Mortality Due to Failure to Quarantine during the Covid-19 Pandemic
*Corresponding Author(s):
Klena JWSentara Heart Hospital, Gresham Drive, Norfolk, Virginia, United States
Tel:+1 7573886005,
Email:jwklena@yahoo.com / jwklena@sentara.com
Abstract
The Covid-19 Pandemic has created significant chaos in the United States’ health care system. The virus has potentially lethal respiratory consequences making pulmonary surgery particularly precarious. Presented is a case of a patient who underwent elective resection of a lung carcinoma who, despite concordance with institutional and Centers for Disease Control and Prevention (CDC) guidelines for the pre-operative testing for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), contracted the virus unknowingly prior to his procedure. He underwent an uncomplicated resection and hospitalization only to present after discharge testing positive for Covid-19 ultimately leading to his death. He appears to have contracted the virus after his pre-operative testing by not remaining quarantined prior to his surgery.
Keywords
Covid-19; Lung cancer; Robotic lung surgery
INTRODUCTION
The presence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) causing the Covid-19 pandemic can be tested for pre-operatively. A negative test reflects the status of the individual during a point in time. Patient isolation through quarantine after a negative test is important to limit exposure to the virus in the peri-operative setting. We present a case where failure of a patient to sequester following a negative test led to their unnecessary death profoundly illustrating the importance of quarantine.
A 72-year-old man was initially seen as an outpatient for a growing right lower lobe lung nodule. Prior to his initial visit he has undergone an image guided biopsy of the nodule which was suggestive of an epithelioid carcinoma. Ironically the patient wished to defer resection from his initial visit in March 2020 when the Covid-19 pandemic was beginning in the United States until he felt more comfortable with being hospitalized. He represented in June 2020 wishing to undergo resection. Repeat computed tomography of the chest at that time (Figure 1) revealed growth of the nodule but no evidence of metastatic disease and he was scheduled for surgery.
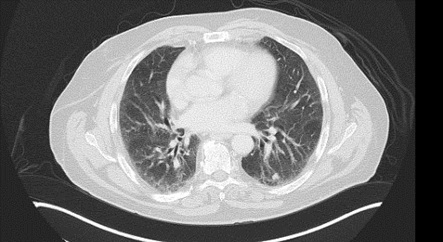 Figure 1: Computed tomography study of the chest showing right lower lobe nodule prior to resection.
Figure 1: Computed tomography study of the chest showing right lower lobe nodule prior to resection.
Per our institution’s guidelines for elective surgery he underwent pre-operative Covid-19 testing with a SARS-CoV-2 Test which is a qualitative PCR-based FDA approved assay for the detection and identification of SARS-CoV-2 nucleic acid. The test was performed 72 hours prior to his scheduled operation. He underwent screening as well and denied recent fever, cough, fatigue and myalgia as well as contact with anyone known to have Covid-19. The day prior to his surgery the patient went to lunch with his minister who 3 days later tested positive for Covid-19 after developing a fever. The patient underwent a robotic-assisted sublobar resection of his right lower lobe nodule with hilar and mediastinal node sampling without complication. Pathology from his resection revealed a 1.3 cm clear cell carcinoma1 of the lung which was staged as a TIb N0 M0, Stage IA2 lung carcinoma. With margins greater than 2 cm it was felt to be an adequate resection and definitive treatment for his malignancy.
The patient made an uncomplicated recovery and was discharged on post-operative day 3. The following day the patient called the thoracic surgery service and reported he had a fever of 99.9oF and had a new dry cough not present until that day. Three days later he presented to the emergency department and was found to have a fever of 38.1oC. A CT scan of the chest revealed multiple new areas of faint ground glass opacities in each lung (Figure 2). Although he was found to have a urinary tract infection with gram negative rods he was also retested for Covid-19 which revealed him to have the virus. A second test was also positive. The patient was admitted and did well for several days prior to experiencing abrupt respiratory insufficiency one week into his hospitalization requiring intubation. He developed adult respiratory distress syndrome and then precipitously went into multiple organ dysfunction syndrome resulting in death on hospital day 15.
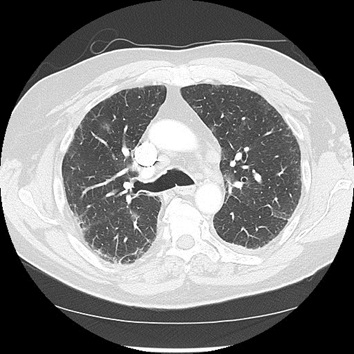
Figure 2: Computed tomography study of the chest, post resection, showing new ground glass opacities in the bilateral lungs.
COMMENT
Per the CDC, the Covid-19 pandemic has resulted in 5,715, 567 cases and 176,617 deaths in the United States at this time [1,2]. The SARS-CoV-2 virus results in a respiratory illness that may cause a paucity of symptoms or a fulminant illness with multi-system organ failure and death [3]. Because the virus has a predilection for the lungs patients undergoing pulmonary surgery are especially susceptible to higher mortality rates when undergoing resection when infected with the virus with an early report from China noting a 27.3% mortality for thoracic surgical patients undergoing surgery compared to a 2% historical mortality rate [4]. In addition to increased patient mortality from historically low risk procedures a patient with Covid-19 also places health care providers at increased risk for contracting the virus. Thoracic procedures allowing multiple exposures to aerosolized patient body fluids are particularly hazardous to health care providers prompting recommendations for increased precautions to reduce the risk [5]. The pandemic has forced health care entities to reconsider multiple facets of health care delivery including the allocation of resources and the ethical treatment of patients [6].
With respect to the case presented, the patient was Covid-19 negative 3 days prior to his surgery by PCR testing. He was instructed to remain quarantined and limit his personal contacts until his surgery. His indiscretion in breaking quarantine led to exposure to the SARS-CoV-2 virus, contraction of the virus and ultimately his death after a low risk surgery. The patient’s incubation period of 6 days correlates with published reports of 5.2 days in surgical patients [7]. He was asymptomatic with respect to the virus at the time of his admission and hospital stay only becoming symptomatic after discharge. Because his pre-operative Covid-19 status was negative the patient did not receive an upgraded exposure status during his hospitalization potentially exposing all health care workers encountered during his hospitalization and placing everyone in the operating room at especially high risk for contraction of the virus.
The case illustrates the point in time nature of Covid-19 testing and the inability to determine the presence of infection on a continuum. The importance of sequestering oneself after testing to avoid exposure is noted. The presented patient demonstrates the inadequacies of the present testing algorithm; only repeated testing could have confirmed the patient’s Covid-19 status immediately prior to surgery. The cost and feasibility of repeated testing in asymptomatic patients makes this untenable. Thus the importance of quarantine is paramount and the lack of adherence can lead to mortality even for low risk procedures. Communication of this fact to patients is a matter of life or death.
MEETING PRESENTATION
None
REFERENCES
- Jeffus SK, Gardner JM, Steliga MA, Shah AA, Stelow EB, et al. (2019) Hyalinizing clear cell carcinoma of the lung: Case report and review of the literature. Am J Clin Pathol 148: 73-80.
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). Centers for Disease Control and Prevention, USA.
- Xu Y, Liu H, Hu K, Wang M (2020) Clinical recommendations on lung cancer management during the COVID-19 pandemic. Thorac Cancer 11: 2067-2074.
- Chen K, Gao S, Liu L, Jianxing H, Jiang G, et al. (2020) Thoracic surgeons’ insights: Improving thoracic surgery outcomes during the coronavirus disease 2019 pandemic. Ann Thorac Surg 110: 349-352.
- Thornton D, Reid D, Shelley B, Steven M (2020) Management of the airway and lung isolation for thoracic surgery during the COVID-19 pandemic: Recommendations for clinical practice endorsed by the association for cardiothoracic anesthesia and critical care and the society for cardiothoracic surgery in great britain and Ireland. Anaesthesia 396: 1-8.
- Drake D, Morrow CD, Kinlaw K, De Bonis M, Zangrillo A, et al. (2020) Cardiothoracic surgeons in pandemics: Ethical considerations. Ann Thorac Surg 110: 355-358.
- Lei S, Jiang F, Su W, Chen C, Chen J, et al. (2020) Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 21: 1-8.
Citation: Klena JW, Ward JR (2020) Mortality Due to Failure to Quarantine during the Covid-19 Pandemic. J Pulm Med Respir Res 6: 048.
Copyright: © 2020 Klena JW, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.