Electromyographic Determination of Jump Landing Sequence and Pre-activation Times During One-foot Landing
*Corresponding Author(s):
Willig GabrielLaboratorio De Investigaciones Biomecanicas, Cátedra De Anatomía Funcional Y Biomecánica, Universidad De Buenos Aires, Buenos Aires 1107, Argentina
Email:gwillig@fmed.uba.ar
Abstract
Introduction: Monopodal jumping is a common gesture in daily life and sports. In the Landing Phase (LF), potential energy is absorbed from the tridimensional stability of the Lower Limb (LH). This stability depends on neuromuscular strategies that include factors such as Muscle Preactivation Times (MAT) and the Sequence of Participation (SP) of the muscle groups. The alteration of TPA has been pointed out as a factor of possible injury. The aim of this study was to determine the preactivation times and participation sequence of the gluteus medius, adductor magnus, rectus femoris, vastus medialis quadriceps, biceps femoris longus, semimembranosus and soleus muscles during the monopodal jump landing in university students. At the same time, we sought to determine the existence or not of significant differences between men and women.
Materials and methods: Twenty-six young adults, 16 women and 10 men, participated. An inertial sensor and 7 surface electrodes were used to collect electromyographic data in the gluteus medius, rectus femoris and vastus medialis quadriceps, semimembranosus, biceps femoris long head, soleus and adductor magnus muscles.
Results: The general activation sequence was Vastus medialis -Biceps femoris longus - Adductor magnus - Gluteus medius - Rectus femoris -Semimembranosus and soleus. The data obtained reflects the activation prior to ground contact of all the muscles studied. There were differences between genders. Women presented a previous activation in all muscles with the exception of the gluteus medius. The muscles with the greatest variability were the adductor magnus in men and the rectus femoris in women.
Conclusion: The significant differences found between men and women show that there are trends that can be the beginning to better understand the risk factors for injury generation. The TPA data presented a great variability which could reflect the existence of different activation patterns and not a unique behavior of the MMII musculature.
Introduction
Jumping is a common gesture in many activities of the daily living and sports. It can be performed using both lower limbs symmetrically or monopodally. In the last case, they have reported a predominance of the use of the dominant lower limb over the contralateral one. Due to the high incidence of lower limb injuries during the Landing Phase (LF) of the gesture, many researchers have studied its biomechanical characteristics [1]. The knowledge of such research and the potential in preventing injuries through biomechanical modification can collaborate in rehabilitation planning, which makes it fundamental to study and understand jumping for its application in daily clinical practice [2].
For analysis, the jump is divided into two phases, a power generation phase and a landing or damping (FA) phase. FA is characterized by the absorption of the kinetic energy generated by jumping in pursuit of adequate three-dimensional stability of the Lower Limb (LH) [1].
Achieving functional stability involves a complementary relationship between the static-passive and dynamic-active components of the sensorimotor system. Dynamic contributions bring into play neuromuscular strategies arising from anticipatory control and neuromotor feedback of the muscles involved [3,4]. These correspond to two interdependent systems that model the relationship between the body and variations in the environment during AF. Prior to ground contact, a preparatory muscle contraction of the IM takes place and it allows controlling the ground reaction force, stabilizing the joints, controlling joint moments avoiding collapse and preventing injuries [4,5]. After contact, the sensitive afferents report the changes in the system and immediately a reflex response takes place and it allows corrections to be generated. The combined effects of these mechanisms provide effective neuromuscular control of jumping [6,7].
It has been pointed out that the three-dimensional stability of the IM during AF depends on several factors, including muscle pre-activation times and the sequence of participation of the various muscle groups [8]. Previous studies have pointed out the relevance of the hip, knee, and ankle muscles in energy absorption during AF. Highlighting the importance of hip extensors and plantar flexors in sagittal plane as well as the knee and ankle adductors in frontal plane. In the knee, a reflex preparatory co-contraction of the quadriceps and hamstrings takes place, with the pattern and speed of muscle recruitment being important to stabilize that joint [9,10]. Its alteration has been pointed out as a factor of possible injury [7].
Certain aspects of neuromuscular control can be quantified by electromyographic studies [11]. Its application in IM has increased during the last years, allowing it to quantify parameters of clinical interest in jumping [7]. Pre-activation times to ground contact and neuromuscular recruitment during AF of the quadriceps and hamstring muscles have been evaluated using a landing protocol [6,7]. They analyzed neuromuscular differences in jumping between men and women, but the obtained results were contradictory [6,7].
The neuromuscular recruitment patterns and the recruitment TPA of the thigh muscles have been pointed out with an important role in the dynamic stability of the knee [10]. In turn, they have described the pre-activation times of the muscles that cross the knee joint and their sequence of participation [6,7]. The abductor, extensor, and external rotator muscles of the hip together with the tibial stabilizers in the sagittal plane such as the soleus muscle, could be a determining factor in controlling the three-dimensional displacement of the knee [12]. However, it is not clear how they contribute to the stability of this biomechanical unit.
The aim of this study was to determine the pre-activation times and participation sequence of the gluteus medius, adductor magnus, rectus femoris, vastus medialis quadriceps, biceps femoris longus, semimembranosus and soleus muscles during monopodal jump landing in university students. At the same time, we sought to determine the existence or not of significant differences between men and women.
Materials And Methods
Participants
Kinesiology and Physiatry Bachelor’s Degree students from Facultad de Medicina at the University of Buenos Aires who participated in the study from June to August in 2018. Subjects had to be over 18 years old and had to read and sign an informed consent.
There were students excluded from the test due to having manifested pain in the lower limbs and/or lumbar spine at the time of the test, those who had a history of lower limb and/or lumbar spine surgeries, those with lower limbs and lumbar spine injuries in the last 6 months and those with orthopedic alterations in the lower limbs and/or lumbar spine that could interfere with the tests.
The participants who presented errors in the execution of the protocol were eliminated. Tests that did not duly comply with the protocol, such as falling before the time indicated by the evaluator or falling with both feet, were considered failed tests.
The jumps that did not duly comply with the protocol were considered failed and discarded. The most frequent errors consisted on not maintaining the starting position for 10 seconds, falling before the evaluator’s indication and losing balance on landing with both feet.
The participants ranged in age from 22 to 33 years, with a mean age of 25 ± 3.4 years. Regarding their anthropometric properties, they recorded an average of 1.7 ± 0.1m in height, 65.6 ± 12.6 kg in weight and a body mass index of 23.2 ± 2.9. Out of the total, 16 were females 25 ± 3.4 years old, 1.70 ± 0.1m in height, with an average weight of 62.6 ± 9.8 kg and body mass index of 22.5 ± 2.6, while 10 were males 25 ± 3.4 years old, 1.70 ± 0.1m in height, a weight of 70 ± 15.2 kg, and body mass index of 24.1 ± 3.3 on average. Out of the total number of students evaluated, two were eliminated due to errors in the execution of the jump. The final sample size was 26 right-footed participants.
Instrumentation
Electromyographic data were collected by wireless sensors of the Freemg 1000 surface EMG system (BTS Bioengineering S.p.A., Milan, Italy) at a frequency of 1000hz. The placement of self-adhesive bipolar dual surface electrodes followed the standards and indications proposed by SENIAM [13] for the gluteus medius, rectus femoris and vastus medialis quadriceps, semimembranosus, biceps femoris long head and soleus muscles. In the absence of specific recommendations on electrode placement in Adductor magnus the guidelines used in previous studies have been followed [14].
To determine the ground contact event, an inertial sensor (SI) G- Sensor 2 (BTS Bioinngenering, Milan, Italy) including a triaxial accelerometer (16 bits / axes, up to 1000 Hz) with multiple sensitivity (± 2, ± 4, ± 8, ± 16 g), a 13-bit triaxial magnetometer (± 1200 µT, up to 100 Hz), and a triaxial gyroscope (16 bits / axes, up to 8000 Hz), with multiple sensitivity (± 250, ± 500, ± 1000, ± 2000 °/s). The sensor was synchronized with the EMG system and located at the level of the base of the fifth lumbar vertebra [6], because it provides a stable and sufficiently vertical location to be able to determine cephalocaudal acceleration with the least interference of movements in the other planes [15].
The software used for data recording, processing and storage, was BTS® EMG analyzer v2.9.40.0. The time for initial muscle activation was set as two standard deviations above [16,17]. It was recorded during the seconds of stabilization of the participant on the platform, in which the electromyographic signal was in a basal state without active contraction. The event contact against the floor was determined as the instant of lowest vertical acceleration recorded by SI [18-20].
Procedure
A test protocol previously described by Devita and Skelly [21] was used to collect landing data. Subjects started from monopodal support in a balanced position near the front edge of a 19 cm high platform with the foot of the limb to be tested fully suspended off the platform and with the heel resting against the front edge of the box for 10 seconds in order to relax the muscles that about were to be tested. To initiate the movement, the subjects performed a forward lean by falling vertically, landing as balanced as possible on the test leg and maintaining that position for 10 seconds (Figure 1). This procedure was explained to the subjects once the surface electrodes were placed, allowing them to practice 3 times the gesture prior to the measurement. They then performed 4 correct landings for recording and analysis [5,7,8,22].
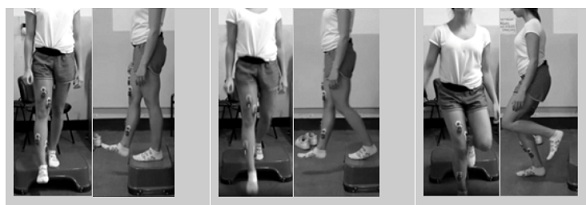 Figure 1: Sequence of instants of the execution of the fall protocol in frontal and sagittal planes.
Figure 1: Sequence of instants of the execution of the fall protocol in frontal and sagittal planes.
Statistical analysis
A descriptive analysis was performed comparing the averages, standard deviations and coefficients of variation of the reactivation time between the different muscles. This was done considering all the subjects evaluated, as well as within the group of women and the group of men. In addition, a t-Student test was performed to verify possible differences in the mean reactivation time of each muscle between women and men, the difference being considered significant if the p-value was less than 0.05 (p<0.05).
Results
Table 1 presents the TPAs, their respective standard deviations and the coefficient of variation. The muscles are ordered according to the pre-contact activation sequence of all participants.
|
Sequence |
Muscles |
P Average |
DS |
Coefficient of variation (%) |
|
1 |
Vastus Medialis quadriceps |
303,5 |
145.9 |
48.1 |
|
2 |
biceps femoris longus |
250.3 |
98.5 |
39.4 |
|
3 |
Adductor Magnus |
247.8 |
106 |
42.8 |
|
4 |
Gluteus Medius |
247.7 |
72.8 |
29.4 |
|
5 |
Rectus Femoris |
237.3 |
161.3 |
68 |
|
6 |
Semimembranosus |
219.3 |
90.7 |
41.3 |
|
7 |
Soleus |
186 |
54 |
29.1 |
Table 1: Preactivation time and Sequence
Table 2 and Table 3 present the APRs, their respective standard deviations and the coefficient of variation for the female and male groups, respectively.
|
Sequence |
Muscles |
Average |
DS |
Coefficient of variation (%) |
|
1 |
Vastus Medialis quadriceps |
344.67 |
155.6 |
45.1 |
|
2 |
Rectus Femoris |
290.5 |
183.2 |
63 |
|
3 |
Biceps Femoris longus |
268.25 |
103 |
38.4 |
|
4 |
Adductor Magnus |
265.17 |
97.7 |
36.8 |
|
5 |
Semimembranosus |
247.69 |
91.7 |
37 |
|
6 |
Gluteus Medius |
238.34 |
79.8 |
29.3 |
|
7 |
Soleus |
172.97 |
52 |
30.1 |
Table 2: Pre-activation time and Sequence – Female.
|
Sequence |
Muscles |
Average |
DS |
Coefficient of variation (%) |
|
1 |
Gluteus Medius |
262.6 |
78.7 |
30 |
|
2 |
Vastus Medialis quadriceps |
237.7 |
104.5 |
44 |
|
3 |
Biceps Femoris longus |
221.6 |
88.2 |
39.8 |
|
4 |
Adductor Magnus |
220.1 |
117.9 |
54.6 |
|
5 |
Soleus |
206.9 |
53.1 |
25.7 |
|
6 |
Semimembranosus |
174 |
71.4 |
41.1 |
|
7 |
Rectus Femoris |
152.2 |
57.6 |
37.8 |
Table 3: Pre-activation time and Sequence - Males
Table 4 presents the differences between women and men indicating the P value less than 0.05 and the activation sequence.
|
Muscles |
p-value |
|
Vastus Medialis quadriceps |
0.03 |
|
Biceps Femoris longus |
0.12 |
|
Adductor Magnus |
0.15 |
|
Gluteus Medius |
0.21 |
|
Rectus Femoris |
0.02 |
|
Semimembranosus |
0.02 |
|
Soleus |
0.06 |
Table 4: p-values for TPA comparison of men vs. women.
Discussion
The main objective of the study was to establish the times and sequence of muscle pre-activation during the landing of the one-legged jump. The data obtained reflects the activation prior to ground contact of all the muscles studied. This coincides with the anticipatory strategies previously described to preserve the body's balance by compensating for the modifications produced by the movement [3,4,23,24]. However, while landing, the pre-activation of the muscles of the IM with diverse kinematic actions would collaborate in the stabilization and absorption of the loads. These findings agree with Baratta et al. where the quadriceps-biceps femoris coactivation collaborates in joint stability, equalizing the distribution of pressures on the articular surfaces and regulating the mechanical impedance preventing overload.
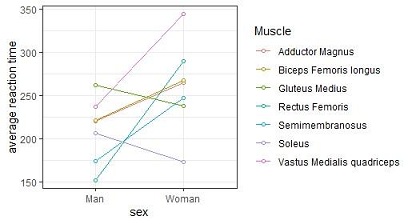 Figure 2: Average reaction time by sex.
Figure 2: Average reaction time by sex.
The general sequence of activation exhibited by the participants was Vastus medialis -Biceps femoris longus - Adductor magnus - Gluteus medius - Rectus femoris -Semimembranosus and soleus (Figure 2). This pattern reflects the activation in the first instance of the knee monoarticular extensor, followed by the hip extensor muscles and finally the ankle extensor. This can be related to the kinematic description made by Heebner 2017, where in monopodal jump damping the main variation of joint angles takes place in the knee [2].
The soleus presented delayed activation regarding the other muscles analyzed. In contrast, the muscles proximal to the soleus are the first to activate, highlighting the coactivation of the gluteus medius and adductor muscles, antagonists in the frontal plane, to decrease excursion in that plane and in turn to participate in hip extension.
The TPA data presented a wide range, being greater in the rectus femoris, vastus medialis, adductor, semimembranosus and biceps femoris muscles. This behavior coincides with previous research [6,7]. This could reflect the existence of different activation patterns, and not a unique behavior of the MMII musculature.
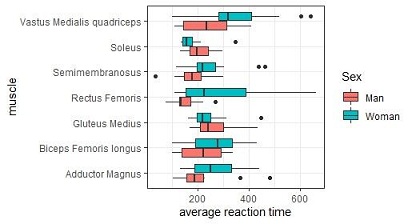 Figure 3: Average reaction time per muscle by sex.
Figure 3: Average reaction time per muscle by sex.
Differences between men and women in terms of activation, muscle recruitment and joint stability of the knee have been reported in previous research [1,25,26]. Regarding those found in the present study, it is worth mentioning the differences in the activation sequence where the main discrepancy was recorded between the rectus femoris and gluteus medius muscles (Figure 3). The latter was the sixth to activate in women and the first in men. Meanwhile, the rectus femoris ranked second in women and last in men. The difference in the activation sequence between genders of the gluteus medius is not due to a variation of the TPA values (p: 0.21) but an anticipation of the other muscles in women. This discrepancy could be explained by the difference in rectus femoris TPA (p=0.02) not observed in gluteus medius (p:0.21). Women presented earlier activation in all the muscles studied except for the gluteus medius, which leaves this muscle in a delayed position relative to men (Figure 4). Significant differences were reflected in the muscles: rectus femoris (p=0.02), vastus medialis (p=0.03) and semimembranosus (p=0.02) between genders. Regarding TPA variability according to gender, the muscles with the greatest variability were the adductor magnus (CV: 53.6) in men and the rectus femoris (CV: 63) in women.
In women, a described aspect of the damping phase of the monopodal jump is the appearance of the so-called dynamic valgus [1,6,27], a compensatory movement of knee abduction, in which hip adduction has been pointed out as the main responsible for the increase of this action [11]. Documenting an increase of the same move in women during activities involving single-legged cutting and jumping [6,26-28]. However, the observed pre-activation times of the primary hip abductor, the gluteus medius, were similar when comparing males and females, suggesting the influence of other factors on kinematics between the two genders or the relative delayed pre-activation mentioned above.
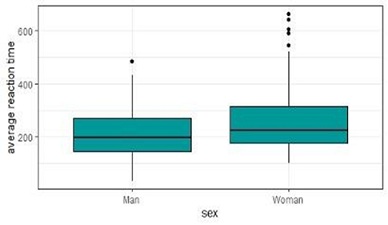 Figure 4: Average reaction time by sex.
Figure 4: Average reaction time by sex.
Regarding the TPA of the vastus medialis and rectus femoris show a significant early action (p=0.03; p=0.02) of women in relation to men, this is in an agreement with Medina in 2008. Such early pre-activation may be related to the higher Anterior Cruciate Ligament (ACL) injury risk rate present in women [1,6] due to a lower knee flexion [1,26] and an anterior displacement of the tibia which would increase ACL tension during the landing phase [29], which would increase the risk of injury. Marked early activation of the vastus medialis in females may also be related to femoropateal syndrome [30]. However, Marotta found late activation of the vastus medialis in female athletes, implying the possible influence of the level of physical activity on the electromyographic behavior of the MI, showing that the assessment of muscle activity using pre-activation times are an important tool to quantify the neuromuscular status of individuals and generate prevention plans.
Conclusion
As we have observed in our results, the pre-activation times and the sequence produced by the muscles in the landing of a one-legged jump are important data to take into account in terms of the functional assessment of individuals. The significant differences found between men and women show that there are certain trends that may be the beginning for a better understanding of the biomechanical risk factors in injury generation.
However, the great variability of the data obtained in the present study, and in previous studies using the same jumping protocol does not allow us to reach further conclusions. Possibly related to the small sample size analyzed, being necessary to deepen in this sense.
The TPA data presented a great variability which could reflect the existence of different activation patterns and not a unique behavior of the musculature of the MMII. Therefore, the search for a universal activation pattern would be questionable and future research should be carried out in this regard.
Limitations
The sample size, which was accessed through the participation of volunteers is a factor that increases the variability of the results; therefore, we suggest enlarging the sample in order to reduce this random error.
References
- Powers CM (2010) The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J Orthop Sports Phys Ther 40: 42-51.
- Heebner NR, Rafferty DM, Wohleber MF, Simonson AJ, Lovalekar M, et al. (2017) Landing kinematics and kinetics at the knee during different landing tasks. J Athl Train 52: 1101-1108.
- Jacobs JV, Horak FB (2007) Cortical control of postural responses. Journal of Neural Transmission, 114: 1339-1348.
- Lephart SM, Ferris CM, Riemann BL, Myers JB, Fu FH (2002) Gender Differences in Strength and Lower Extremity Kinematics During Landing. Clin Orthop Relat Res 401: 162-169.
- Horita T, Komi PV, Nicol C, Kyröläinen H (2002) Interaction between pre-landing activities and stiffness regulation of the knee joint musculoskeletal system in the drop jump: Implications to performance. European J Appl Physiol 88: 76-84.
- Marotta N, Demeco A, de Scorpio G, Indino A, Iona T, et al. (2020). Late activation of the vastus medialis in determining the risk of anterior cruciate ligament injury in soccer players. J Sport Rehabil 29: 952-955.
- Medina JM, Valovich McLeod TC, Howell SK, Kingma JJ (2008) Timing of neuromuscular activation of the quadriceps and hamstrings prior to landing in high school male athletes, female athletes, and female non-athletes. J Electromyogr Kinesiol 18: 591-597.
- Huston LJ, Wojtys EM. Neuromuscular Performance Characteristics in Elite Female Athletes. Am J Sports Med 24: 427-436.
- Baratta R, Solomonow M, Zhou BH, Letson D, Chuinard R (1988). Muscular coactivation. The role of the antagonist musculature in maintaining knee stability. Am J Sports Med 16: 113-122.
- Solomonow M, Baratta R, Zhou BH, Shoji H, D’ambrosia RD (1987) The EMG-Force Model of Electrically Stimulated Muscle: Dependence on Control Strategy and Predominant Fiber Composition. IEEE Trans Biomed Eng 34: 692-703.
- Hollman JH, Ginos BE, Kozuchowski J, Vaughn AS, Krause DA, et al. (2009) Relationships Between Knee Valgus, Hip-Muscle Strength, and Hip-Muscle Recruitment During a Single-Limb Step-Down. J Sport Rehabil 18: 104-117.
- Padua DA, Beii DR, Clark MA (2012) of-athletic-training Neuromuscular Characteristics of Individuals Displaying Excessive Medial Knee Displacement. J Athl Train 47: 525-536.
- Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10: 361-374.
- Lovell GA, Blanch PD, Barnes CJ (2012) EMG of the hip adductor muscles in six clinical examination tests. Phys Ther Sport 13: 134-140.
- B?azkiewicz M, Wiszomirska I, Wit A (2014) Comparison of four methods of calculating the symmetry of spatial-temporal parameters of gait. Acta Bioeng Biomech 16: 29-35.
- Shultz SJ, Perrin DH, Adams JM, Arnold BL, Gansneder BM, Granata KP (2000) Assessment of neuromuscular response characteristics at the knee following a functional perturbation. J Electromyogr Kinesiol 10: 159-170.
- Shultz SJ, Perrin DH, Milton J, Brent A, Arnold L, et al. (2001) Neuromuscular Response Characteristics inMen and Women After Knee Perturbation ina Single-Leg, Weight-Bearing Stance. J Athl Train 36: 37-43.
- Bugané F, Benedetti MG, Casadio G, Attala S, Biagi F, et al. (2012) Estimation of spatial-temporal gait parameters in level walking based on a single accelerometer: Validation on normal subjects by standard gait analysis. Comput Methods Programs Biomed 108: 129-137.
- Cimolin V, Capodaglio P, Cau N, Galli M, Santovito C, et al. (2017) Computation of spatio-temporal parameters in level walking using a single inertial system in lean and obese adolescents. Biomed Tech 62: 505-511.
- Zago M, Sforza C, Pacifici I, Cimolin V, Camerota F, et al. (2018) Gait evaluation using inertial measurement units in subjects with Parkinson’s disease. J Electromyogr Kinesiol 42: 44-48.
- Devita P, Skelly WA (1992) Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med Sci Sports Exerc 24: 108-115.
- Huston LJ, Lou M, Greenfield VH, Wojtys EM (2000) Anterior Cruciate Ligament Injuries in the Female Athlete Potential Risk Factors. Clin Orthop Relat Res 372: 50-63.
- le Pellec A, Maton B (2000) Anticipatory postural adjustments depend on final equilibrium and task complexity in vertical high jump movements. J Electromyogr Kinesiol 10: 171-178.
- Riemann BL, Lephart SM (2002) The sensorimotor system, part I: the physiologic basis of functional joint stability. J Athl Train 37: 71.
- Barber-Westin SD, Noyes FR, Smith ST, Campbell TM (2009) Reducing the risk of noncontact anterior cruciate ligament injuries in the female athlete. Phys Sportsmed 37: 49-61.
- Sigward SM, Pollard CD, Powers CM (2012) The influence of sex and maturation on landing biomechanics: Implications for anterior cruciate ligament injury. Scand J Med Sci Sports 22: 502-509.
- Ford KR, Myer GD, Hewett TE (2003) Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc 35: 1745-1750.
- Malinzak RA, Colby SM, Kirkendall DT, Yu B, Garrett WE (2001) A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech (Bristol, Avon) 16: 438-445.
- Colby S, Francisco A, Yu B, Kirkendall D, Finch M, et al. (2000) Electromyographic and Kinematic Analysis of Cutting Maneuvers Implications for Anterior Cruciate Ligament Injury. Am J Sports Med 28: 234-240.
- Greuel H, Herrington L, Liu A, Jones RK (2019) How does acute pain influence biomechanics and quadriceps function in individuals with patellofemoral pain? Knee 26: 330-338.
Citation: Gabriel W, Lucila DV, Manuel CJ, Franco T (2021) Electromyographic Determination of Jump Landing Sequence and Pre-activation Times During One-foot Landing. J Orthop Res Physiother 7: 057
Copyright: © 2021 Willig Gabriel, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.