Creative Dance in Neurorehabilitation: A Pilot Study
*Corresponding Author(s):
Loi MIstituti Clinici Scientifici Maugeri IRCCS, Via Maugeri 1, 27100 Pavia (PV), Italy
Email:marianna.loi@icsmaugeri.it
Abstract
Background
Dance is an increasingly common type of intervention in several domains of the medical field due to its active stimulation of both physical and mental well-being as well as its capability to instill calmness, equilibrium and ability to manage emotions.
Creative Dance (CD) helps patients to acquire the fundamental rules of movement with minimal energy consumption and a constant improvement in performing motorial actions self-confidently, which allows for greater autonomy in activities of daily living (https://www.sisbio.it/discipline/danza-creativa).
The purpose of CD sessions is to provide patients with the necessary means to express themselves from a physical point of view, communicating emotions through movement. The employment of CD in adult subjects has recently been object of a study that highlighted its advantages in the motorial, motivational and social inclusion domains.
Objective
The purpose of this observational longitudinal pilot study is to evaluate the feasibility and the appreciation of CD in a group of patients admitted for neurorehabilitation care for different types of neurological diseases. Secondly, it is meant to appraise the entity of the potential improvement of global motor functionality and its reverberation on the quality of social life, on day-to-day autonomy in life and in the sphere of social and interpersonal relationships and on the possible rise in compliance to the proposed treatments.
Methods
We consecutively enrolled 68 patients, 33 males (67+15.01) and 35 females (60+14.26), admitted at the Department of Neurorehabilitation of IRCCS Maugeri Institute of Pavia Boezio; they started the activity of Creative Dancing (the initial familiarization phase) and the standard treatment between October 2016 and December 2017.
The first 3 to 4 lessons were necessary to the group to comprehend the proposed style of dance and the necessary means of both physical and communicative expression in relation to their understanding of the space that was provided to them for interaction. The music played was chosen in relation to the enjoyment of the patients.
The inclusion criteria were: to be >18 years old, to be capable of giving consent and to be diagnosed with chronic neurological conditions.
Between the exclusion criteria are counted: being incapable of giving consent, aphasia and a high risk of falling.
At baseline, on every patient was performed the clinical evaluation, complete with the use of the FIM, Barthel and CIRS-G tests. The risk of falling was measured on the Morse e Stratify scales. At the end of the treatment the clinical evaluation, the FIM scale and the semi-structured satisfaction questionnaire were repeated.
Results
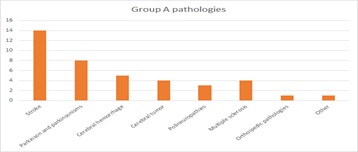
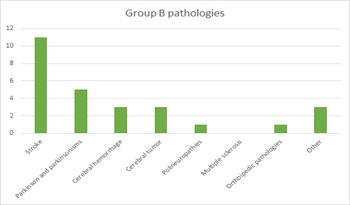
The epidemiological and pathological characteristics of the patients were gathered through an in- depth anamnesis. The subjects were divided into two groups: Those who completed less than 5 treatments (a maximum of 4 sessions, namely those necessary to understand the basics of the task) those who completed 5 or more treatments of CD. Group A was composed of 41 patients (20 men, 21 women, average age of 64,12 + 15.37) and Group B was composed of 27 patients (13 men, 14 women, average age of 63,85 +14.58): there was no significative difference between groups besides the score on the CIRS-G scale that highlighted a higher number of comorbidities in Group
The results showed a global improvement (Delta FIM trend) in the group that continued with CD treatments, which also registered a higher rate of satisfaction and a higher rate of adherence to the therapy (a statistically significant value).
Group A started at a better FIM baseline so it was possible that, at baseline, the motivation was lower. A qualitative evaluation of patients in Group B, which underwent double treatment, showed a global psychomotor improvement and, above all, a better awareness of their bodies in the space they occupy accompanied by a new pursuit of strategies to compensate for their inability as well as a global improvement in their mood and socialization skills.
Conclusion
In conclusion, CD, like other types of dancing, appears to be helping patients affected by neurological chronic conditions to regain their psycho-physical balance. The comprehension of the task and the global participation were satisfactory, so the CD treatment might be integrated in a targeted neurorehabilitative treatment. This pilot study lays the foundation for a future in-depth research on the use of this therapeutic strategy in support of the Departments of Neurorehabilitation.
Keywords
Creative Dance; Neurological Disease; Rehabilitation
Introduction
Impressing fluidity to the movement of the body means imparting fluidity to the thought process, stimulating creativity and freeing individual expression through a different language. Movement is a form of language that enables the expression of the individual, which consents a process of transformation and evolution [1]. This process finds one of its major expressions in dancing and its purpose can be the emotive and psychic rehabilitation, motor recovery, but can also have an educative or formative goal, as it happens, for example, in the evaluative stage [1].
Creative Dancing (CD) allows learning the fundamental rules of movement with minimal energy consumption, a progressive incrementation of self confidence in the performance of motorial exercises which brings to a better autonomy in day-to-day life activities. Nowadays CD is widely used in several countries. The methodology is easy but manageable and in- depth and it brings together people of all ages and all psychophysical conditions.
During a CD session —through movement accompanied by music— are suggested easy, non- technical choreographies while with the aid of images and objects (fabrics, rubber bands, paper, etc) a physically and emotionally involving atmosphere is created, where it becomes possible to explore creativity and self-expression.
All of this helps mood improvement, increases self-awareness and hints at helpful behaviours for the well-being of the self.
For this to happen, the methodology has to be applied in a group setting, so that the presence of other people can allow dance to be used as an instrument of communication and expression.
Each CD session is characterized by a peculiar use of music, objects and materials and a precise valorisation of space, which are integrated in a symbolic path through evocative and significative, although coherent, images.
The purpose of these stimuli is to gradually lead the people in the group to get in touch with their bodies and the surrounding space, to explore and value the countless possibilities offered by movement, and to gradually connect with the others through a progressive transformation of movement into dancing The purpose of these CD sessions is to equip patients with the means to express themselves in a physical way and to communicate emotions through movement.
The employment of CD in adult subjects has recently been an object of study (Joung et al. 2019). The authors have used this methodology with an elderly population, concluding with an improvement in the dynamic balance and in the global mobility therefore contributing to healthy aging [2]. Suggested using CD to enhance the proprioception of the body in the elderly population [3] Noted how CD improved posture and balance in the pediatric population affected by cerebropathy. In neurorehabilitation, [4]’s equipe applied this methodology to young adolescents affected by spasticity induced by neonatal cerebropathy, emphasizing-at the end of the 3 months treatment— how the articulation of knees and hips was improved and the speed and the length of the walking step increased together with an overall improving of their body image.
The role of CD is to associate repetitive movements with spatial exploration and music listening in patients to let them acquire the fundamental rules of movement to reach a greater autonomy in activities of daily living.
Therefore we decided to integrate the aspects of this type of dance with the standardized rehabilitation activities.
The purpose of this observational longitudinal pilot study was to evaluate the feasibility and the appreciation of CD in a group of patients admitted in neurorehabilitation care for different neurological pathologies. Secondly, it was meant to appraise the entity of the potential improvement of global motor functionality and its reverberation on the quality of social life, on day- to-day autonomy in life and in the sphere of social and interpersonal relationships and on the possible rise in compliance to the proposed treatments.
Methods
Inclusion criteria: patients had to be >18 years old, capable of understanding the directions given to them, being affected by neurological conditions, being hospitalized at the Neurorehabilitation Department of Maugeri Boezio Institute and being able to sign a written informed consent.
At baseline, before the beginning of the treatment, the clinical and neurological evaluation was carried out with the tests FIM, Barthel and CIRs-G. The risk of falling was measured on the Morse and Stratify scales: values lower than 44 on the Morse scale (medium-low risk of falling), values lower than 2 on the Stratify scale (low risk of falling).
The neurological diseases included in the study were: either ischemic or hemorrhagic stroke, Parkinson’s disease or parkinsonisms, brain tumor outcomes, polyneuropathy, multiple sclerosis, orthopedic pathologies with neurological stupor, congenital or acquired ataxias.
Exclusion criteria: symptoms so severe that prevented therapeutic adherence and/or orthopedic pathologies obstructive to the course of the proposed activities, a high risk of falling, diagnosed global aphasia.
The CD sessions were held during the hospitalization period with bi-weekly incidence, in the early afternoon. They lasted 45 minutes and were held in an assigned space with groups of six subjects per session, for a maximum of 9 sessions.
The initial purpose of the first 3-4 sessions was to provide patients with the necessary means for the optimization of their ingrained actions, learning or alternating between different movement activities and communicating and self-expressing through movement.
These goals were reached by teaching patients a series of fundamental principles such as:
- body rieducation
- appropriate motor execution
- use of space
- response to music
- Enriching the range of movements and the skill in executing them was fundamental in that only if the action was well executed it was possible to consider it beyond the mere athletic gesture and as a purposeful body gesture.
- The sessions were structured into two parts dedicated to:
- establishing ground rules and making sure patients understood them
- broadening movement knowledge and enhancing global capacity of execution through
- Varied choreographies tailored to the patients’ needs.
This type of treatment requires patients, in addition to experiencing movement, to be guided through the exercises to create their own moves, and that they are put in a position where they are able to observe the movement in order to increase its execution and enrich their creative and analytical skills. In every session the CD physiotherapist presented a form of movement: it could be focused on space, on the direction of the movement or it could involve a dynamic approach.
After concluding these “familiarization” sessions, patients were proposed to carry on with this type of activity (and go through with other CD sessions) or to switch to standard rehabilitation activity. Patients that carried on with rehabilitation activity that included CD were assigned to Group B, while the other patients were assigned to Group. After the warm-up were then explored ways to allow the patient to experience the moves in their simpler form and to gradually transform them into something more complicated, refining the ability to control that same movement.
At the end of every session it was agreed on a song or an artist that would be played during the next meeting so that the participants could feel personally involved while approaching music listening. Ultimately the music was chosen depending on the purpose and the execution of the exercises, so that it could be integrated with the choreographed motions learnt beforehand.
Every patient also followed an hour of physiotherapy six times a week, generally in the morning, following the traditional protocol targeted to fulfill the needs outlined by the initial diagnosis.
Patients were so divided: Group A. Those who had completed ≤ 4 treatments (that is the number of sessions necessary
To understand the basics of the task) Group B. Those who had completed 5 or more treatments of CD. At the end of the treatment, a qualitative evaluation of the subjects was carried on by the CD physiotherapist through a semi-structured interview.
The semi-structured questionnaire asked the patients whether they were satisfied with the treatment, if they had difficulties with the exercises and what they perceived to be the biggest improvement since the beginning of the treatment.
At the end of the treatment it was also performed an objective neurological assessment using the FIM instrument. Within the year of the acute event an interview with the patient was performed during a planned neurological exam, or via telephone, to evaluate the individual perception of the clinical, psychological and social improvement through time.
Statistics
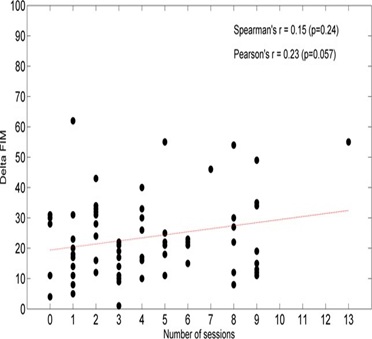
The Shapiro–Wilk statistic supported by visual inspection was used to test the normality of the distribution of all continuous variables. Because no severe violations to the normality assumption were observed, descriptive statistics are reported as mean ± SD and parametric tests were used. Categorical variables are reported as N (percent frequency). Between-group comparisons for continuous variables were carried out by unpaired t-tests. Between groups comparisons for categorical variables were carried out by the Chi-square test or Fisher exact test when appropriate. Within-group comparisons were carried out by paired t-test. To test the hypothesis that CD could affect positively the primary rehabilitation outcome, namely FIM score, and determine benefit as compared to traditional rehabilitation protocols, we considered the difference between the discharge and admission values and compared these differences by unpaired t-test. The association between variables was assessed by Spearman’s rank correlation coefficient or Pearson’ correlation coefficient, as appropriate. A p value <0.05 was considered statistically significant. All analyses were carried out using the SAS/STAT statistical package, release 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Overall, 68 patients hospitalized at the Department of Neurorehabilitation of ICS Maugeri Boezio were consecutively enrolled from October 2016 to December 2017. Out of these 68 patients, 33 were male (average age 67+15.01 sd) and 35 were female (average age 60+14.26 sd). All of them signed a written consent where the type and the purpose of the longitudinal observational prospective study were stated. The clinical features’ data (independent variables) are resumed in the tables shown below.
Out of these 68 patients, 27 carried out a complete CD rehabilitation protocol (Grp B), and 41 followed a traditional rehabilitation protocol (Grp A). Group A and Group B do not differ in age and autonomy in the ADLs assessed on the Barthel scale. The only differences regard the comorbidities (statistically significant CIRS-G difference), more severe in Group B.
Continuous Variables
The improvement on the FIM scale was greater in Group B at the end of the treatment, although the improvement was not statistically significant (Table 1). The sample’s epidemiological features are reported in the tables as follows
|
Variable |
N Grp A |
N Grp B |
Grp A |
Grp B |
P (unpaired t-test) |
|
Age |
41 |
27 |
64.12 ± 15.37 |
63.85 ± 14.58 |
0.94 |
|
Barthel_I |
41 |
27 |
13.20 ± 3.74 |
11.85 ± 4.26 |
0.17 |
|
Barthel_pct |
41 |
27 |
33.05 ± 18.33 |
40.74 ± 21.29 |
0.12 |
|
CIRS_G |
41 |
27 |
10.46 ± 4.35 |
13.63 ± 5.46 |
0.010 |
|
FIM_I |
41 |
27 |
89.15 ± 17.00 |
85.93 ± 18.17 |
0.46 |
|
FIM_D |
41 |
27 |
110.71 ± 10.00 |
112.74 ± 10.89 |
0.43 |
|
DeltaFIM |
41 |
27 |
21.56 ± 12.02‡ |
26.81 ± 15.02‡ |
0.12 |
Table 1: Grp A: patients that followed 5 sessions.
Data expressed as mean±SD
‡: p< 0.001 testing H0= DeltaFIM=0
Regarding dichotomous variables, there are no differences in age and sex. Regarding comorbidities, a greater predisposition to cardiopathies in Group B should be noted.
Dichotomous Variables
|
Variable |
N Grp A |
N Grp B |
Grp A = 1 |
Grp B= 1 |
p chisq |
|
Sex |
41 |
27 |
20 (48.8%) |
13 (48.1%) |
0.96 |
|
Marital status |
41 |
27 |
31 (75.6%) |
20 (74.1%) |
0.89 |
|
Stroke |
41 |
27 |
14 (34.1%) |
11 (40.7%) |
0.58 |
|
Parkinson |
41 |
27 |
4 (9.8%) |
1 (3.7%) |
0.35 |
|
Parkinsonisms |
41 |
27 |
4 (9.8%) |
4 (14.8%) |
0.53 |
|
Cerebral hemorrhage |
41 |
27 |
5 (12.2%) |
3 (11.1%) |
0.89 |
|
Cerebral tumor |
41 |
27 |
4 (9.8%) |
3 (11.1%) |
0.86 |
|
Polyneuropathies |
41 |
27 |
3 (7.3%) |
1 (3.7%) |
0.54 |
|
Multiple sclerosis |
41 |
27 |
4 (9.8%) |
0 (0.0%) |
0.09 |
|
Orthopedic pathologies |
41 |
27 |
1 (2.4%) |
1 (3.7%) |
0.76 |
|
Other |
41 |
27 |
2 (4.9%) |
3 (11.1%) |
0.34 |
|
Arterial hypertension |
41 |
27 |
24 (58.5%) |
14 (51.9%) |
0.59 |
|
Dyslipidemia |
41 |
27 |
16 (39.0%) |
11 (40.7%) |
0.89 |
|
Arterosclerosis |
41 |
27 |
15 (36.6%) |
14 (51.9%) |
0.21 |
|
Diabetes Mellitus |
41 |
27 |
9 (22.0%) |
7 (25.9%) |
0.71 |
|
Pneumopathy |
41 |
27 |
3 (7.3%) |
3 (11.1%) |
0.59 |
|
Cardiopathy |
41 |
27 |
10 (24.4%) |
14 (51.9%) |
0.020 |
|
Mood disorder |
41 |
27 |
26 (63.4%) |
19 (70.4%) |
0.55 |
|
Satisfaction |
41 |
27 |
14 (34.1%) |
25 (92.6%) |
<0.0001 |
|
Easiness |
41 |
27 |
17 (41.5%) |
16 (59.3%) |
0.15 |
Data expressed as N = number of patients with variable =1 (%)
 At the end of the treatment, a qualitative evaluation of the subjects was carried out by the CD therapist through a semi-structured interview. The interview inquired whether the patients were satisfied with the treatment, if they had difficulties with learning and performing the exercises, their mood variation compared to the beginning of the treatment and inquired about the ability to communicate with unfamiliar people in their work group.
At the end of the treatment, a qualitative evaluation of the subjects was carried out by the CD therapist through a semi-structured interview. The interview inquired whether the patients were satisfied with the treatment, if they had difficulties with learning and performing the exercises, their mood variation compared to the beginning of the treatment and inquired about the ability to communicate with unfamiliar people in their work group.
Additionally patients were asked to freely express their opinion on what actually improved in those weeks.
From these interviews emerged a psycho-motor improvement of the patients, and above all a better awareness of their bodies in the space they occupy accompanied by a new pursuit of strategies to compensate for their inability as well as a global improvement in their mood and socialization skills. Within the year of the event an interview with the patient was performed during a planned neurological exam, or via telephone; 13 patients (19.12%) didn’t follow up.
Most patients who hadn’t continued with the double program did remember neither its characteristics nor the difficulties it posed. The patients of Group B instead, even after the end of the treatment, kept in touch and kept interacting with each other; the benefits of the therapy persisted over time as evidenced by the ongoing pursuit of socialisation as means of mutual help and support.
Discussion
Recently, Creative Dance (CD) is being proposed more and more frequently to the young and elderly population. There are two reasons why this dance is being suggested to the elderly: the first one being that CD does not require a standard preparation priory acquired with long trainings. Secondly, CD promotes the flourishing of interpersonal relationship among the participants, stimulating emotivity, joy, enjoyment, in addition to increasing the quality of life [5-9].
CD is a vehicle for interpretation of ideas, stimulation of sensations, personal creativity and a means of bonding with the participants, which are then communicated symbolically through motion [10]. Some studies showed how CD can take inspiration from other styles of dance and — with the help of a professional that is familiar with the subject’s personal skills in terms of agility, resistance and fatigability — CD can resolve various types of discomfort passing through the symbolic world of images [6]
There are few studies that outline the benefits of CD on the elderly population: in particular the improvement of proprioception [11] social abilities [12] body image [8] quality of life (Osgood et al. 1990), psycho-social wellness and cognitive functions [13] body form and perception, agility and balance [5]
The application of CD to adult subjects has recently been an object of study [14] the authors applied this treatment to an elderly population, finding an improvement of dynamic balance and global mobility that overall contributed to a healthy aging process.
In the neurorehabilitative field [3] noticed how, in the pediatric population affected by cerebropathy, CD improved posture and balance [4] applied CD to young teenagers affected by spasticity induced by neonatal cerebropathy: at the end of the 3 months treatment he noticed how the articulation of knees and hips improved and the speed and the length of the walking step increased together with an overall improving of their body image.
To our knowledge, CD has never been employed with an adult population affected by neurological disease.
Dance is overall a form of treatment increasingly common in many medical fields, and in particular for neurological diseases [15-18]
A recent review [19] analyzed nine works in which dance was used as a form of therapy for balance, improvement of footstep pattern and motor functionality of all four limbs, not only in Parkinson’s disease (the better investigated disease in these studies) but also in many other neurological diseases such as stroke, multiple sclerosis, Huntington’s disease and others.
In the conclusions it emerged how there were different motivations in support of CD treatment in neurorehabilitation, however, further randomized and controlled studies with a higher number of cases and different forms of dance with repetitive and standardized moves should be necessary.
In the same review it was stated it would be preferable to do an evaluation of the tolerability of the treatment and the registration of possible adverse events.
Some styles of dance such as valzer, Argentinian tango, Sardinian folk dance and Irish dance, have been associated with Parkinson’s rehabilitation yielding good results both in motor success and in patients’ quality of life [16, 17]
Bognar’s study [18] provided a unique point of view from the perspective of patients affected by Parkinson’s disease on the experience of a group dance program. Community-based dance lessons allow people with Parkinson’s disease to develop once more their social self and, if need be, a sense of enjoyment in life. Dance programs allow for re-establishing self-identity and a sense of usefulness through the offer Of opportunities for social interactions, non-verbal communication and self-improvement. Dance, as a rehabilitation tool, is emerging as a strategy to face the physical and psychosocial effects of Parkinson’s disease, encouraging an increase in social participation that lowers isolation and improves quality of life. Moreover it shows improvements in disease self-management.
Contemporary dance is also used to treat Huntington’s disease and seems to improve motor functionality. Belly dance, used to treat women affected by low back pain seems to positively influence the progression of chronic pain. Aerobic dance, proposed in the treatment of mild cognitive impairment (Yi Zhu et al., 2018) seems to improve the mnemonic capabilities and the working memory.
The studies unanimously agree on the improvement of the quality of life of neurologic patients. Another important point is the treatment of patients affected by both ischemic and hemorrhagic stroke with rehabilitation treatments combined with some forms of dance, both in early and late stages.
Thornberg [20] applied the RGRM (Ronnie Gardiner rhythm and Music) method reaching the conclusion that the activation of mirror neurons is fundamental to the process of improvement, providing the patient had created beforehand an internal representation of the body scheme guided by music, using a more functional motor scheme.
Therefore, music and rhythm are fundamental in neuronal plasticity.
In the aforementioned work Thornberg emphasized how music in neurorehabilitation has the capability of improving the synchronization of movement, functioning as a guide of motor action in subjects who lost their capability of motor planning.
[21] Claimed that the employment of music can improve both uncoordinated and finer motion, improving velocity, precision and singular movement perfection.
Music also impacts emotions, cognitive functions and memory [22] Music is experienced as a guide for the motor system.
Elements such as melody, harmony, rhythm and metric help in finding the right pacing for the motions, bypassing motor difficulties [21]
Regarding our work, we chose to enroll a group of patients with neurological conditions, first and foremost to study the feasibility and satisfaction of a standard rehabilitation protocol combined with CD; secondly we wanted to study how the employment of Creative Dancing (in addition to the usual care) could influence an outcome standardized valuation parameter (FIM) [23-25].
Both groups were overall homogeneous in regards of age, sex, and marital status. From a comorbidities viewpoint, the baseline values of both groups were homogeneous besides CIRS_G (Group B had a higher number of comorbidities) and Group B had a higher cardiopathic incidence.The main result of our study is that Group B, which had more difficulties due to starting with a lower FIM score, benefited more than Group A from the combined use of DC with traditional physiotherapy treatment, even though the difference wasn’t statistically significant. Both groups’ FIM scores improved significantly although there is no difference in the entity of the improvement; even if Group B performed slightly better (DeltaFIM 21.56 vs 26.81 con p < 0.12). Both groups appreciated how easy was the execution of the exercises and moves learnt during the CD sessions [26,27].
This result is aligned with what other studies on elderly population already emphasized: CD improves gratification and dedication during the treatment. Such positive results will support the employment of CD treatment in neurorehabilitation in the future. Emphasized how participation in creative dance and movement activities is beneficial for older adults and how it contributes positively to their morale, encouraging expression of feelings and needs. Group participation, body awareness and sensitivity, laughter, joy, and fun were also important goals of these sessions. This level of involvement in the patients resulted in self-confidence, pride and accomplishment, group cohesiveness and life satisfaction. Within the year of the acute event an interview with the patient was performed during a planned neurological exam, or via telephone, to evaluate the individual perception of the clinical, psychological and social improvement through time.
Most patients who hadn’t continued with the double program (Group A) did remember neither its characteristics nor the difficulties it posed. The patients of Group B instead, remembered receiving the treatment, sometimes asking for its administration at home even after the end of the treatment, and kept in touch and kept interacting with each other; it is evident that the benefits of the therapy persisted over time from the ongoing pursuit of socialisation as means of mutual help and support.
These data are coherent with what the literature on enjoyment of group dance globally convenes [16-18] but in addition they outline a persistency in enjoyment and gratification overtime, as it was suggested by Bergmann (Bergmann 1992), who believed that the potential therapeutic effect of CD consisted in the help given to participants to develop positive concepts of self and self-acceptance.
Limitations and future applications
The size of the reduced sample, the tested varied neurological conditions, and the lack of sample stratification per neurological pathology each represent a specific choice, even though debatable. For that matter other authors [17] considered different manners of evidence necessary to truly capture and explore human cognitive functionalities, as often objective data do not capture the inner personal meaning of some types of experiences [28].
Moreover improvisation, which is an element of dancing, is linked with a system which is non- uniform and non-repeatable and, because of this, more similar to real life: its results are more obvious and sometimes more incisive than routine testing.
Group B distinctly expressed a greater satisfaction (Group A: 14 vs Group B: 25 with p<0.0001) which could be indicative of the enjoyment of the type of dance. Consequently it could be that Group B decided to continue with the treatment because, since it started at most disadvantage, it was also more inclined to pursue alternative methods of treatment [29].
This pilot study lays the groundwork for further in-depth studies in the neurorehabilitation field which will see Creative Dance applied side by side with the traditional treatment approach, with already tested treatment advantages. Certainly it will be necessary to increase the size of the sample and to divide it according to the different types of disabilities to further reduce confounding factors and for a better evaluation of short and long-term benefits.
Conclusion
This study was designed to elaborate alternative strategies to support the rehabilitation of patients with both degenerative and non-degenerative pathologies, to increase the compliance to traditional treatment and prevent the risk of patients not completing the treatment with a consequent worsening of the outcome through time. CD treatment was also used as a support for depression prevention and for the treatment of already existing mood disorders.
A qualitative evaluation of the subjects that continued the double treatment registered an overall psycho-motor improvement and above all a better awareness of their body in the space it occupies accompanied by a new pursuit of strategies to compensate for their inability as well as a total improvement in their mood and socialization skills.
In conclusion, CD, like other types of dancing, seems to help patients with chronic neurological diseases to find their psycho-physical balance.
This pilot study is the premise for further future investigations, which will involve standardizing the protocol as much as possible, increasing the number of treated pathologies, and evaluating the results through time.
References
- Demarin V, Bedekovi? MR, Pureti? MB, Paši? MB (2016) Arts, Brain and cognition. Psychiatria Danubiana 28: 343-348.
- Marmeleira JF, Pereira C, Cruz-Ferreira A, Fretes V, Pisco R, et al. (2009) Creative dance can enhance proprioception in older adults. J Sports Med Phys Fitness 49: 480- 485.
- Stribling K, Christy J (2017) Creative Dance Practice Improves Postural Control in a Child With Cerebral Palsy. Pediatr Phys Ther 29: 365-369.
- Joung HJ, Park J, Ahn J, Park MS, Lee YJ (2020) Effects of creative dance-based exercise on gait performance in adolescents with cerebral palsy. Exerc Rehabil 16: 332-343.
- Cruz-Ferreira A, Marmeleira J, Formigo A, Gomes D, Fernandes J (2015) Creative Dance Improves Physical Fitness and Life Satisfaction in Older Women. Res Aging 37: 837-855.
- Osgood NJ, Meyers BS, Orchowsky S (1990) The Impact of Creative Dance and Movement Training on the Life Satisfaction of Older Adults: An Exploratory Study. Journal of Applied Gerontology 9: 255-265.
- Bergmann S (1992) The Process product dichotomy and its indications for creative dance. Journal of Aesthetic Education 26: 103-108.
- Lewis RN, Scannell ED (1995) Relationship of Body Image and Creative Dance Movement. Perceptual and Motor Skills 81: 155-160.
- Irene E, Gempton R, Poole GD (2000) An Intergenerational Creative Dance Program for Children and Frail Older Gerontology & Geriatrics Education 20: 49-68.
- Dimondstein, Geraldine (1971) Children Dance in the Classroom. Book ERIC.
- Rossberg-Gempton I, John, Gary P (1999) Creative dance: Potentiality for enhancing social functioning in frail seniors and young children. Arts in Psychotherapy - ART PSYCHOTHER 26: 313-327.
- Rossberg-Gempton IE, Poole GD (2008) Creative dance: Potentiality for enhancing social functioning in frail seniors and young Gerontology &Geriatrics Education 20: 49-68.
- Joung HJ, Lee Y (2019) Effect of Creative Dance on Fitness, Functional Balance, and Mobility Control in the Elderly. Gerontology 65:537-546.
- Patterson KK, Wong JS, Prout EC, Brooks D (2018) Dance for the rehabilitation of balance and gait in adults with neurological conditions other than Parkinson’s disease: A systematic Review article Heliyon 4: 00584.
- Solla P, Cugusi L, bertoli M, Cereatti A, Della U, et al. (2019) Sardinian Folk Dance for Individual’s Parkinson’s Disease: A randomized controlled pilot trial. The journal of Alternative and Complementary Medicine 25: -316.
- Marchant DW (2016) Dancing with Disease: A dance’s Reflections on Moving with People with Parkinson’s and Memory Frontiers in Neurology 7 :137.
- Bognar S, DeFaria AM, O'Dwyer C, Pankiw E, Simic Bogler J, et al. (2017) More than just dancing: experiences of people with Parkinson's disease in a therapeutic dance program. Disabil Rehabil 39: 1073-1078.
- Patterson KK, Wong JS, Nguyen TU, Brooks D (2018) A dance program to improve gait and balance in individuals with chronic stroke: A feasibility Top Stroke Rehabil 25:410-416.
- Thornberg K, Josephsson S, Lindquist I (2014) Experiences of partecipation in rhythm and movement therapy after stroke. Disability and Rehabilitation An international multidisciplinary journal 36:1869-1874
- Chen W (2001) Description of an expert teacher's constructivist-oriented teaching: engaging students' critical thinking in learning creative Res Q Exerc Sport 72: 366-375.
- Chen JL, Penhune VB, Zatorre RJ (2008) Listening to Musical Rhythms Recruits Motor Regions of the Brain. Cerebral Cortex 18: 2844-2854.
- Demers M, McKinley P (2015) Feasibility of delivering a dance intervention for subacute Stroke in a Rehabilitation Hospital Setting. Int J Environ Res Public Health 12: 3120-3132.
- Duncan RP, Earhart GM (2014) Are the effects of community-based dance on Parkinson disease severity, balance, and functional mobility reduced with time? A 2-year prospective pilot study. J Altern Complement Med 20: 757-763.
- https://www.sisbio.it/discipline/danza-creativa/
- Kropacova S, Mitterova K, Klobusiakova P, Brabenec L, Anderkova L, et al. (2019) Cognitive effects of dance-movement intervention in a mixed group of seniors are not dependent on hippocampal atrophy. J Neural Transm (Vienna) 126: 1455-1463
- Malosa Sampaio LM, Savitha S, Arena R, Tanvi B (2016) Does virtual reality-based Kinect dance training paradigm improve autnomic Nervous System Modulation in Individuals with Chronic Stroke? JVIN 9: 21-29.
- Mirandola D, Monaci M, Muraca MG, Catallo R, Gulisano M, et al. (2015) Role of dance as part of an adapted physical activity program in breast cancer survivors: A pilot study. Medicina dello sport 68: 591-599.
- Modenesi N (2016) Riabilitango, Recupero post stroke. Ortopedici e sanitari 66.
- Zhu Y, Wang T, Wu H, Qi M, Wang S, et al. (2018) Effects of a specially designed aerobic dance routine on mild cognitive impairment. Clin interv Aging 13: 1691-1700.
Citation: Loi M, Ruisi G, Bossi D, Ghidini R, Magistroni A, et al. (2023) Creative Dance in Neurorehabilitation: A Pilot Study. J Orthop Res Physiother 9: 059.
Copyright: © 2023 Loi M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.