of 21 points. About one third of participants in the pilot sample reported a Video and Streaming Use Disorder (n = 7; 35%) or a Social Network Use Disorder (n = 7; 35%) as a condition for accessing the online intervention. In this case, pathological video and streaming behavior was limited to online computer games. Another 3 subjects stated to suffer from an Internet Gaming Disorder (15%), while 2 participants (10%) reported a pathological use of information platforms. One subject (5%) stated an online Pornography Use Disorder. On average, the internet has been used for 19.20 years (SD = 6.8 years), ranging from 10 to 33 years. Figure 2 illustrates the percentage of IUD recorded in the pilot phase sample.
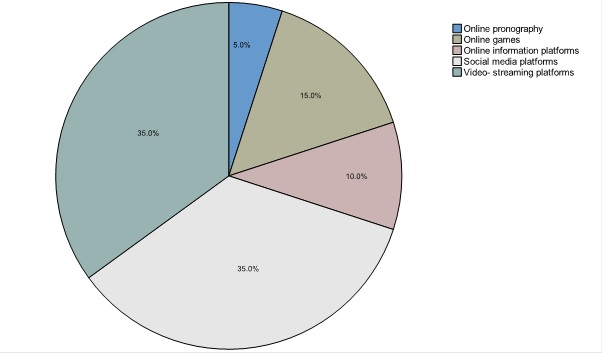 Figure 2: Percentages of pathological used internet applications or -contents.
Figure 2: Percentages of pathological used internet applications or -contents.
A cross tabulation was created to analyze correlations between gender and IUD. Regarding the preferred medium, no statistically significant association with the gender of participants was found (Χ2(4) = 4.95; p = 0.25; V = 0.51) with the two-tailed exact Fisher-Freeman-Halton test calculated based on an expected cell frequency of
- Comorbid psychopathologies
Along with the PHQ-D [25], which was applied to categorically diagnose current comorbid psychopathologies, previous mental disorders were standardized documented via eCRF. In table 3, assessed comorbid disorders are displayed. Multiple diagnoses could be assigned when there was evidence of a presence of distinct mental disorders. 14 participants (70%) in the pilot sample were affected by at least one other mental disorder at the time of inclusion, while 12 recipients (60 %) reported at least one previous mental disorder lifetime. According to the GAF score, participants in the pilot sample experienced moderate impairments in terms of social, occupational, or academic functioning (N = 20; M = 65.50; SD = 12.07).
|
Assessed disorders |
Quantity n (%) |
|
Present comorbiditiesa Affective disorders Anxiety disorders Somatoform disorders Eating disorders Alcohol abuse Previous mental disordersb Affective disorders Attention deficit (hyperactivity) syndrome Somatoform disorders Multiple mental disordersc |
12 (60.0) 6 (30.0) 2 (10.0) 3 (15.0) 3 (15.0)
4 (20.0) 1 (5.0) 1 (5.0) 6 (30.0) |
Table 3: Comorbid psychopathology and previous disorders.
Annotations. aOperationalized through the PHQ-D. bRecorded through supplement items in eCRF. cDefined as > 2 previous mental disorders. (N = 20). Multiple mentions possible.
On average, recipients of the online treatment intervention exhibited signs of moderate depression (MBDI-II = 21.00; SDBDI-II = 12.52), whereas the mean score for social phobic symptoms was beneath the cut-off value of 55 points (MLSAS = 43.00; SD LSAS = 26.49). Statistically significant correlations were calculated for CIUS sum score (M = 36.30; SD = 6.45) and depressiveness (M = 21.00; SD = 12.52; r = 0.57; p = 0.01).
- Intraindividual characteristics
For the analysis of correlations between intraindividual characteristics and symptomatology of IUD, assessed with the CIUS [15], additional Pearson product-moment correlation analyses were conducted. A statistically significant correlation was calculated for CIUS sum scores (M = 36.30; SD = 6.45) and compulsivity (M = 13.30; SD = 7.45; r = 0.60; p = 0.01). Table 4 displays results of the Pearson product-moment correlation analyses.
|
Comorbid psychopathology |
|||||||
|
|
1. |
2. |
3. |
4. |
5. |
6. |
7. |
|
1. CIUS |
1 |
|
|
|
|
|
|
|
2. Depression |
0.572** |
1 |
|
|
|
|
|
|
3. Social phobia |
0.131 |
0.218 |
1 |
|
|
|
|
|
4. Pos. affect |
0.490* |
0.519* |
0.135 |
1 |
|
|
|
|
5. Neg. affect |
-0.198 |
0.094 |
-0.143 |
0.204 |
1 |
|
|
|
Intraindividual characteristics |
|||||||
|
6. Compulsivity |
0.601** |
0.743** |
0.091 |
0.640** |
0.233 |
1 |
|
|
7. Self-efficacy |
-0.380 |
-0.161 |
-0.664** |
-0.164 |
0.339 |
-0.182 |
1 |
Table 4: Results of pearson product-moment correlation analyses.
Notes.**Significant correlation at 0.01 level (two-tailed); *Significant correlation at 0.05 level (two-tailed).
Discussion
The objective of this analysis was a clinical characterization of recipients of a novel online treatment intervention for IUD. Therefore, sociodemographic, psychopathological and intraindividual characteristics from the pilot phase sample (N = 20) of the SCAPIT online short-term therapy were assessed and analyzed in terms of correlations with the symptomatology of IUD. Consistent with results of previous studies on IUD, a distinct underrepresentation of female participants was found in the pilot sample [13,28,29]. In an inventory and needs assessment survey in schools, counseling centers, and clinics, among individuals seeking counseling or treatment services for IUD in Germany, an estimated 9% were female [30], while Dufour and colleagues [31] found a frequency distribution of 94% male and 6% female respondents in the treatment services system for IUD. Epidemiological studies, in contrast, reveal no significant differences in the prevalence of IUD among men and women, indicating comparable characteristics and symptom burdens in both genders [32], although females appear to seek existing help services to a considerably smaller extent. In this regard, results from the characterization of the pilot sample emphasize that the low access rate of women with IUD appears to exist in both offline psychotherapeutic care institutions and online treatment services. Future research should verify this finding and consequently examine what recruitment initiatives can advance the access rate of affected women. One possible explanation for the gender-specific underrepresentation could be that IUD are more likely to remain undetected at women. For instance, one study showed that a pathological internet use was missed by treatment providers in 94.64% of women (N = 327) assessed [33]. Based on this, it can be surmised that women tend to seek treatment for comorbid mental health disorders and thus symptomatology of IUD might be relegated to the background. Results from the characterization of the pilot sample consistently indicate that the majority of online short-term therapy recipients have at least one comorbid psychopathology at the time of inclusion (n = 14; 70.0%) or during life course (n = 12; 60.0%). Other studies have also found that behavioral addictions mostly co-occur with comorbid mental disorders and are associated with anxiety, depressiveness, and personality disorders in treatment-seeking individuals [34]. Comorbid occurrence of psychopathologies requires a differentiated alignment of the intervention to symptom complexes of those affected. Subsequently, coexisting disorders should be addressed in the context of treatment interventions for IUD, which may lead to challenges in clinical practice. Additionally, IUD should be proactively assessed in cases where help is sought for other apparent disorders, especially among vulnerable groups [35]. Therefore, it is important to raise awareness for symptoms of IUD in clinical practice [34,36]. In addition, affected individuals with an IUD having a migration background also seem to be underrepresented in this pilot sample. Consistent with studies on other manifestations of behavioral addictions, an underrepresentation of individuals with an immigrant background was observed among gambling addicts [37]. Treatment services for IUD should therefore aim for an increased inclusion of immigrant populations. Summarizing, findings on the sociodemographic data of participants in the pilot phase sample indicate an apparent underrepresentation of certain individuals with IUD even in an online setting. Future research should examine whether results from this sample characterization are generalizable to disorder specific online interventions and address underlying reasons for underrepresentation.
Regarding the preferred use of different internet applications and contents, previous research indicated gender differences [30,38], that were not replicated in this analysis. In the piloting sample, video and streaming platforms (n = 7; 35%) related to online computer games were consumed most frequently, along with social networks (n = 7; 35%). The surprisingly high usage preference of video and steaming platforms highlights the need for further research, as behavioral addictions related to this digital modality are under-researched so far. Consequently, the scientific evidence on behavioral addictions related to the use of video and streaming platforms should be further investigated.
Limitations
The interpretation of the present results is constrained by several limitations. Specific manifestations of IUD have been classified in this analysis although diagnostic criteria are currently available solely for Internet Gaming Disorder and Internet Gambling Disorder [4,39]. In the absence of diagnostic classification criteria for other manifestations of IUD, adapted criteria based on DSM-5 and ICD-11 were applied. In addition, IUD was considered as an entity in the correlation analyses, due to the small sample size distinct internet activities were not considered differentiated from each other. The sample size represents a methodological limitation restricting the generalizability of the results, although findings exhibit a high degree of consistency with previous studies in terms of sociodemographic characteristics and psychopathological comorbidity. Further, no conclusions about causality can be drawn on the basis of correlative analyses. Finally, it is limiting to note that the present analysis is methodologically a cross-sectional observational study, which is why the results and the resulting implications have an explorative character.
Despite these limitations, initial implications for treatment interventions for IUD can be derived from the clinical characterization of recipients of a novel online short-term therapy. The underrepresentation of certain populations of affected individuals with IUD also appears to persist in the online setting. Based on this, initiatives to increase the prevalence of women and individuals with an immigrant background should be researched. Complementary, particular consideration should be given to the screening and diagnostic of IUD in clinical practice. Identified associations of IUD and comorbid psychopathologies emphasize the importance of tailoring interventions to the disorder-specific symptom complexes of the affected individuals.
Conflict of Interest
The authors declare no conflict of interest.
Funding Statement
Financial support for the study is provided by the Innovation Fund of the Federal Joint Committee (ID = 01NVF19031). The scientific lead lies with the University of Lübeck, Department of Psychiatry and Psychotherapy. The implementation of the research project is realized in cooperation with University Medical Center Mainz, the University of Ulm, Free University Berlin, CONVEMA Versorgungsmanagement GmbH (lead of the consortium) and Media Protect GmbH.
References
- Király O, Potenza MN, Stein DJ, King DL, Hodgins DC, et al. (2020) Preventing problematic internet use during the COVID-19 pandemic: Consensus guidance. Compr Psychiatry 100: 152180.
- Montag C, Pontes HM, Rozgonjuk D, Brandt D, Bischof A, et al. (2022) Examining the interplay between Internet Use Disorder tendencies and well-being in relation to sofalizing during the COVID-19 pandemic. PsychArchives.
- Rumpf HJ, Batra A, Bischof A, Hoch E, Lindenberg K, et al. (2021)Vereinheitlichung der Bezeichnungen für Verhaltenssüchte. SUCHT 67: 181-185.
- World Health Organization (2018) ICD–11 for Mortality and Morbidity Statistics. International Classification of Diseases 11th Revision. WHO, Geneva, Switzerland.
- Castro-Calvo J, King DL, Stein DJ, Brand M, Carmi L, et al. (2021) Expert appraisal of criteria for assessing gaming disorder: An international Delphi study. Addiction 116: 2463-2475.
- Brand M, Rumpf HJ, Demetrovics Z, MÜller A, Stark R, et al. (2020) Which conditions should be considered as disorders in the International Classification of Diseases (ICD-11) designation of "other specified disorders due to addictive behaviors"? J Behav Addict 30: 150-159.
- Fineberg NA, Menchón JM, Hall N, Dell'Osso B, Brand M, et al. (2022) Advances in problematic usage of the internet research - A narrative review by experts from the European network for problematic usage of the internet. Compr Psychiatry 24: 152346.
- Rumpf HJ, Brand M, Wegmann E, Montag C, MüllerA, et al. (2020) Covid-19-Pandemie und Verhaltenssüchte. SUCHT 66: 212-216.
- Mestre-Bach G, Blycker GR, Potenza MN (2020) Pornography use in the setting of the COVID-19 pandemic. J Behav Addict 9: 181-183.
- Paschke K, Austermann MI, Simon-Kutscher K, Thomasius R (2021) Adolescent gaming and social media usage before and during the COVID-19 pandemic Interim results of a longitudinal study. Sucht 67: 13-22.
- Gjoneska B, Potenza MN, Jones J, Corazza O, Hall N, et al. (2022) Problematic use of the internet during the COVID-19 pandemic: Good practices and mental health recommendations. Compr Psychiatry 112: 152279.
- Wölfling K, Jo C, Bengesser I, Beutel ME, Müller KW (2013) Computerspiel- und Internetsucht: Ein kognitiv-behaviorales Behandlungsmanual. Störungsspezifische Psychotherapie.
- Wölfling K, Müller KW, Dreier M, Ruckes C, Deuster O, et al. (2019) Efficacy of Short-term Treatment of Internet and Computer Game Addiction: A Randomized Clinical Trial. JAMA Psychiatry 76: 1018-1025.
- Bischof A, Brandt D, Schlossarek S, Vens M, Rozgonjuk D, et al. (2022) Study protocol for a randomised controlled trial of an e-health stepped care approach for the treatment of internet use disorders versus a placebo condition: the SCAPIT study. BMJ open 12: 061453.
- Meerkerk GJ, Van Den Eijnden RJ, Vermulst AA, Garretsen HF (2009) The compulsive internet use scale (CIUS): Some psychometric properties. Cyberpsychol Behav 12: 1-6.
- Peukert P, Steffen S, ElKasmi J, Barth GM, Meerkerk GJ, et al. (2012) Faktorielle Struktur der deutschen Version der Compulsive Internet Use Scale (CIUS) nach konfirmatorischer Faktorenanalyse. Zeitschrift für Klinische Psychologie und Psychotherapie 41: 101-108.
- Gürtler D, Rumpf HJ, Bischof A, Kastirke N, Meerkerk GJ, et al. (2014) Psychometrische Eigenschaften und Normierung der deutschen Version der Compulsive Internet Use Scale (CIUS). Diagnostica 61: 1-12.
- Wölfling K, Müller KW, Beutel ME (2010) Reliability and Validity of the Scale for the Assessment of Pathological Computer-Gaming (CSV-S). Psychotherapie Psychosomatik Medizinische Psychologie 61: 216-224.
- Steffen S, Peukert P, Petersen KU, Batra A (2012) Messverfahren zur Erfassung der Internetsucht. SUCHT 58: 401-413.
- Kuhner C, Burger C, Keller F, Hautzinger M (2007) Reliabilität und Validität des revidierten Beck-Depressionsinventars (BDI-II). Der Nervenarzt 78: 651-665.
- Petrowski K, Schmalbach B, Kliem S, Hinz A, Brähler E (2019) Symptom-Checklist-K-9: Norm values and factorial structure in a representative German sample. PLoS One 14: 0213490.
- Stangier U, Heidenreich T (2005) Liebowitz social anxiety scale. Internationale Skalen für Psychiatrie (Internatioal Scales for Psychiatry). Beltz, Weinheim, Germany.
- Schwarzer R, Jerusalem M (2010) The general self-efficacy scale (GSE). Anxiety, Stress, and Coping 12: 329-345.
- Breyer B, Bluemke M (2016) Deutsche Version der Positive and Negative Affect Schedule PANAS (GESIS Panel). GESIS, Germany.
- Gräfe K, Zipfel S, Herzog W, Löwe B (2004) Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ-D)”. Diagnostica 50: 171-181.
- Endicott J, Spitzer RL, Fleiss JL, Cohen J (1976) The global assessment scale. A procedure for measuring overall severity of psychiatric disturbance. Arch Gen Psychiatry 33: 766-771.
- Cohen J (1988) Statistical power analysis for the behavioral sciences (2ndedn). Lawrence Erlbaum Associates, Hillsdale, USA.
- te Wildt BT, Dieris-Hirche J, Bottel L (2018) Entwicklung und Evaluation eines Online-Ambulanz-Service zur Diagnostik und Beratung von Internetsüchtigen (OASIS). Bundesministerium für Gesundheit.
- Bottel L, Dieris-Hirche J, te Wildt B (2019) Personenbezogene Merkmale von Teilnehmenden des Online-Ambulanz-Service für Internetsüchtige (OASIS). Suchttherapie 20.
- Petersen KU, Hanke S, Bieber L, Muhleck A, Batra A (2017) Angebote bei internetbasiertem Suchtverhalten (AbiS). Pabst Science Publishers.
- Dufour M, Brunelle N, Khazaal Y, Tremblay J, Leclerc D, et al. (2017) Gender difference in online activities that determine problematic internet use. Journal de Thérapie Comportementale et Cognitive 27: 90-98.
- Rumpf HJ, Vermulst AA, Bischof A, Kastirke N, Gürtler D, et al. (2014) Occurence of internet addiction in a general population sample: A latent class analysis. Eur Addict Res 20: 159-166.
- Scherer L, Mader L, Wölfling K, Beutel ME, Dieris-Hirche J, et al. (2021) Nicht diagnostizierte internetbezogene Störungen im psychotherapeutischen Versorgungssystem: Prävalenz und geschlechtsspezifische Besonderheiten. Psychiatrische Praxis 48: 423-429.
- Wölfling K, Dreier M, Beutel ME, Müller KW (2022) Inanspruchnehmende einer Spielsuchtambulanz mit Doppeldiagnosen. Sucht 68: 251-262.
- Müller KW, Beutel ME, Wölfling K (2014) A contribution to the clinical characterization of Internet addiction in a sample of treatment seekers: Validity of assessment, severity of psychopathology and type of co-morbidity. Compr Psychiatry 55: 770-777.
- te Wildt BT (2019) Diagnostik und Therapie der Internetabhängigkeit. Die Rehabilitation 57: 321-333.
- Hayer T, Girndt L, Brosowski T (2020) Die Bedeutung der Selbsthilfe in der Versorgung pathologischer Glücksspieler*innen: Nutzen, Grenzen und Optimierungspotenziale. Universität Bremen, Bremen, Germany.
- Dufour M, Brunelle N, Tremblay J, Leclerc D, Cousineau MM, et al. (2016) Gender difference in Internet use and Internet problems among Quebec high school students. Can J Psychiatry 61: 663-668.
- American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR). American Psychiatric Publishing, Arlington, USA.
Citation: Basenach L, Rumpf H-J, Dreier M, Renneberg B, Gnauert O, et al. (2023) Clinical Characterization of the Pilot Sample of an Online Short-Term Therapy for Internet Use Disorder. J Addict Addictv Disord 10: 121.
Copyright: © 2023 Lara Basenach, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.