Maxillary Split Crest and Sinus Augmentation with Piezosurgery and Growth Factors
*Corresponding Author(s):
Maurizio SerafiniSchool Of Medicine, University Of “Aldo Moro” Bari-Italy, Via Caduti Sul Lavoro, 37, 66100 CHIETI, Abruzzo, Italy
Email:serafinidrmaurizio@gmail.com
Abstract
One of the most common anatomic limitation which prevents a correct implant placement, is horizontal and vertical bone deficiency. Modern surgical techniques allow predictable rehabilitation of these severe defects, using on one side the great regenerative potential of autologous growth factors, on the other side instruments that allow more bone preservation and less trauma on hard and soft tissues, crucial criteria for successful surgeries. This case report shows the rehabilitation of a sever bone defect trough split crest and sinus augmentation with the use of growth factors and Bio-Oss.
Keywords
Growth factors; Implantology; Maxillary split crest; Piezoelectric device; Sinus augmentation
INTRODUCTION
Bone width and height deficiency can occur as a result of many inflammatory and traumatic conditions, such as chronic periodontal disease, systemic disease that compromise the tooth-supporting structures, prolonged denture wear with subsequent disuse atrophy, post extraction defects with hypernpeumatized sinus, implant removal caused by periimplantitis with severe bone resorption, trauma, misalignment, etc. Different are the surgical approaches for an implant rehabilitation in these areas [1,2]
- • Split crest
- • Autologous bone grafts harvested from the iliac crest, calvarial or tibial bone which are hospital based procedures, or intraoral bone graft which is an easier autologous graft technique but with limited bone volume available
- • Heterologous bone graft or bioglass with resorbable or not resorbable membrane
- • Titanium mesh
Split crest and implant insertion in one stage surgery using growth factors in combination with bone graft is a predictable technique, with faster healing process thanks to growth factors great potential for soft and hard tissue regeneration [3,4].
Bone graft alone, allows immediate or long term reabsorption with unpredictable final bone volume, specially using iliac or tibial bone grafts because embryologically different from the cranium, for this reason a second surgery with animal derived bone graft it’s often required.
MATERIALS AND METHODS
Type C bone defect (Misch and Judy classification) [5], with width between 1.5 and 2.5 mm and height between 8 and 12 mm (Figure 1). The split crest procedure should be performed only with really thin chisels because the use of burs would compromise bone preservation.
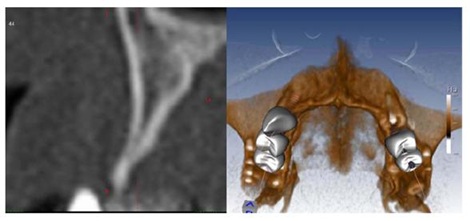 Figure 1: Type C bone defect
Figure 1: Type C bone defect
Expansion technique
Ridge expansion technique was firstly described by Tatum [6] and then modified by other Authors. After a mucoperiosteal flap is reflected to expose the crest of the bone, a crestal incision separating the buccal from the palatal bone is connected to the two beveled vertical relaxing incisions on the buccal bone plate, allowing the horizontal distraction of the vestibular cortical plate. With the help of thin chisels, tapered osteotomes with increasing diameters are used to separate the two cortices to expand the ridge and widen the crestal apical diameter. After achieving the proper width of the bone (Figure 2), the implant site preparation is performed (Figure 3).
Nowadays technology helps the clinician and the patient with a less traumatic and more predictable surgery, performed with piezosurgery device. Its advantages are
- • Better compliance for both the clinician and the patient
- • Less risk of ridge fracture
- • Faster surgery and healing time
- • Less morbidity during or after surgery
CASE REPORT
58 years old female patient, in treatment for one year with strontium ranelate, calcium and vitamin D for osteoporosis and negative blood tests.
First level orthopantomography shows a bone defect on 1.6 extending to the maxillary sinus (Figure 2).
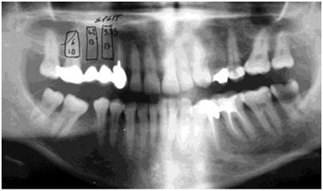 Figure 2: Preliminary Study on orthopantomography
Figure 2: Preliminary Study on orthopantomography
In substitution of the old prosthetic bridge extending from 1.3 to 1.6, the plan is to replace 1.6-1.5-1.4 with dental implants after a crestal sinus lift on 1.6 region.
Second level Computed Tomography (CT) scan confirmed the severe bone defect which in region 1.4-1.5 measures 3.7 mm on the mid-apical part and 1.54 mm on the coronal segment of the ridge (Figures 3,4,5). After these measurements, it’s decided to perform a split crest in this area.
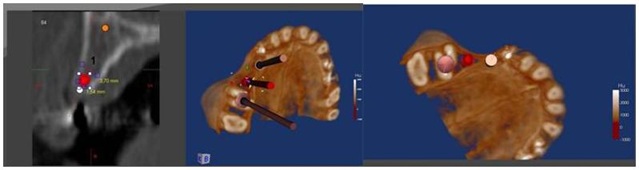 Figures 3,4,5: Planning Second level Computed Tomography (CT).
Figures 3,4,5: Planning Second level Computed Tomography (CT).
During surgery, 4 tubes of blood are harvested and centrifuged at 1000 rpm for 20 min, obtaining 4 ml of PRP by each one (Figure 6).
 Figure 6: Blood Venus and PRP
Figure 6: Blood Venus and PRP
After extraction of 1.6, a full thickness flap is raised; a horizontal incision to separate the vestibular from the palatal cortical is made with piezosurgery connected with two vertical incisions on the vestibular cortical (Figures 7,8).
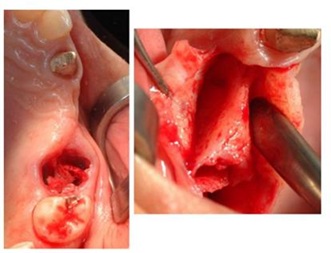 Figure 7: Extraction and a full thickness flap.
Figure 7: Extraction and a full thickness flap.
 Figure 8: Piezosurgery incision.
Figure 8: Piezosurgery incision.
The ridge expansion is performed with increasing diameter osteotomes to achieve the proper width of bone for the insertion of two implants with 3.75 mm and 4.2 mm diameters and 13 mm length. A crestal sinus lift is performed on 1.6 region with Summers osteotomes and an implant 6 x 10 mm is inserted (Figure 9).
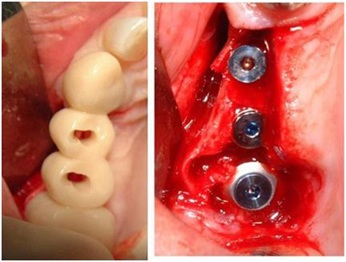 Figure 9: Test provisional prosthesis in mouth, with landmark holes to make the guide holes on the bone. Fig. 9bis Implants allocated.
Figure 9: Test provisional prosthesis in mouth, with landmark holes to make the guide holes on the bone. Fig. 9bis Implants allocated.
Implants insertion followed the injection of liquid PRP and imbibed fibrin sponges; the residual gaps between the corticals and in the interproximal spaces between corticals and implants, are filled with a packing of PRP activated with calcium chloride that allows platelet degranulation in order to obtain PRF which is mixed with Bio-Oss (Figure 10).
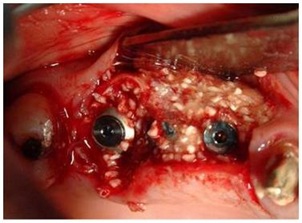 Figure 10: Packing of PRP activated with calcium chloride and Bio-Oss
Figure 10: Packing of PRP activated with calcium chloride and Bio-Oss
Post-op orthopantomography is shown in figure 11.
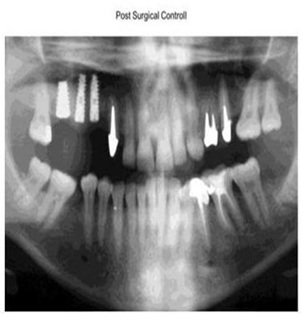 Figure 11: Post surgical Control
Figure 11: Post surgical Control
4 months post op orthopantomography shows healing of the split crest and the sinus lift (Figure 12), as well as the 5years radiographic check up (Figure 13).
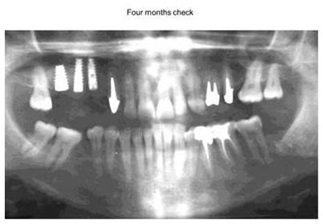 Figure12: X-ray Control Four Months later.
Figure12: X-ray Control Four Months later.
 Figure13: 5 years radiographic check up.
Figure13: 5 years radiographic check up.
DISCUSSION
Nowadays is possible and advisable to combine advantages of advanced technology with the great healing potential of growth factors to achieve a successful rehabilitation of severe bone defects. An accurate preop plan is necessary to manage and anticipate all the surgical steps. Piezoelectric devices, thanks to the use of modulated frequency piezoelectric energy scalpels, permits the expansion of the ridge and implants placement in advanced and complex situations previously treated in 2 surgical stages. The use of growth factors boosts the regeneration and allows reduction of the morbidities and time needed for dental rehabilitation [7]. The principal limitation of this technique is related to the skills and experience of the operator.
REFERENCES
- Fiorellini JP, Nevins ML (2003) Localized ridge augmentation/preservation. A systematic review. Ann Periodontol 8: 321-327.
- McAllister BS, Haghighat K (2007) Bone augmentation techniques. J Periodontol 78: 377-396.
- Sethi A, Kaus T (2000) Maxillary ridge expansion with simultaneous implant placement: 5-year results of an ongoing clinical study. Int J Oral Maxillofacial Implants 15: 491-499.
- Oyama T, Nischimoto S, Tsugawa T, Shimizu F (2004) Efficacy of platelet-rich plasma in alveolar bone grafting. Int J Oral Maxillofac Surg 62: 555-558.
- Misch CE, Judy KW (1987) Classification of partially edentulous arches for implant dentistry. Int J Oral Implantol 4: 7-13.
- Tatum H (1986) Maxillary and sinus implant reconstruction. Dent Clin North Am 30: 207-229.
- Marx RE, Carg AK (2005) Dental and craniofacial applications of platelet-rich plasma. Quintessence books (Pg No: 168), Chicago, USA.
Citation: Inchingolo F, Dipalma G, Contaldo M, Serpico R, Domenico MD (2020) Maxillary Split Crest and Sinus Augmentation with Piezosurgery and Growth Factors. J Stem Cell Res Dev Ther 6: 058.
Copyright: © 2020 Francesco Inchingolo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.