Effects of Pulmonary Nodules on Patient Anxiety and Health-Related Quality of Life
*Corresponding Author(s):
Xueling WuDepartment Of Pulmonology, Renji Hospital, Shanghai Jiaotong University School Of Medicine, Shanghai, P.R., China
Tel:+86 021 3450 6271,
Email:wuxueling76@126.com
Xiaoming Tan
Department Of Pulmonology, Renji Hospital, Shanghai Jiaotong University School Of Medicine, Shanghai, P.R., China
Tel:+86 021 3450 6271,
Email:tanxiaomingfsh@163.com
Yu Zheng
Department Of Pulmonology, Renji Hospital, Shanghai Jiaotong University School Of Medicine, Shanghai, P.R., China
Tel:+86 021 3450 6271,
Email:dr-_zhengyu@163.com
Abstract
Objective: The purpose of this study was to examine the psychological and health status of patients with pulmonary nodules.
Methods: We conducted a cross-sectional study of the incidental pulmonary nodules in adults.
Results: Female patients were more anxious than male patients (P = 0.036). Univariate analysis indicated that the size of the pulmonary nodules (P = 0.041), having seen the pulmonary nodules (P = 0.001), and doctors having said that pulmonary nodules are common (P = 0.006) could influence anxiety in patients. Multivariate analysis found that age (P = 0.010), monthly income (P = 0.014), nodule size (P = 0.038), and having seen the pulmonary nodules on Computed Tomography (CT) (P = 0.002) can affect the anxiety levels of patients. The five-level EuroQol 5-dimension (EQ-5D-5L) utility score was 0.9578 ± 0.0634, and the EQ-5D-5L utility was negatively correlated with the Impact of Event Scale-Revised (IES-R) score (R = −0.3495, P < 0.0001).
Conclusion: Female patients were more anxious than male patients. If patients have seen the pulmonary nodules on CT themselves, this can increase the anxiety levels. If a doctor has told a patient that pulmonary nodules are common before CT imaging, this can reduce the anxiety levels. The evaluation of the health-related quality of life of patients with pulmonary nodules with the EQ-5D-5L utility is acceptable, but its value is negatively correlated with the IES-R score.
Keywords
Anxiety; Communication; Pulmonary nodules; Questionnaire; Survey
Abbreviations
CT: Computed Tomography
EQ-5D-5L: five-level EuroQol 5-Dimension
IES-R: Impact of Event Scale-Revised
HRQOL: Health-Related Quality of Life
Introduction
With the popularization of Computed Tomography (CT) screening for lung cancer, the detection rate of pulmonary nodules is increasing [1]. Most pulmonary nodules do not develop into lung cancer [2], but most patients with pulmonary nodules undergo more than 2 years of follow-up to ensure that pulmonary nodules are not enlarged [3]. However, most pulmonary nodules do not eventually develop into lung cancer [4]. During the first discovery and long-term follow-up, the psychological pressure on patients can be high. The Impact of Event Scale-Revised (IES-R) is a self-assessment scale based on 22 questions, which is commonly used in screening anxiety and depression [5]. We screened patients with pulmonary nodules for anxiety and depression with the IES-R scale to find out (i) The psychological state of patients with pulmonary nodules and (ii) Whether these patients need psychological intervention treatment, because anxiety and depression disorders are related to significantly lower Health-Related Quality of Life (HRQOL). The five-level EuroQol 5-Dimension (EQ-5D-5L) utility is a frequently used generic measure of the HRQOL, which captures mental health through a single domain, that is, the anxiety/depression dimension. It can be used in clinical and economic evaluations of healthcare, and in assessing public health [6]. Therefore, we also included EQ-5D-5L in this study. Based on the above studies, we hypothesized that the prevalence of anxiety and depression in patients with pulmonary nodules is high, and their mental health is affected to varying degrees. Effective communication between doctors and patients about pulmonary nodules can reduce the degree of anxiety and depression. We (i) Characterized the prevalence of anxiety and depression in patients with pulmonary nodules and (ii) Identified the risk factors for anxiety.
Methods
Participants were pulmonary nodules patients admitted to the Renji Hospital South Campus between July 2018 and July 2019. Inclusion criteria were the following: Newly reported, incidental (not screen-detected) nodules less than 3 cm in diameter, with plans for non-urgent CT follow-up. Exclusion criteria were the following: Living in a nursing facility, has been diagnosed with lung cancer, mental illness or cognitive impairment, and terminal illness. A total of 178 patients met the criteria and were included. The participants answered the questionnaire we designed face-to-face.
Questionnaire Design
We designed a questionnaire to assess the psychological and health status of patients with pulmonary nodules, which included: (i) Basic clinical characteristics; (ii) Communication between doctors and patients about pulmonary nodules; (iii) The IES-R scale; and (iv) The EQ-5D-5L utility, which is comprised of five domains, that is, mobility, self-care, usual activities, pain/discomfort and emotions [6]. Scores for the different domains range from 1 to 5, where a high score indicates a low quality of life [7]. The EQ-5D-5L score was calculated after the construction of the EQ-5D-5L profile. The integral EQ-5D-5L utility system based on Chinese population preferences was adopted [8]. Before implementation of the questionnaire, it was evaluated by three experts in lung cancer-related and statistics-related fields. Ten patients with pulmonary nodules who met the criteria initially took the questionnaire. The final questionnaire contained 38 questions. The participants answered the questionnaire face to face.
Data Analyses
Data were checked and cleaned using SPSS version 25.0 and Prism 6.0 prior to analysis. Descriptive analysis was used to determine the overall patient IES-R score, the EQ-5D-5L score, and participants’ clinical outcomes. One-way ANOVA was used to compare the IES-R score between different groups. Univariate and multivariate logistic regression analyses were performed to determine the risk factors of anxiety. The correlation of the IES-R score with the EQ-5D-5L score was established by the Pearson correlation coefficient test. All data are presented as mean ± Standard Deviation (SD). A P-value < 0.05 was considered to indicate statistical significance in all statistical analyses.
Results
Basic clinical characteristics
A total of 178 patients met the inclusion and exclusion criteria. The questionnaire included questions about whether friends or relatives had lung cancer, smoking status, education, monthly income, marital status, whether they had children attending school, and the size of pulmonary nodules. Patient characteristics such as age and sex are shown in table 1. One-way ANOVA showed a difference in IES-R score between sexes; female patients are more anxious (P = 0.036). No significant difference in IES-R score was found for other factors (P > 0.05). We analyzed the independent risk factors for anxiety, as assessed by IES-R, by logistic regression analyses. The results are shown in table 2.
|
|
Overall N = 178 |
|
Gender,%* Male/female |
43.8%/56.2% |
|
Mean age, years (SD) |
51 (13.2) |
|
Friends or family with lung cancer, % |
|
|
Yes/no |
21.3%/78.7% |
|
Smoking status, % |
|
|
No, but with smoking history Yes No |
14.0% 20.8% 65.2% |
|
Highest education,% |
|
|
Illiteracy Primary school Junior high school Senior high school College or higher |
3.4% 12.9% 34.8% 20.8% 28.1% |
|
Monthly income,% |
|
|
Less than 3000 RMB (approx. 425 USD) 3000-6000 RMB (425-850 USD) 6000-10000 RMB (850-1400 USD) More than 10000 RMB (approx. 1400 USD) |
30.9% 36.0% 21.3% 11.8% |
|
Marriage,% |
|
|
Unmarried Married Divorced |
4.5% 93.8% 1.7% |
|
Children in school,% Yes/no |
32.6%/67.4% |
|
Time since nodule detection,% Less than 1 day 0-3 months 3-6 months 6-12 months More than 12 months |
26.4% 11.2% 10.1% 9.0% 43.3% |
|
Nodule size,% Less than 3 mm 3-6 mm 6-8 mm More than 8 mm |
29.8% 50.0% 15.2% 5.1% |
Table 1: Clinical characteristics of patients with pulmonary nodules (N = 178).
*Female patients are more anxious than male patients, as indicated by one-way ANOVA of the Impact of Event Scale-Revised scores (P = 0.036).
|
|
Moderate |
Severe |
Moderate |
Severe |
|
|
Univariate regression analysis OR (95% CI), P-value |
Multivariable regression analysis OR (95% CI), P-value |
||
|
Gender |
1.704 (0.912-3.181), 0.095 |
2.378 (0.755-7.495), 0.139 |
1.990 (0.996-3.977), 0.051 |
3.014 (0.805-11.283), 0.101 |
|
Age |
1.003 (0.980-1.027), 0.786 |
0.973 (0.934-1.014), 0.197 |
0.990 (0.961-1.020), 0.498 |
0.930 (0.880-0.983), 0.010 |
|
Friends or family with lung cancer |
0.636 (0.299-1.355), 0.241 |
1.556 (0.317-7.634), 0.586 |
|
|
|
Smoking status |
1.147 (0.755-1.744), 0.519 |
1.648 (0.692-3.920), 0.259 |
|
|
|
Highest education |
0.994 (0.755-1.307), 0.964 |
0.936 (0.581-1.507), 0.785 |
|
|
|
Monthly income |
0.793 (0.579-1.086), 0.147 |
0.642 (0.356-1.158), 0.141 |
0.791 (0.531-1.179), 0.250 |
0.374 (0.171-0.818), 0.014 |
|
Marital status |
1.042 (0.293-3.701), 0.949 |
0.583 (0.080-4.264), 0.595 |
|
|
|
Children in school |
1.091 (0.562-2.118), 0.797 |
0.618 (0.206-1.851), 0.390 |
|
|
|
Time since nodule detection |
1.092 (0.911-1.310), 0.342 |
1.098 (0.797-1.511), 0.569 |
|
|
|
Nodule size |
0.845 (0.568-1.257), 0.405 |
1.914 (1.027-3.567), 0.041 |
0.869 (0.567-1.333), 0.521 |
2.081 (1.042-4.159), 0.038 |
|
Doctors pointing out the size of the pulmonary nodules |
0.900 (0.454-1.785), 0.763 |
1.125 (0.326-3.879), 0.852 |
|
|
|
Having seen the pulmonary nodules on CT |
3.070 (1.594-5.912), 0.001 |
1.139 (0.388-3.345), 0.813 |
3.091 (1.515-6.305), 0.002 |
1.319 (0.390-4.467), 0.656 |
|
Doctors having made clear the possibility of lung cancer |
0.774 (0.267-2.245), 0.637 |
1.232 (0.236-6.432), 0.804 |
|
|
|
Doctor having clearly pointed out the uncertainty of pulmonary nodules |
0.771 (0.389-1.529), 0.457 |
2.839 (0.946-8.523), 0.063 |
1.187 (0.555-2.541), 0.659 |
3.149 (0.912-10.871), 0.070 |
|
Doctors having said pulmonary nodules are common |
0.404 (0.211-0.774), 0.006 |
1.320 (0.446-3.901), 0.616 |
0.514 (0.252-1.045), 0.066 |
0.979 (0.290-3.297), 0.972 |
Table 2: Univariate and multivariate regression analyses of risk factors for anxiety and depression among patients with pulmonary nodules.
Doctor-patient communication on issues related to pulmonary nodules
We investigated whether communication between doctors and patients on pulmonary nodules prior to the discovery of the nodules could reduce anxiety in patients after the discovery of pulmonary nodules. Therefore, several statements about doctor-patient communication on pulmonary nodules were included in the questionnaire: (i) Your doctor pointed out pulmonary nodules are common. (ii) Your doctor pointed out the uncertainty of pulmonary nodules. (iii) Your doctor clearly pointed out the possibility of lung cancer. (iv) You have seen the pulmonary nodules on CT. (v) Your doctor informed you of the size of the pulmonary nodules. The proportions of patients who answered positively are shown in figure 1. The most common communications between doctors and patients were the doctor informing the patient of the size of the pulmonary nodules and the patient seeing the pulmonary nodules on CT.
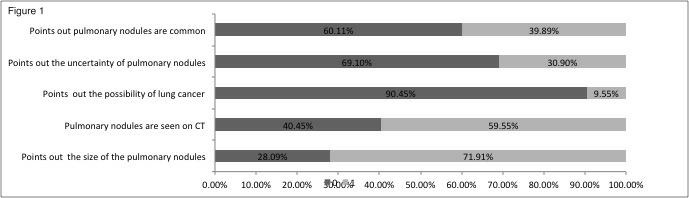 Figure 1: Doctor-patient communication about pulmonary nodules prior to the discovery
Figure 1: Doctor-patient communication about pulmonary nodules prior to the discovery
Assessment of anxiety
We further assessed the levels of anxiety in 178 patients with pulmonary nodules. The results are shown in table 3. Scores range from 0 to 75. The higher the score, the greater the anxiety (Shortened time interval between colorectal cancer diagnosis and risk testing for hereditary colorectal cancer is not related to higher psychological distress). In previous cancer-related pain studies, 17-20 we used the recommended categories: Normal (score 0-8) or mild (score 9-25), moderate (score 26-43) or severe (score 44-75), and clinical anxiety was defined as moderate or severe (score above 26). We found that most patients with pulmonary nodules had mild or moderate anxiety.
|
Anxiety |
Total (N = 178) |
|
Subclinical, n (%) |
0 (0) |
|
Mild, n (%) |
77 (43.26) |
|
Moderate, n (%) |
85(47.75) |
|
Severe, n (%) |
16 (8.99) |
Table 3: Anxiety based on the IES-R score of pulmonary nodule patients.
The univariate and multivariate logistic regression analysis results of clinical characteristics and doctor-patient communication affecting anxiety are summarized in table 2. Because mild anxiety does not need further intervention, we conducted logistic regression analysis on the risk factors of patients with moderate and severe anxiety. We found that the size of the pulmonary nodules (OR, 1.914; 95% CI, 1.027-3.567; P = 0.041), having seen the pulmonary nodules (OR, 3.070; 95% CI, 1.594-5.912; P = 0.001), and doctors having said that pulmonary nodules are common (OR, 0.404; 95% CI, 0.211-0.774; P = 0.006) could influence anxiety in patients. Multivariate regression analysis was carried out for the factors with P < 0.2 in the univariate regression analysis. Age (OR, 0.930; 95% CI, 0.880-0.983; P = 0.010), monthly income (OR, 0.374; 95% CI, 0.171-0.818; P = 0.014), nodule size (OR, 2.081; 95% CI, 1.042-4.159; P = 0.038), and having seen the pulmonary nodules on CT (OR, 3.091; 95% CI, 1.515-6.305; P = 0.002) can affect the anxiety levels of patients.
The EQ-5D-5L utility and the correlation between EQ-5D-5L and IES-R scores
Finally, we evaluated the EQ-5D-5L score for all patients with pulmonary nodules. The EQ-5D-5L score was 0.9578 ± 0.0634. Our correlation analysis between the EQ-5D-5L and IES-R scores revealed that the EQ-5D-5L score was negatively correlated with the IES-R score (r = −0.3495, p < 0.0001), as shown in figure 2.
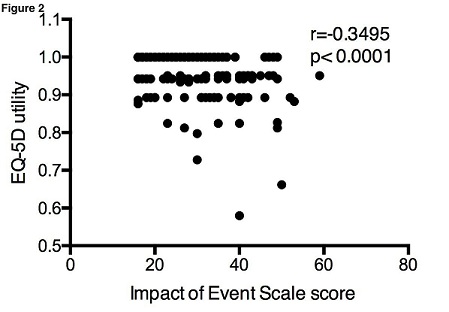 Figure 2: Correlation between IES-R and EQ-5D-5L scores of pulmonary nodule patients
Figure 2: Correlation between IES-R and EQ-5D-5L scores of pulmonary nodule patients
Discussion
As far as we know, this is the first study in China to assess the mental state and the HRQOL of patients with pulmonary nodules. The degree of anxiety and depression of 178 patients with pulmonary nodules is shown in table 3. We found that most patients with pulmonary nodules had mild or moderate anxiety. Female patients were more anxious than male patients, as assessed by the IES-R score. No statistical difference was observed between the IES-R scores for other factors. Our univariate regression analysis revealed that large nodule diameters are associated with higher anxiety levels. Seeing pulmonary nodules on CT can increase the anxiety levels, and if doctors have said that pulmonary nodules are common, this can alleviate anxiety. Our multivariate regression analysis showed that young age, low monthly income, and large nodule diameter are associated with higher anxiety levels. Seeing pulmonary nodules on CT can lead to increased anxiety levels, as shown in table 2. These results are consistent with previous studies on mental health and the HRQOL in pulmonary nodule patients [9-11]. Studies have shown that patients often receive inaccurate information about pulmonary nodules [12,13]. Therefore, good communication between doctors and patients about pulmonary nodules may alleviate anxiety. However, our results are not in agreement with those from previous studies [14,15]. We found that when patients see the pulmonary nodules on CT themselves, this can increase the anxiety levels in patients, as shown by both univariate and multivariate regression analyses. When doctors have told patients that pulmonary nodules are common, this can reduce the anxiety levels. Therefore, doctors are advised to inform patients before the CT scan that the detection rate of pulmonary nodules is relatively high and that most nodules are benign, as this can reduce patient anxiety. Larger nodule diameters are associated with higher anxiety levels; this may be related to the knowledge of popular science among patients and the information doctors provide on different treatment schemes for pulmonary nodules of different sizes.
Studies have shown that lung nodules found during lung cancer screening can increase anxiety and depression in patients and affect the HRQOL. The National Lung Screening Trial (the largest study of lung cancer screening) indicated that there was no significant difference in anxiety and HRQOL between patients with lung nodules screened and those with normal lung nodules screened [9]. We found no significant difference in IES-R score between patients with different periods of time since the pulmonary nodule detection, which is consistent with the results of the National Lung Screening Trial study. This result further supports the importance of lung cancer screening and follow-up monitoring of pulmonary nodules.
Finally, we applied the EQ-5D-5L scale to assess the HRQOL in patients with pulmonary nodules. All of the algorithms were found to overestimate the EQ-5D-5L score for low HRQOL (<0.5) and underestimate the score near full health (≥0.9). We found an EQ-5D-5L score in patients with pulmonary nodules of 0.9578 ± 0.0634, which is basically at a normal level. We found a significant negative correlation between the IES-R and EQ-5D-5L scores in patients with pulmonary nodules. The EQ-5D-5L utility is an assessment tool to estimate the HRQOL. It provides a score, which can be used to calculate the quality-adjusted life year score and to evaluate the incremental cost-effectiveness ratio [16]. The EQ-5D-5L utility was used to assess the HRQOL before and after operation for non-small-cell lung cancer [17] and for chronic obstructive pulmonary disease [18]. We introduced the EQ-5D-5L utility for the first time to assess the mental status and the HRQOL of patients with acute pulmonary nodules in the late stage.
Conclusion
We found that the degree of anxiety varied between different genders; female patients are more anxious than male patients. When patients themselves have seen the pulmonary nodules on CT, this can increase anxiety levels and when doctors have told patients that pulmonary nodules are common, this can reduce anxiety levels. The EQ-5D-5L utility can be used to evaluate the mental status and the HRQOL in patients with pulmonary nodules, but in this study its score was negatively correlated with the IES-R score, so further research is needed.
Ethical approval
This study was approved by the Institutional Review Board of Renji Hospital (2018056).
Acknowledgment
Not applicable
Funding
This work was supported by a study on the diagnosis and treatment strategy of interstitial lung disease associated with connective tissue in diagnostic bronchoscopy (No PYI-17-009) and Multi disciplinary clinical study on precise treatment of COPD based on imaging phenotype (2019NYLYCP0103).
Competing interests
The authors confirm that there are no conflicts of interest.
References
- Gould MK, Tang T, Liu IL, Lee J, Zheng C, et al. (2015) Recent trends in the identification of incidental pulmonary nodules. American journal of respiratory and critical care medicine 192: 1208-1214.
- Humphrey LL, Deffebach M, Pappas M, Baumann C, Artis K, et al. (2013) Screening for lung cancer with low-dose computed tomography: A systematic review to update the US Preventive services task force recommendation. Annals of internal medicine 159: 411-420.
- Ko JP, Azour L (2018) Management of incidental lung nodules. Seminars in ultrasound, CT, and MR 39: 249-59.
- Gould MK, Fletcher J, Iannettoni MD, Lynch WR, Midthun DE, et al (2007) American college of chest p. evaluation of patients with pulmonary nodules: When is it lung cancer? ACCP evidence-based clinical practice guidelines (2nd edition). Chest 132: 108S-1830S.
- Joseph S (2000) Psychometric evaluation of horowitz's impact of event scale: A review. Journal of traumatic stress 13: 101-113.
- EuroQol G (1990) EuroQol-a new facility for the measurement of health-related quality of life. Health policy 16: 199-208.
- Lamers LM, Bouwmans CA, Van Straten A, Donker MC, Hakkaart L (2006) Comparison of EQ-5D and SF-6D utilities in mental health patients. Health economics 15: 1229-1236.
- Luo N, Liu G, Li M, Guan H, Jin X, et al. (2017) Estimating an EQ-5D-5L value set for China. Value in health: The journal of the International Society for Pharmacoeconomics and Outcomes Research 20: 662-669.
- Gareen IF, Duan F, Greco EM, Snyder BS, Boiselle PM, et al. (2014) Impact of lung cancer screening results on participant health-related quality of life and state anxiety in the National Lung Screening Trial. Cancer 120: 3401-3419.
- Freiman MR, Clark JA, Slatore CG, Gould MK, Woloshin S, et al. (2016) Patients' knowledge, beliefs, and distress associated with detection and evaluation of incidental pulmonary nodules for cancer: Results from a multicenter survey. Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer 11: 700-708.
- Wiener RS, Gould MK, Woloshin S, Schwartz LM, Clark JA (2013) What do you mean, a spot?: A qualitative analysis of patients' reactions to discussions with their physicians about pulmonary nodules. Chest 143: 672-677.
- Slatore CG, Golden SE, Ganzini L, Wiener RS, Au DH (2015) Distress and patient-centered communication among veterans with incidental (not screen-detected) pulmonary nodules. A cohort study. Annals of the American Thoracic Society 12: 184-192.
- Slatore CG, Press N, Au DH, Curtis JR, Wiener RS, et al. (2013) What the heck is a "nodule"? A qualitative study of veterans with pulmonary nodules. Annals of the American Thoracic Society. 2013 10: 330-335.
- Hudon C, Fortin M, Haggerty JL, Lambert M, Poitras ME (2011) Measuring patients' perceptions of patient-centered care: A systematic review of tools for family medicine. Annals of family medicine 9: 155-164.
- Sullivan DR, Golden SE, Ganzini L, Hansen L, Slatore CG (2015) I still don't know diddly': A longitudinal qualitative study of patients' knowledge and distress while undergoing evaluation of incidental pulmonary nodules. NPJ primary care respiratory medicine 16: 15028.
- Brooks R (1996) EuroQol: The current state of play. Health policy 37: 53-72.
- Koide R, Kikuchi A, Miyajima M, Mishina T, Takahashi Y,(2019) Quality assessment using EQ-5D-5L after lung surgery for non-small cell lung cancer (NSCLC) patients. General thoracic and cardiovascular surgery 67: 1056-1061.
- Szentes BL, Schwarzkopf L, Kirsch F, Schramm A, Leidl R (2019) Measuring quality of life in COPD patients: Comparing disease-specific supplements to the EQ-5D-5L. Expert review of pharmacoeconomics & outcomes research 12: 1-7.
Citation: Lou Y, Fan B, Zhang L, Wu B, Fu Y, et al. (2021) Effects of Pulmonary Nodules on Patient Anxiety and Health-Related Quality of Life. J Pulm Med Respir Res 7: 063.
Copyright: © 2021 Yueyan Lou, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.