Synchronous Association of a Thymoma with Lung Adenocarcinoma Mixed Subtype: About An Operated Case
*Corresponding Author(s):
Chighaly El Hadj SidiDepartment Of Cardiovascular And Thoracic Surgery, Sahloul University Hospital, Sousse, Tunisia
Tel:+216 58 709 821,
Email:chiccv27@yahoo.fr
Abstract
The synchronous association of different tumors is rare. We report the case of a thymoma in synchronous association with non-small cell lung cancer in a 50-year-old woman who consulted for atypical chest pain. Chest computed tomography showed an anterior mediastinal mass lateralized to the left of the thymic lodge associated with a nodule in upper lobe of right lung. The diagnosis of thymic epithelial tumor with single lung metastasis was more likely and the initial treatment consisted of total thymectomy with resection of all mediastinal fat and a right upper lobe wedge resection taking lung injury by median sternotomy. A thymoma associated with a lung adenocarcinoma was diagnosed and the patient underwent a right superior lobectomy with lymph node dissection via a right posterolateral thoracotomy 4 months later.
Keywords
INTRODUCTION
The synchronous association between different tumors is rare, but usually described for those of the upper aerodigestive tracts whose risk factors are commons. The synchronous association between a thymictumor and a lung adenocarcinoma is very rare [1]. According to our knowledge, only two cases are reported in the literature [2,3].
CASE REPORT
We report the case of a 50-year-old woman with no specific history, who was complaining of atypical chest pain evolving for two months.
The history-taking did not find myasthenic symptoms and the physical examination was normal. The radiological study (Chest computed tomography) has concluded of the existence of an anterior mediastinal mass lateralized to the left, which appears encapsulated and evolves from the thymic lodge, this mass was associated with a nodule in upper lobe of right lung, probably of the same nature (Figure 1) and the bronchial endoscopy was normal.
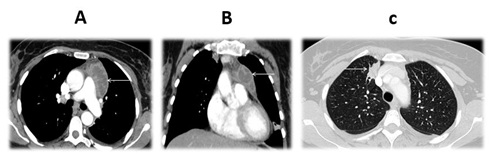 Figure 1: Chest computed tomography. A shows Axial plane showing an anterior mediastinal mass lateralized on the left (arrow), B shows Coronal reconstruction showing an anterior mediastinal mass lateralized on the left (arrow) and C shows Axial plane showing a nodule in upper lobe of right lung (arrow).
Figure 1: Chest computed tomography. A shows Axial plane showing an anterior mediastinal mass lateralized on the left (arrow), B shows Coronal reconstruction showing an anterior mediastinal mass lateralized on the left (arrow) and C shows Axial plane showing a nodule in upper lobe of right lung (arrow).
The eventuality of a thymic carcinoma with a single lung metastasis made more sense. The radiological aspect cystic of the mediastinal mass and intra-parenchymal of the pulmonary nodule contraindicates any percutaneous biopsy, and we opted for a simultaneous complete resection of two lesions, as it seems surgically possible.
The surgery was performed by median sternotomy and consisted of a recess of all mediastinal fat removing the mass with a broad flap of the adjacent pericardium -at the cost of a severance of the left diaphragmatic nerve which was very adherent to the tumor- and a wedge resection on the anterior segment of the upper lobe of the right lung taking the nodule. All the resected material was sent for histopathologic examination.
The postoperative recoveries were unfortunately complicated by left diaphragmatic paralysis (Figure 2) but without clinical manifestation.
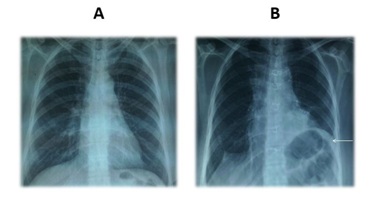 Figure 2: Front chest X-rays. A is Preoperative: normal and B is Postoperative: showing an elevation of the left diaphragmatic dome (arrow).
Figure 2: Front chest X-rays. A is Preoperative: normal and B is Postoperative: showing an elevation of the left diaphragmatic dome (arrow).
Histopathological examination of the operative specimens concluded of a Masaoka stage I type B1 thymoma, and a primitive (as shown by the TTF-1 labelling) lung adenocarcinoma mixed subtype acinar and bronchioloalveolar, stage I. The resection margins were all negatives. The thymic lesion requires only a simple surveillance and the vital prognosis depends on the pulmonary lesion (the pulmonary excision was not carcinologically satisfactory in the absence of lymph node dissection).
A new extension assessment for lung cancer (brain computed tomography, abdominal ultrasound, and bone scan) has been done and negative income, and respiratory functional explorations show a good Forced Expiratory Volume in One Second (FEV1) authorizing reoperation for lobectomy.
We proposed to the patient to undergo an upper right lobectomy with lymph node dissection by posterolateral thoracotomy. The second intervention was performed four months later, since the patient is in good health without any progression of lung tumor disease or recurrence of thymoma for a period of three years.
DISCUSSION
The risk of developing an intra or extra-thoracic second malignancy in patients who have been treated for a thymictumor (thymomectomy with or without preoperative chemotherapy or adjuvant radiotherapy) is currently well-established [2].
The exact mechanisms remain unclear and various theories are proposed. Knowing that this risk cannot be attributed to the effect of the treatment itself or correlated with the histological type or stage of the thymoma as illustrated by the study by Pan et al [3], some authors suggest that this risk can be attributed to a dysfunction in the immune system of the host caused by thymoma [4], while some others suggest that these patients could be genetically predisposed to developing tumors [5].
The metachronous or synchronous association between a thymictumor and a lung cancer is rare. Kamata et al note that its incidence is 5.1% and propose to follow-up by annual Chest computed tomography for patients treated for a thymictumor [6].
In recent years, a few cases of thymictumor associated with operated lung cancer have been reported. Surgical treatment by thymomectomy with lobectomy and lymph node dissection was the rule thoracoscopically [7,8], whereas for Patella et al, the lung cancer was advanced (stage IV) and their patient underwent adjuvant chemotherapy [5].
For us, the choice of a median sternotomy approach was motivated by the site variation of two lesions: mediastinal lesion on the left and pulmonary lesion on the right.
Furthermore, our case presents a diagnostic challenge and consequently therapeutic: the presence of two intrathoracic lesions without being able to verify their histological nature by biopsy. We relied on the radiological features of the lesions, which led us to the diagnosis of a thymic carcinoma with a single right lung metastasis. This false diagnosis had two consequences on our therapeutic decision: the first is the severance of the left diaphragmatic nerve and the second is the realization of an atypical resection on the right lung.
The severance of the left diaphragmatic nerve is the result of ignorance of the benign nature of the mediastinal lesion, it could have consequences on the respiratory function thus complicating the postoperative recoveries and/or against-indicating a satisfactory surgical treatment of the lung lesion. The incomplete surgical treatment of the pulmonary lesion is secondary to the ignorance of its primary nature, which forced us to propose a second operation for the patient with its undesirable consequences (vital risk, multiple incisions, postoperative pain, sanitary cost, etc.). These consequences could be preventable by performing a systematic extemporaneous hisopathological examination.
CONCLUSION
The synchronous association of a thymictumor with a lung cancer is rare but known, the complete surgical treatment of two tumors at the same time is possible and even by minimally invasive approach.
In the absence of a preoperative histopathological diagnosis, the completion of an extemporaneous pathological examination must be necessary.
REFERENCES
- Engels EA, Pfeiffer RM (2003) Malignant thymoma in the United States: demographic patterns in incidence and associations with subsequent malignancies. Int J Cancer 105: 546-551.
- Patella M, Anile M, Vitolo D, Venuta F (2011) Synchronous B3 thymoma and lung bronchoalveolar carcinoma. Interact Cardiovasc Thorac Surg 12: 75-76.
- Dolci G, Dell'Amore A, Asadi N, Caroli G, Greco D, et al. (2015) Synchronous thymoma and lung adenocarcinoma treated with a single mini-invasive approach. Heart Lung Circ 24: 11-13.
- Filossoa, PL, Galassi C, Ruffinia E, Margaritora,S, Bertolaccini L, et al. (2013) Thymoma and the increased risk of developing extrathymic malignancies: a multicentre study. Eur J Cardio thorac Surg 44: 219-224.
- Pan CC, Chen PC, Wang LS, Chi KH, Chiang H (2001) Thymoma is associated with an increased risk of second malignancy. Cancer 92: 2406-2411.
- Welsh JS, Wilkins KB, Green R, Bulkley G, Askin F, et al. (2000) Association between thymoma and second neoplasms. J Am Med Assoc 283: 1142-1143.
- Kamata T, Yoshida S, Wada H, Fujiwara T, Suzuki H, et al. (2017) Extrathymic malignancies associated with thymoma: a forty-year experience at a single institution. Interact Cardiovasc Thorac Surg 24: 576-81.
- Xie D, Xie H, Zhu Y, Jiang G (2014) Simultaneous video-assisted thoracoscopic surgery sleeve lobectomy and thymectomy. Interact Cardiovasc Thorac Surg 19: 313-314.
Citation: El Hadj Sidi C, Alimi F (2019) Synchronous Association of a Thymoma with Lung Adenocarcinoma Mixed Subtype: About An Operated Case. J Pulm Med Respir Res 5: 030.
Copyright: © 2019 Chighaly El Hadj Sidi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.