Effectiveness of Nutritional Management of Childhood Obesity in Obese Children Aged 10-16 Years Seen at The Abidjan Heart Institute (Cote D'ivoire)
*Corresponding Author(s):
Mahamat-Azaki OumarInstitut De Cardiologie D’Abidjan, BP 206 Abidjan, Cote D'Ivoire
Email:omrzaki11@gmail.com
Abstract
Context and objective: Obesity is on the rise worldwide and is a public health problem. It is a factor promoting cardiovascular disease, diabetes and other kidney diseases. Obesity affects adults as well as young children. The objective of this study is to determine the consumption of foods rich in sodium and then to propose a weight loss diet. help with local dishes for 48 obese children aged 5-16 received at the Institute of Cardiology of Abidjan.
Methods: A food frequency questionnaire (FFQ) was used to assess dietary intakes and consumption rates of high sodium products in obese children aged 5 to 16 years. Multivariate regression analysis was performed to assess the association between consumption of sodium-rich products and obesity. In addition, a slimming diet has been proposed to children in order to reduce weight gain.
Results: The children consuming meals in the canteen were the most numerous by 63.6% against 36.4% for those who ate lunch at home. The type of food also influenced children’s weight. Thus, fried foods and grilled meats (51.1%) are more prone to obesity than meals in sauce (11.6%). The foods rich in sodium the most consumed were salt, seasoning cubes followed by powdered milk and sodas.
Conclusion: It appears that the majority of sodium consumed would come from powdered and sugary drinks, in addition to cooking salt and seasoning cubes. These products contribute significantly to childhood obesity. Weight reduction in children is possible by reducing both sodium levels in foods and salt.
Keywords
Childhood obesity; Energy Nutritional intake; Sodium intake
Introduction
The number of overweight people in the world is constantly increasing. This phenomenon has been most pronounced in developed countries, particularly the United States, Canada and Korea, where around 30% of the adult population is overweight and 4% is obese [1]. However, its prevalence is also increasing in developing countries [2]. In most countries, with the exception of South Africa, the prevalence of overweight children remains low. The prevalence of obesity was 5% in Côte d'Ivoire in 2012 [3]. In fact, obesity-related medical problems affect a very large number of people, more than 115 million in developing countries [4]. According to the WHO, these disorders will be the leading cause of death among needy populations by 2030 [4]. Obesity is also the main reason for dietary consultations [5]. In many countries, overweight and obesity among children and adults is a major public health problem [1].
Being overweight has been linked to numerous chronic diseases such as cardiovascular disease, kidney disease, type 2 diabetes mellitus, hypertension and hyperlipidaemia. In sub-Saharan Africa, very little data is available on childhood obesity, as the various nutrition and public health initiatives have focused on malnutrition and food security problems. In many developing countries, obesity coexists with malnutrition [3,5]. This represents a double burden for these countries, whose efforts to overcome these problems must be carefully balanced.
There was therefore no data on the management of childhood obesity. Also, despite the presence of numerous dietary programmes, few have been systematically studied. It is therefore crucial to research the real causes of childhood obesity, and specifically the role played by sodium-rich foods in the onset of this obesity.
Materials and Methods
Setting, type and period of the study
This is a retrospective study with an analytical aim running from February to July 2021 in the nutrition department of the Abidjan Heart Institute. During this period, dietary trials were proposed to high body weight patients by modifying their usual diet when necessary.
Study population
The study population consisted of 48 obese children who were referred to the dietetics department of the Abidjan Heart Institute (AHI) after being declared overweight by their parents.
Selection criteria
The study included all obese children and adolescents who had not taken any medication that affected their lipid profile. Obese children over 16 years of age were not included in the study.
Data collection
Data from the medical records of patients taken from the archives during the study period were recorded on a previously prepared survey form.
Dietary survey
The recommendations were presented during individual consultation sessions. The volunteers were accompanied and helped by their parents. Volunteers were asked about their usual diets by answering an elaborate questionnaire on local foods, in particular foods rich in sodium. Questionnaires focusing on the type of breakfast, lunch and dinner were used. The survey also covered the type of meal, the number of meals and the type of drink. The food frequency questionnaire was used to assess their food intake, particularly the rate of consumption of sodium-rich products. Eating habits were assessed using the dietary survey method.
This section covers eating behaviour and habits, places, duration and number of meals, preferred food tastes and frequency of consumption of the main meals.
Frequency of consumption was collected by interviewees responding directly to multiple-choice questions : every day, sometimes (3 to 4 times a week), rarely (1 to 2 times a week) or never (0 times a week). The composition of breakfast was collected by answering an open question. The child indicated the foods usually eaten during this meal. The composition of lunch and dinner was collected by a direct response from the child to multiple choice questions : meat, fish, chicken, fruit, vegetables. The composition of snacks and morning snacks was collected by interviewees responding directly to open-ended questions.
The composition of snacking, which is considered to be any food eaten outside the main meals (breakfast, lunch, afternoon snack and dinner), was obtained by the child's direct response to a multiple-choice question.
The diet errors were then explained to them and they were given advice for 30 to 45 minutes to change their experiment.
Measurement of anthropometric parameters
Anthropometric measurements (height, weight, body mass index) were measured at the Heart Institute using the method of Kweon et al, [6].
Measurements were taken at T0, 15 days after T0 (T1), 45 days after T1 (T2), 45 days after T2 (T3) and 45 days after T3 (T4). Height was measured to the nearest 0.1 cm using a Seca 225 (Germany Seca Ltd.), and weight was measured to the nearest 0.1 kg using a GL-6000-20 (Korea G-tech Ltd.). Body mass index (BMI) was calculated using the height and weight data according to the following equation: BMI (kg/m²) = weight (kg)/taille² (m²).
Food formulation (diet)
Low-calorie diet: Meals with sauce contain less energy than meals without sauce. The diet included less red meat, more poultry and fish, which are by nature less salty, and the midday meal consisted mainly of vegetable and leaf sauce, with fruit consumption limited to just one in our study.
Low-salt diet: In our recommendations, meals with a higher salt content were banned, such as powdered milk, coconut water, soda, homemade juices, carrots and salted broths. Industrial meat products such as sausages, jerky, etc. were also banned. During diet therapy, fish and poultry were used more than meat.
Low carbohydrate diet; In the morning, to avoid anaemia, breakfast consisted of 1/3 bread with eggs, or meat, or avocado, or beef liver.
Impact of diets on body weight.
The impact of the diets was monitored by comparing weight and BMI at first contact T0, T1 (15 days after T0), T2 (45 days after T1), T3 (45 days after T2) and T4 (45 days after T3).
Data analysis
Multivariate regression analysis was conducted to assess the association between sodium-rich products and obesity. Results were expressed as mean with extremes for quantitative variables ; and as percentage for qualitative variables.
Results
Distribution of patients by age
The average age of respondents was 10.7 ± 2.7 years, with extremes of 5 and 16 years. The median age was 11 years.
Distribution of subjects by sex
There were as many women as men in this study: 24 girls and 24 boys.
Eating habits and practices
(Table 1) shows the contribution of sodium-rich foods to the eating habits of the respondents. The results show that all the people questioned said that they always consumed salt and seasoning broths. Consumption of freshly squeezed juice and milk powder was the same at 95.7%. Sausage was eaten 3 times a week in 66.7% of cases. Carrots were eaten by 62.2%.
Breakfast was also eaten by 100% of subjects. The results also showed that 97.7% of those surveyed ate lunch regularly.
|
|
Always |
3 times a week |
Sometimes |
Rarely |
Never |
|
Homemade juice |
44 (95.7%) |
2(4.4%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
|
Soda |
9(20.9%) |
12(27.99%) |
15(34.9%) |
5(11.6%) |
2(4.7%) |
|
Sausage |
2(11.1%) |
12(66.7%) |
3(16.7%) |
1(5.6%) |
0(0.0%) |
|
Powdered milk |
45(95.7%) |
2(4.3%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
|
Carrot |
3(6.7%) |
2(4.4%) |
5(11.1%) |
28(62.2%) |
7(15.6%) |
|
Cooking salt |
47(100%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
|
Seasoning cube |
47(100%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
0(0.0%) |
Table 1: Frequency consumption of products rich in sodium.
Weight loss during weight loss diet
The weight loss of the patients having followed the slimming diet is observed in (Figure 1). Two (2) weeks after the start of the diet, an average loss of 2 kg was indicated passing from 77.40 ± 20.75 kg at T0 to 75.52 ± 20.53 kg at T1. At T1, the weight drops to 72.76 ± 19.7 kg at T2 in with an average loss of 5 kg from the initial weight. On the T3 date, 105 days after the start of the diet, an average of 7 kg of loss was observed (77.40 ± 20.75 kg to ????? kg). After, 150 days of diet (T4), the final weight is 69.13 ± 18.18 kg. These are nearly 8 kg of weight lost in 150 days for low-calorie and low-sodium diet.
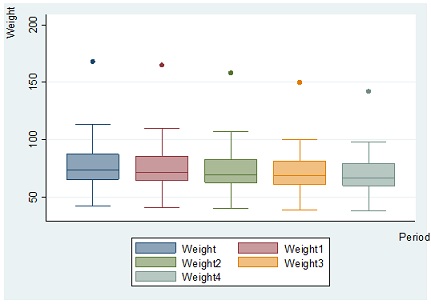 Figure 1: Weight loss during weight loss diet.
Figure 1: Weight loss during weight loss diet.
Decrease in Body Mass Index during dieting
(Figure 2) shows the decrease of Body Mass Index (BMIs) at different periods. There are, therefore, significant statistical differences in BMI between the different comparisons (P = 0.0000, <5%). On average, during the first 2 weeks, the BMI drops from 34.01 ± 7.15 to 33.02 ± 7.08, a reduction of 3%. This result remains almost constant during dieting period.je ne vois pas la constance. Essaie de revoir stp
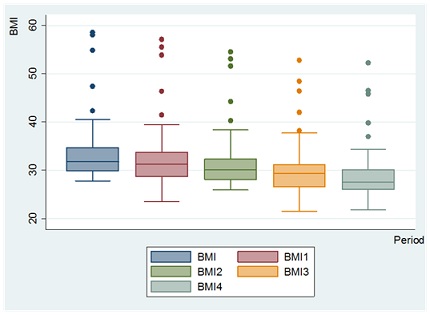 Figure 2: Decrease in BMI during dieting.
Figure 2: Decrease in BMI during dieting.
Discussion
The aim of this study was to improve the health of children. Forty-eight (48) high-weight volunteers (25 to 97 kg) aged 10.7 ± 2.7 years participated in the study. These patients were not taking any medication known to affect lipid metabolism according to clinical practice.
With regard to socio-demographic characteristics, the results showed that there were as many girls as boys (50%). Subjects aged over 10 years were the most numerous (60%). The minimum age was 4 and the maximum was 16.
The results obtained were identical to those of Grimes et al [7], who found a proportion of 51.7% of male subjects compared with 48.3% of female subjects. However, 52% of the subjects were aged over 9 years.
The results of the food consumption survey, which focused on sodium-rich foods and the types of food consumed, showed that in addition to cooking salt and seasoning cubes, milk powder and sweetened drinks were the predominant foods.
In fact, all the children (100%) consumed salt and seasoning cubes on a daily basis. Cooking salt and bouillon (seasoning cubes) were the foods most used by the whole population in all kitchens, and milk powder was used most for breakfast.
Numerous studies have shown that salt increases appetite and that there is a significant association between sodium intake and obesity [8,9].
Dietary salt intake predicts total fluid intake and soft drink consumption among consumers of soft drinks. Consumption of soft drinks is associated with the risk of obesity [7].
In this study, sodium came from both parental choices (salt, seasoning cubes and homemade juice) and choices more or less related to the children themselves, in particular milk powder and soft drinks. Consuming milk powder and homemade fruit juice is important for health. Children with higher urinary sodium excretion had a higher BMI in both sexes and greater parental obesity than those with lower urinary sodium excretion. The study suggests a close relationship between children's obesity and their sodium intake, which also correlates well with parental BMI and eating behaviour. Consequently, parental education and active participation could be crucial in regulating childhood obesity. The World Health Organization currently recommends a daily intake of less than 5 grams of salt [10].
In low- and middle-income countries where people may have limited access to processed foods, salt added at home, during cooking or at the table, accounts for the majority of dietary salt [10].
With regard to the place where food is consumed, the survey showed that there were more cases of childhood obesity among children eating their meals in school canteens than among people eating their lunch at home. The location of the lunch was also a determining factor in the fight against childhood obesity. All these results can be explained by the lack of control over the school environment, whether in the canteen or in the surrounding sales areas, and the low consumption of fruit and vegetables, while the consumption of fizzy drinks is increasing [11].
This could also be due to a lack of satisfaction linked to the unavailability of food for consumption in the school canteen. This could lead teenagers to prefer going to the shops to buy cheaper and more desirable foods. The responsibility of parents in the development of childhood obesity is indisputable, particularly in the choice of menus at home.
As for food preferences, survey results have also shown that children prefer meals without sauces, such as fried and grilled foods. These behaviours are linked to the nutritional transition, which is leading patients to abandon traditional foods and take advantage of imported menus. Indeed, with the nutritional transition, traditional menus tend to disappear. Nutritional transition leads to the abandonment of raw, unprocessed cereals and tubers in favour of an ultra-processed diet richer in animal proteins and with added sugars and fats in certain foods such as fried foods, grilled meats, soft drinks and sausages [12].
With regard to the nutritional management strategy used in this study, the effects, particularly weight loss, were observed on a regular basis. This precaution is very important in order to avoid the trauma associated with a change of diet. The aim of the study was to reduce body mass, the results obtained can be explained by a number of factors, including the reduction in the energy content of food and the reduction in salt.
The reduction in energy intake involved replacing grilled and fried foods with sauces. Meals in sauce are lower in calories because they have been prepared with leaves and vegetables without fat but with water as in African dishes [5]. This amount of sauce leads to satiety with low energy.
Previous research has indicated that increasing the volume of food by adding water can lead to affecting satiety and food intake. However, the addition of water affects not only the volume but also the energy density (kJ/g) of foods [13]. Fibre-rich foods are known to affect satiety and fullness [14] and to suppress hunger and reduce food intake [15].
The proposed diet was also based on a sauce with a lower salt content in order to reduce energy intake. Indeed, Bolhuis [16] had shown that the addition of sodium chloride (salt) increases the palatability of many foods by encouraging greater energy intake. These results were also observed by Grimes et al [17]. The results of their research showed that a diet richer in sodium can increase fluid intake. In short, sodium intake is strongly correlated with energy intake. According to the WHO [18], there are two key strategies for reducing sodium intake in the population : voluntary or mandatory reformulation strategies and communication with consumers to educate, raise awareness and motivate them to make desirable behavioural changes [8].
In addition, it should be considered that reformulation policies aimed at reducing salt in manufactured foods can be very cost-effective. According to the study carried out by these authors, the strategies indicated could be applied to reduce sodium content not only in products and foods with a high concentration of sodium (for example, meats with visible fat or fried meats, fried chicken, sauces, processed meats and sausages), but also in those with a moderate sodium content, such as deep-fried pastries, sandwiches, fast food, cereals, 'gallo pinto', salted seeds, salted biscuits, snacks in small packets and popcorn, among others.
The American Heart Association (AHA) has also recommended education on nutrition and physical exercise. In terms of nutrition, the emphasis should be on a diet rich in fibre, fruit, vegetables, fish and foods low in saturated fats, trans fats, cholesterol, salt (sodium) and added sugars. The American Heart Association also recommends 60 minutes of physical exercise a day [19]. Several studies have highlighted the beneficial effects of salt reduction. Population-based approaches to dietary salt reduction can be effective in developed countries and have shown promising results in reducing blood pressure [20].
Conclusion
The aim of this study was to improve children's health through weight loss by means of a diet at the Abidjan Heart Institute. The results showed that the majority of adolescents (63.63%) in this study use the school canteen. They preferred fried and grilled foods to meals with sauce [21]. They also consume cooking salt and seasoning cubes every day, and often powdered milk, sweet drinks and sausages. Apart from cooking salt and seasoning cubes, powdered milk and sweet drinks are the foods that contribute most to sodium consumption in Côte d'Ivoire. Reduce sodium-rich foods such as powdered milk and fruit juices, and choose low-energy foods such as sausages [22]. Improving eating habits, particularly by reducing salt intake during childhood, will have beneficial effects on health, including the prevention of arterial hypertension [7].
References
- Fleming T, Ng M, Robinson B, Graetz N, Margono C, et al. (2014) Global Regional and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384: 766-781.
- Abubakari AR, Lauder W, Agyemang C, Jones M, Kirk A, et al. (2008) Prevalence and time trends in obesity among adult West African populations: a meta-analysis. Obes Rev 9: 297-311.
- Kramoh KE, N’goran YN, Aké-Traboulsi E, Boka BC, Harding DE, et al. (2012) Prévalence de l’obésité en milieu scolaire en Côte d’Ivoire. Annales de Cardiologie et d’Angéiologie 61: 145-149.
- OMS (2006) Le défi de l’obésité dans la Région européenne de l’OMS et les stratégies de lutte EUR/06/5062700/6 Conférence ministérielle européenne de l’OMS sur la lutte contre l’obésité. Istanbul Turquie.
- Chubike NE, Okaka JC, Okoli EC (2013) Evaluation of vegetable consumption in South Eastern Nigeria. International Journal of Nutrition and Metabolism 5: 57-60.
- Correia J, Pataky Z, Golay A (2014) Comprendre l’obésité en Afrique : poids du développement et des représentations. Rev Med Suisse 10: 712-6.
- Ohta Y, Iwayama K, Suzuki H, Sakata S, Hayashi S, et al. (2016) Salt intake and eating habits of school-aged children. Hypertens Res 39: 812-817.
- Nunez-Rivas H, Holst-Schumacher I, Blanco-Metzler A, de los Angeles Montero-Campos M, Campos-Saborío N, et al. (2020) Salt/Sodium Intake Estimation in Children and Adolescents of Costa Rica. Food and Nutrition Sciences 11: 919-941.
- Grimes CA, Wright JD, Liu K, Nowson CA, Loria CM (2013) Dietary sodium intake is associated with total fluid and sugar-sweetened beverage consumption in US children and adolescents aged 2-18 y: NHANES 2005-2008. Am J Clin Nutr 98: 189-96.
- Campbell NR, Johnson JA, Campbell TS (2012) Sodium Consumption: An Individual’s Choice? Int J Hypertens 2012: 860954.
- Näslund E, Barkeling B, King N, Gutniak M, Blundell JE, et al. (1999) Energy intake and appetite are suppressed by glucagon-like peptide-1 (GLP-1) in obese men. Int J Obes Relat Metab Disord 23: 304-311.
- Drewnowski A, Popkin BM (1997) The nutrition transition: new trends in global diet. Nutr Rev 55: 31-43.
- Rolls BJ, Bell EA, Thorwart ML (1999) Water incorporated into a food but not served with a food decreases energy intake in lean women. Am J Clin Nutr 70: 448-55.
- Burley VJ, Paul AW, Blundell JE (1993) Influence of a high-fibre food (myco-protein) on appetite: effects on satiation (within meals) and satiety (following meals) Eur J Clin Nutr 47: 409-418.
- Van ittalie TB (1978) Dietary fiber and obesity. Am J Clin Nutr 31: S43-S52.
- Bolhuis DP, Lakemond CM, de Wijk RA, Luning PA, de Graaf C (2012) Effect of salt intensity in soup on ad libitum intake and on subsequent food choice. Appetite 58: 48-55.
- Grimes CA, Riddell LJ, Campbell KJ, Nowson CA (2013) Dietary Salt Intake, Sugar-Sweetened Beverage Consumption, and Obesity Risk. Pediatrics 131: 14-21.
- Taleb S (2013) Obésité des enfants scolarisés à Tébessa (1995-2007). Prévalence, Comportement alimentaire et facteurs socio-économiques [Thèse de doctorat, Université Mentouri de Constantine].
- Blasingame T (2017) Addressing Childhood Obesity with Education. J Child Obes 2: 11.
- Rolland-Cachera MF (2018) Apports lipidiques pendant la période périnatale ; relation avec l’obésité de l’enfant et du futur adulte. OCL 25: D307.
- Tremblay MS, Willms JD (2000) Secular trends in the body mass index of Canadian children. CMAJ 163: 1429-33.
- Tounian P (2007) l’obésité de l’enfant. Edition John Libbey Eurotext, ISBN 2742005498, 9782742005499 196 pages.
Citation: Mahamat-Azaki O, Yves A, Benedicte B, Arnaud E, Christelle G, et al. (2023) Effectiveness of Nutritional Management of Childhood Obesity in Obese Children Aged 10-16 Years Seen at The Abidjan Heart Institute (Cote D'ivoire). J Pract Prof Nurs 7: 045
Copyright: © 2023 Mahamat-Azaki Oumar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.