Neurofibrom-Schwannom Hybrid Tumor in the Chest Wall
*Corresponding Author(s):
Cakmak MuharremDepartment Of Thoracic Surgery, Firat University Faculty Of Medicine, Elazig, Turkey
Tel:+90 4242333555 (2130),
Email:drcakmak@gmail.com
Abstract
Schwannoma originates from the roots of spinal nerve. Chest wall shwannoma originating from intercostal nerves is very rare. In this study, we aimed to share a schawannoma-neurofibroma hybrid tumor located in the chest wall.
Keywords
Chest wall; Mass; Neurofibroma; Schwannoma
INTRODUCTION
Schwannoma is a benign, encapsulated, neurogenic tumor originating from schwann cells. They often originate from the roots of the spinal nerve. Neurofibroma is a tumor originating from the nerve sheath anywhere in the body [1]. Although chest wall shwannoma and neurofibromas originating from intercostal nerves have been reported rarely, schwannoma-neurofibroma hybrid tumor has not been reported. Nerve system rooted tumors are seen equally in women and men [2]. They are usually asymptomatic and benign. Malignancy is rarely seen. Symptomatic ones often present as compression-related pain or slow-growing, painless, prominent masses. Neurofibromas are mostly associated with neurofibromatosis. Radiological data are helpful in the diagnosis. Treatment is surgical excision, but long-term follow-up is essential for recurrence [3]. In this study, we aimed to share a schawannoma-neurofibroma hybrid tumor located in the chest wall.
CASE REPORT
A 47-year-old female patient was admitted to our clinic with the complaint of a painful swelling in her chest wall that had gradually increased in the last year. On examination, a painful lesion measuring approximately 50x25mm was detected on the lateral of the left hemithorax.
Contrast-enhanced computed tomography of the chest was requested to see the extent of the lesion on the chest wall. On the thorax CT was seen lesion in size 51x28x25cm in the axial axis at anterolateral 5th intercostal space in extrapulmonary localization. Density of protruding noduler lesion was average 10 HU (Figure 1).
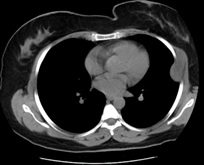 Figure 1: Tomography image of the patient (axial).
Figure 1: Tomography image of the patient (axial).
The patient's medical history was unremarkable, and laboratory tests were normal. The operation was planned. The mass was completely excised (Figure 2). The postoperative chest wall defect was reconstructed using surrounding intact tissues. The pathology result was reported as schawannoma-neurofibroma hybrid tumor (Figures 3(a-d)). No recurrence was observed in the patient who was followed for one year.
 Figure 2: Intraoperative surgical incision and appearance of the mass.
Figure 2: Intraoperative surgical incision and appearance of the mass.
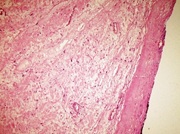 Figure 3a: Presence of right thick capsule seen in Schwannoma (HEX100).
Figure 3a: Presence of right thick capsule seen in Schwannoma (HEX100).
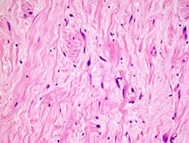 Figure 3b: Neurofibroma areas consisting of spindle-shaped and wavy nucleus cells and collagen (HEX400).
Figure 3b: Neurofibroma areas consisting of spindle-shaped and wavy nucleus cells and collagen (HEX400).
 Figure 3c: S-100 positivity in peripheral nerve sheath tumor (X400).
Figure 3c: S-100 positivity in peripheral nerve sheath tumor (X400).
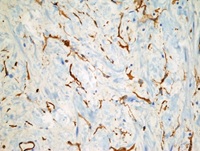 Figure 3d: CD34 positivity in peripheral nerve sheath tumor (X400).
Figure 3d: CD34 positivity in peripheral nerve sheath tumor (X400).
DISCUSSION
Schwannoma is a benign, encapsulated, neurogenic tumor originating from schwann cells [1]. It is a peripheral nerve sheath tumor and often originates from the spinal nerve roots. Neurofibroma is a tumor originating from the nerve sheath anywhere in the body. Although chest wall shwannoma and neurofibromas originating from intercostal nerves have been reported rarely, schwannoma-neurofibroma hybrid tumor has not been reported [2]. Thoracic neurogenic tumors occur in the posterior mediastinum because intrathoracic nerves are mostly concentrated in the paravertebral sulcus region (75-95%). Chest wall shwannoma originating from the intercostal nerves is very rare [2]. It is seen equally among women and men. Neurofibromas are mostly associated with neurofibromatosis. Our patient was a tumor originating from the intercostal nerve.
They are usually asymptomatic, benign and very rarely malignant [3]. It may occur as a solid mass on the chest wall [4]. Symptomatic ones often present as compression-related pain or slow-growing, painless, prominent masses [1]. Schwannomas are divided into four groups as conventional, cellular, plexiform and melanotic schwannomas.
Classical schwannoma is associated with neurofibromatosis type 2. It is also called neurilemmoma and neurinoma. It can be seen at any age, but peaks in the third and sixth decades. It occurs equally in both sexes. central nervous system schwannomas are more common in women [5]. Schwannomas originating from larger nerves are seen especially in cranial sensory nerves and spinal nerve roots. Patients are usually asymptomatic. Cutaneous scwannomas are usually small in diameter. Mediastinal, retroperitoneal and sacral localizations may be large. Therefore, symptoms may occur due to compression of the mass to the surrounding tissue. Schwannomas are usually solitary lesions and grow slowly over the years. Palpable lesions are detected mobile on physical examination. Multiple schwannomas are encountered in two cases. The most common of these is NF2-related bilateral 8th nerve schwannomas. Rarely encountered are multiple schwannomas associated with somatic mutations in the NF2 gene and are called “schwannomatosis [3-5].
These patients do not have a family history and do not have bilateral 8th nerve schwannomas. Instead, most cutaneous or subcutaneous, larger spinal or cranial nerves are involved. Diagnosis is made by the presence of both Antoni A/Antoni B and verocay bodies with histochemical stains. As they are benign and well-limited, total excision is sufficient for treatment. However, when they are incompletely removed, they rarely recur. Malignant transformation is the only type [3-5].
Radiological data are helpful in the diagnosis. Approximately 5% of the spinal origin is seen in the form of an hourglass neural foramen extension. Computed tomography or oblique chest X-rays may show notches in the ribs and enlargement of the vertebrae foramen. In non-contrast CT, paraspinal, well-circumscribed homogeneous hypodense in the posterior mediastinum, areas with fluid density in places, and post-contrast muscle and iso-hyperdense lesions appear. Magnetic resonance imaging shows iso-hypointense on T1-weighted images and homogeneous and heterogeneous apparent hyperintense on T2-weighted images [6]. Treatment is complete surgical excision, but long-term follow-up is required for recurrence. Standard thoracotomy often requires a large incision and causes postoperative pain. Thus, VATS may be preferred to minimize trauma in posterior thoracic cavity located masses [4].
In conclusion, schawannoma-neurofibroma hybrid tumor are not common. Additionally, chest wall placement is very rare. These tumors should be considered in the differential diagnosis of chest wall masses in elderly patients.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
FINANCIAL SUPPORT AND SPONSORSHIP
The authors received no financial support for the research and/or authorship of this article.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- Albert P, Patel J, Badawy K, Weissinger W, Brenner M, et al. (2017) Peripheral nerve schwannoma: A review of varying clinical presentations and ?maging findings. The Journal of Foot and Ankle Surgery 56: 632-637.
- Galukande M, Khingi A (2016) Chest wall schwannoma presenting as a solitary malignant lesion: A case report. Springer Plus 1: 1549.
- Moon H, Park SJ, Kim SR, Park HS, Lee YC (2010) Benign intercostal schwannoma mimicking a solitary metastasis from lung cancer. Thorax 65: 753-754.
- Chen F, Nakayama E, Okubo K, Date H (2008) Intrathoracic multiple schwannomas of a single intercostal nerve. Ann Thorac Surg 86: 660-661.
- Ida CM, Scheithauer BW, Yapicier Ö, Carney JA, Wenger DE, et al. (2011) Primary schwannoma of the bone: A clinicopathologic and radiologic study of 17 cases. Am J Surg Pathol 35: 989-997.
- Kivrak AS, Koc O, Emlik D, Kiresi D, Odev K, et al. (2009) Differential diagnosis of dumbbell lesions associated with spinal neural foraminal widening: Imaging features. Eur J Radiol 71: 29-41.
Citation: Muharrem C, Ferda DA (2020) Neurofibrom-Schwannom Hybrid Tumor in the Chest Wall. J Pulm Med Respir Res 6: 047.
Copyright: © 2020 Cakmak Muharrem, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.