The Radioactive Iodine (I-131) Efficiency for the Treatment of Well-differentiated Thyroid Cancer
*Corresponding Author(s):
Modallal MohammadDepartment Of Medical Imaging, Faculty Of Allied Medical Health, Palestine Ahliya University, Jabal Daher, PO.Box 1041 Bethlehem, Palestine
Tel:+972598431323,
Email:modallal_1991@hotmail.com
Abstract
Background: The aim of this study was to evaluate the efficacy of radioactive iodine -131 therapy after complete thyroidectomy using high accumulated doses of radioactive iodine (131I ).
Methods: This study was a retrospective review of 141 patients over 22 months at a period between January 2018 and November 2019 in Al Ahli hospital, Hebron, Palestine. All patients after complete thyroidectomy, thyroid remnant tissues were confirmed by I-131 whole-body scan; then, high accumulated Iodine doses were performed for treatment.
Results: The total effective rate of 131I therapy of the current study was 87.9%. The recurrence rate was 12.1%. Of the real 141 thyroid cancer patients, 114 thyroid cancer patients were female (80.15%), and 27 patients were male (19.85%). Recurrences were more common in female patients with thyroid cancer than in male patients (17.55 vs. 11.11%, respectively). However, the middle age 30-40 was the most affected age group, while the least affected age group was the 60-70.
Conclusion: 131I provides an effective treatment for patients with thyroid cancer after a complete thyroidectomy. Thyroglobulin (Tg) levels after surgery is a credible indicator of the presence of remnant thyroid tissue. Whole-body iodine scans are useful in determining remnant thyroid tissue in patients after a complete thyroidectomy.
Keywords
Gamma camera; Radioactive iodine; Thyroid cancer; Thyroid gland; Thyroglobulin; Total thyroidectomy
INTRODUCTION
The thyroid gland is usually found in the lower front of the neck. It consists of two lobes, right and left, connected by a thin bridge called the isthmus. Isthmus covers the anterior trachea at the middle-lower third junction of the gland [1]. The thyroid is anterior to the longus colli and paraspinal musculature and deep to the strap muscles [2]. An accessory lobe, known as the pyramidal lobe, can be present in up to 50% of people, and is usually originate from the isthmus and superiorly extends [3]. Thyroid cancer is caused by follicular and parafollicular cells (C cells). The malignancy potential is from low (papillary/follicular cancer) to aggressive degrees (anaplastic carcinoma) [4]. The main Differential Thyroid Carcinoma (DTC) involves four types; papillary, follicular, medullary, and anaplastic. Most DTC is papillary, followed by follicular, medullary, and anaplastic, sequentially [5]. The thyroid gland is essential for regulating various metabolic functions. Therefore, patients with active thyroid glands have a wide range of hormonal symptoms [6]. Radiographic images assess the morphological features and pathological effects of abnormal thyroid function [7]. The imaging of the thyroid gland can be done in several modalities such as high-resolution Ultrasound (US), Magnetic Resonance Imaging (MRI) [8,9], Computed Tomography (CT), and nuclear medicine. However, the primary methods for assessing thyroid disease depending on clinical history, physical examination, and laboratory tests [10].
Nuclear Medicine can be used to test thyroid gland functionality. There are several methods to scan the thyroid gland in nuclear medicine. The most common method is a gamma camera using Technetium-99m (99mTc) -pertechnetate [11]. The thyroid gland uptake mechanism traps 3-4% of the administered activity. The 75 MBq (2mCi) activity is usually administrated, which gives the right quality image [12]. 99 mTc pertechnetate does not cause further metabolic degradation in thyroid cells. A more physiological method for thyroid imaging involves the radioisotope iodine, which is trapped by follicular cells, usually iodine-123 (123I) and iodine-131 (131I) [13,14].
The Gamma Camera images produce a 2-dimensional (2D) image, which is displayed the distribution of radiopharmaceutical within the thyroid, and it can be improved with a pin-hole collimator [15]. To differentiate between salivary excretion and activity in the thyroid bed, the amount of water should be drunk before the thyroid scan. Certain drugs interfere with absorption mechanisms in the thyroid gland, such as thyroxin, tetroxide, amiodarone, and potassium perchlorate. These medications should be discontinued at variable intervals. Also, Iodinated contrast agents should be avoided before the 70 days of examination because it produces an undesirable sodium-iodide [16].
Radioactive iodine (131I) has been used as an adjuvant treatment for high-risk, well- DTC after thyroidectomy for residual or recurrent thyroid cancer [17,18]. Three different DTC treatment stages should be followed to obtain optimal treatment strategies: the ablation of thyroid tissue, either total ablation or subtotal ablation, postoperative 131I ablation of thyroid remnant, and thyroid hormone administration for suppression treatment [19]. Most patients with DTC have a good prognosis following appropriate treatment. A 90% remission rate can be achieved after receiving treatments that include thyroidectomies and postoperative 131I therapies [10]. Regarding the significance, this study aimed to investigate the treatment efficacy of radioactive iodine therapy on patients after total thyroidectomy and its effect on the quality of life.
METHODS
Study design
A retrospective analysis of 141 thyroid cancer patients undergoing total thyroidectomy admitted to Al-Ahli Hospital at West Bank, Palestine, from January 2018 to November 2019 was performed, including 27 males and 114 females, with an average age of (51.12±10.11) years. All of the following data were obtained age, dose activity ablation, lab tests, number of doses for each patient, gender, image after ablation. The age was sorted in sixth groups; first group (between 20-30 years), second group (between 30-40 years), third group (between 40-50 years), fourth group (between 50-60 years), fifth group (between 60-70 years), and sixth group (between 70-80 years).
All patients confirmed as thyroid cancer by histopathological diagnosis with serum Thyroglobulin (Tg) level ≥10 ng/ml or thyroid cancer recurrence or metastasis. All patients underwent total thyroidectomy and treated with 131I. Patients having undergone radiotherapy and chemotherapy, or have respiratory, digestive, and endocrine diseases. Also, patients with cognitive impairment and communication impairment, and patients who did not cooperate with the examination were excluded. The study was approved ethically by the Ethics Committee of the university collaborated with the Hospital administration.
Treatment methods
The remnant tissue in DTC patients was cured with 131I 2.75-7.4 GBq (74-200 mCi). Before the 131I treatment, all patients should stop the thyroid hormone medications for three weeks for thyroxine and two weeks for T3, to keep the Thyroid-stimulating Hormone (TSH) levels more than 30 uIU / ml). All patients had routine blood tests (TSH, TG, Thyroglobulin Antibodies, Serum (TGAb), and chest radiographs. The dealing with patients was followed as; whole-body iodine (WBI) was obtained before iodine ablation to determine the amount activity for each patient that needs, followed by administration of iodine ablation, and then after six days, the WBI was acquired for the patient. Finally, the WBI followed up after six months.
Treatment efficacy criteria
To evaluate the efficacy of 131I for the treatment of DTC, Tg levels, and 131Itherapeutic dose are included throughout the body. The criteria for the effectiveness of the treatment were as follows; Cure Rate (CR) when the remnant disappeared, and the level of Tg was <2 μg / ml; Improvement Rate (IR) where the remnant tissue shrinkage and resection and Tg levels decreased but remained >2 μg / ml; Non-effective Rate (NR) where the remnant tissue still found but tended to increase in size or increase in number and also no marked changes were shown on the 131I whole-body scan and no change in Tg level.
Statistical analysis
The data were analyzed using SPSS software version 25. The significance level, mean, standard deviation, tables were used to present the demographic data. Pie charts and bar charts were used to present the data in graphical form.
RESULTS
A total of 141 patients were collected retrospectively in this study. The genders of sample distribution between the patients were 27 males (19.1%) and 114 females (80.9%). The most affected age group in the study was found in the second group (30-40) with a percentage of 27.66%, while the lowest percentage was found in the fifth group (60-70) with a percentage of 7.09%, As shown in figure 1.
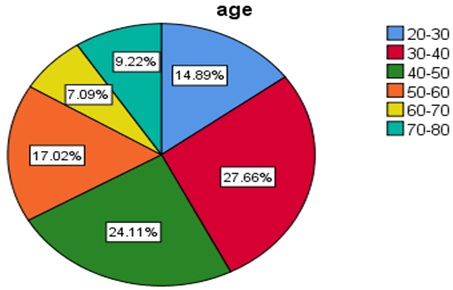 Figure 1: The distributions of the age groups in the sample.
Figure 1: The distributions of the age groups in the sample.
The relationship between age group and number of dose percentage
The study also examined the number of doses given to patients who suffer from DTC to determine the effectiveness of iodine treatment from the first dose, second dose, third dose, and the fourth dose. All cases who took four doses are considered untreated using RAI. Table 1 shows the relationship between doses number exposed to a patient with respect age.
|
|
Age group |
||||||
|
Number of doses |
20-30 |
30-40 |
40-50 |
50-60 |
60-70 |
70-80 |
Total |
|
0* |
0.7% |
0.7% |
2.1% |
- |
0.7% |
0.7% |
4.9% |
|
1 |
12.8% |
24.9% |
15.6% |
14.9% |
6.4% |
7.1% |
81.7% |
|
2 |
0.7% |
0.7% |
6.4% |
1.4% |
- |
1.4% |
10.6% |
|
3 |
- |
1.4% |
- |
0.7% |
- |
- |
2.1% |
|
4 |
0.7% |
- |
- |
- |
- |
- |
0.7% |
Table 1: The relationship between the number of doses and patient age groups.
0*: Patients who underwent RAI in a different hospital and made the follow up at Al-Ahli Hospital. Table 1 showed the highest number of patients were taken a single dose estimated to 81.7%, while the patients who took a double dose is 10.6%, and 2.1% of patients were taken triple doses. Finally, the patients who were not treated were 0.7%, representing patients who were given four-time of doses. Figure 2 shows the treatment efficacy of 131I respected age groups.
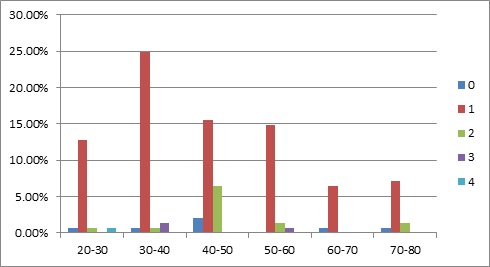 Figure 2: The relationship between the number of doses and age groups.
Figure 2: The relationship between the number of doses and age groups.
Figure 2 shows the highest age group taking a single dose was the second age group (30-40), while the fifth age group (60-70) was the lowest group taking a single dose. It also appears the third age group (40-50) was exposed to a double dose at a greater percentage than other age groups. Finally, the first age group (20-30) is the only group that has been exposed to four doses.
The relationship between the number of doses and age groups in male
Figure 3 explained the percentage of a single dose that is given to the patients was the highest percentage among the number of other doses in the male group. In addition to that, there are no cases that have been exposed to more than two therapeutic doses.
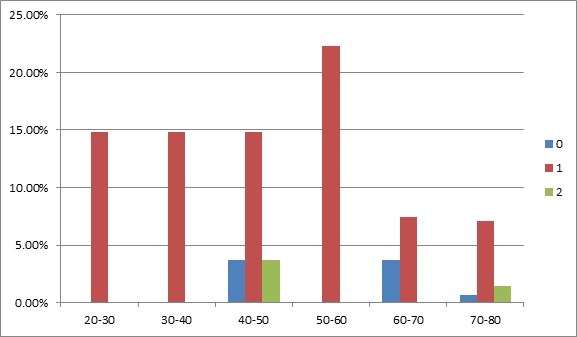 Figure 3: The relationship between the number of doses and age groups in males.
Figure 3: The relationship between the number of doses and age groups in males.
The relationship between the number of doses and age groups in female
Figure 4 explained the percentage of a single dose that is given to the female patients; it shows the highest rate among the number of other doses in the female group. It also shows the highest percentage who exposed a single dose in females was the second group (30-40) with the percentage of 27.1%, and the second dose was prominent compared to the male group. Also, the highest percentage in the second dose was found in the third group (40-50). Moreover, the lowest percentage of doses was noticed in the fifth group (60-70).
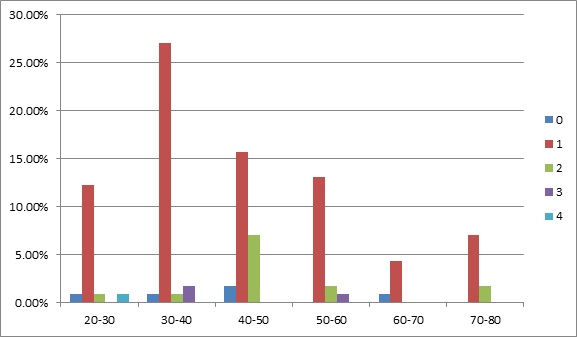 Figure 4: The relationship between the number of doses and age groups in the female.
Figure 4: The relationship between the number of doses and age groups in the female.
The efficacy of iodine treatment for TC patients
To find out the efficacy of iodine treatment for DTC patients, the project was conducted to study the relationship between the numbers of doses given to patients and the number of follow-up for each patient. Table 2 and Figure 5 show this relationship between the number of doses and the number of follow-up examinations.
|
|
F.U 1 |
F.U 2 |
F.U 3 |
F.U 4 |
Total % |
|
D1 |
74.5% |
12.7% |
0.7% |
|
87.9% |
|
D2 |
- |
5.7% |
1.4% |
0.7% |
7.8% |
|
D3 |
- |
- |
2.1% |
1.4% |
3.5% |
|
D4 |
- |
- |
- |
0.7% |
0.7% |
Table 2: The relationship between the number of doses and follow-up examinations.
D1: Single-dose, D2: Double dose, D3: Triple dose, D4: Tetra dose, F.U: Follow up. As shown in Figure 5, the effectiveness of RAI treatment for DTC patients from the first dose was estimated at 87.9%, and this percentage considered the CR, while the cancer recurrence percentage to the patients who underwent double and tri-dose were estimated at 11.3% and these two groups located under IR group. However, the patients who underwent tetra-Iodine dose and followed up with four times whole body iodine scans considered the NR group.
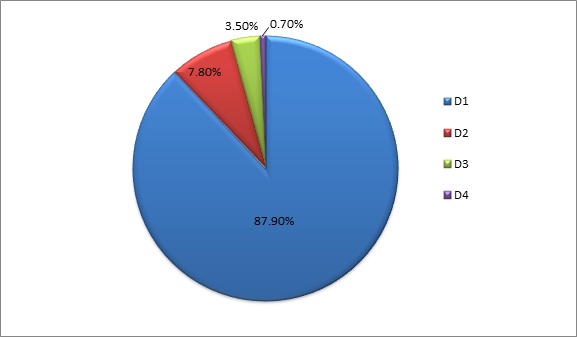 Figure 5: Iodine treatment efficacy in the sample.
Figure 5: Iodine treatment efficacy in the sample.
Figure 6 shows the male group reported significantly more recovery percentage than the female group. It reached 88.89% for patients who underwent a single dose, and 11.11% for patients experienced a double dose. However, the female recovery percentage from an available amount reached to 82.45%. Moreover, the female patients need tri and tetra doses, estimated at 2.63% and 0.87%, respectively.
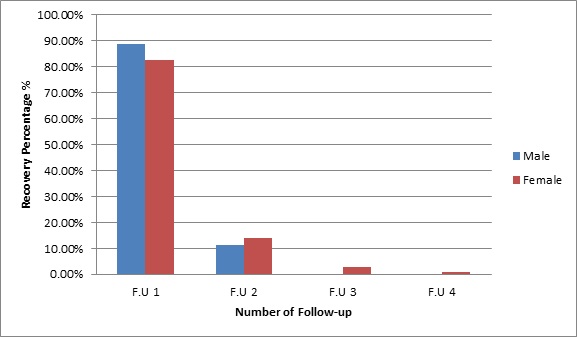 Figure 6: The recovery percentages in the males and females’ group.
Figure 6: The recovery percentages in the males and females’ group.
DISCUSSION
The current study was based on revealing the treatment percentage for DTC patients who underwent surgical thyroidectomy, and they were given radioactive iodine-131 as a complementary treatment procedure. Then they were followed up from 6-12 months after receiving radioiodine treatment. The study estimated the treatment efficacy percentage among male and female patients, where the treatment efficacy was divided into three sections CR, IR, and NR. The study showed that the percentage of treatment CR at ages 30-40 is more than any other age, and the rate of treatment efficiency decreases from the first dose with age. The reason for these findings correlated with treatment sensitivity in adults, while the elderly patients are less sensitive to iatrogenic DTC [20].
The study showed that the cure rate in the sample was 87.9%, while the improvement and non-effective rate was 11.3% and 0.07%, respectively. These results are consistent with previous studies, such as a study of He, Ying et al., where the cure rate estimated the percentage of DTC was 88.07%, and the non-effective rate was 11.93% [19].
The cure rate percentage of treatment in the male group was estimated at 88.89% while the percentage of treatment for females from the first treatment dose was estimated at 82.45%, and this is due to females suffer from hormonal disorders more than males, and also women are more susceptible to genetic risk-factors compared to males likely to develop MEN2 syndrome [21]. These results are consistent with previous studies, such as a study of He, Ying et al. [19], which estimated the percentage of DTC in females with 70.64% compared to DTC incidence in males with 29.36%. The results show the percentage of patients exposed to a single dose was the highest among the other doses, which is consistent with previous studies such as a study by Lee, Stephanie L [22]. He found that 63.2% of the patients need a single dose for treatment, 28.1% required a second treatment, and 8.8% required a third treatment. The number of times the male exposed to is less than the number of females, which indicates that the treatment in men is higher than in the female.
In reviewing the literature, some articles were found on the association between gender and recovery rate for DTC patients. They found different results than we showed like Shi et al. and Y.H Lee et al. studies. The found that Recurrence and death were more common in male patients with PTC than in female patients with thyroid carcinoma [23,24]. In any case, the current study suffered some limitations represented in not documenting all the serum Tg tests for all patients, and testing the relationship between it and the disease recurrence on one side and between it and efficiency treatment on the other hand. The other matter is that patients from other hospitals have not previously documented the number of times their dose was taken. Finally, the activity amount for every single dose was not calculated for each patient separately, and therefore the accuracy of treatment did not calculate precisely.
CONCLUSION
Surgery followed by radioiodine has remained the treatment of choice over the last six decades in DTC with a favorable outcome. The presence of remnant thyroid tissue after total thyroidectomy is problematic challenging, especially in DTC patients for RAI ablation. Postoperative Tg levels are a sensitive and reliable indicator of the presence of remnant thyroid tissue. According to the results of our study, females have more risk than males for DTC. Besides, the prognostic value for the female is lower than male. Also, the middle age group between 30-50 is the more affected group. Finally, the patients with well-differentiated DTC with distant metastases have poor prognoses after long-term follow-up.
ACKNOWLEDGEMENTS
Special thanks to Al-Ahli Hospital for their fruitful encouragement that facilitate our study.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- Hopkins CR, Reading CC (1995) Thyroid and parathyroid imaging. Seminars in Ultrasound, CT and MRI 16: 279-295.
- Price DC (1993) Radioisotopic evaluation of the thyroid and the parathyroids. Radiol Clin North Am 31: 991-1015.
- Braun EM, Windisch G, Wolf G, Hausleitner L, Anderhuber F (2007) The pyramidal lobe: clinical anatomy and its importance in thyroid surgery. Surg. Radiol. Anat 29: 21-27.
- Arrangoiz R, Cordera F, Caba D, Moreno E, Luque-de-Leon E, et al. (2019) Thyroid Cancer. Int J Otolaryngol Head Neck Surg 8: 217-270.
- Hedinger C (2012) Histological typing of thyroid tumours. Springer Science & Business Media.
- Loevner LA (1996) Imaging of the thyroid gland. Seminars in Ultrasound, CT and MRI 17: 539-562.
- Guerra G (2014) Morphological, diagnostic and surgical features of ectopic thyroid gland: a review of literature. Int J Surg 12: S3-S11.
- Ahmad MS (2020) A Recent Short Review in Non-Invasive Magnetic Resonance Imaging on Assessment of HCC Stages: MRI Findings and Pathological Diagnosis. J Gastroenterol Hepatol Res 9: 3113-3123.
- Ahmad MS (2019) Current Status Regarding Tumour Progression, Surveillance, Diagnosis, Staging, and Treatment Of HCC A Literature Review. J Gastroenterol Hepatol Res 8: 2841-2852.
- Dal Maso L (2017) Survival of 86,690 patients with thyroid cancer: a population-based study in 29 European countries from EUROCARE-5. Eur J Cancer 77: 140-152.
- Fjeld JG, Erichsen K, Pfeffer PF, Clausen OPF, Rootwelt K (1997) Technetium-99m-tetrofosmin for parathyroid scintigraphy: a comparison with sestamibi. J Nucl Med 38: 831-834.
- Khan SU, Khan AU, Khan A, Shah AS, Khan K (2011) Extrathyroidal uptake from thyroid carcinoma on 99m Tc-pertechnetate scintigraphy. J Coll Physicians Surg Pak 21: 772-774.
- Van Nostrand D (2009) The utility of radioiodine scans prior to iodine 131 ablation in patients with well-differentiated thyroid cancer. Thyroid 19: 849-855.
- Ahmad MS, Zeyadeh SL, Odah R, Oglat A (2019) Occupational Radiation Dose for Medical Workers atAl-Ahli Hospital in West Bank-Palestine. J Nucl Radiol Radiat Ther 5: 1259-1266.
- Ryo UY (1976) Thyroid scintigram: sensitivity with sodium pertechnetate Tc 99m and gamma camera with pinhole collimator. Jama 235: 1235-1238.
- Sarkar SD (2006) Benign thyroid disease: what is the role of nuclear medicine? Seminars in nuclear medicine 36: 185-193.
- Meier DA (2002) Procedure Guideline for Therapy of Thyroid Disease with 131 Iodine. 43: 856-862.
- Urken ML (2015) Management of recurrent and persistent metastatic lymph nodes in well?differentiated thyroid cancer: A multifactorial decision?making guide for the thyroid cancer care collaborative. Head Neck 37: 605-614.
- He Y, Pan M, Huang J, Xie X, Zhang F, et al. (2016) Iodine-131?: An Effective Method for Treating Lymph Node Metastases of Differentiated Thyroid Cancer. Med Sci Monit 4924-4928.
- Ajish TP, Jayakumar RV (2012) Geriatric thyroidology?: An update. Indian J Endocrinol Metab 16: 542.
- El-maouche D, Welch J, Agarwal SK, Weinstein LS, William F (2017) HHS Public Access. Int J Endocr Oncol 3: 89-95.
- Lee SL (2010) Complications of Radioactive Iodine Treatment of Thyroid Carcinoma. J Natl Compr Canc Netw 8: 1277-1286.
- Shi L, Liu J, Yu L, Lei Y, Leng SX, et al. (2018) Clinic-pathologic Features and Prognostic Analysis of Thyroid Cancer in the Older Adult?: A SEER Based Study. Journal of Cancer 9: 2744-2750
- Lee YH, Lee YM, Sung TY, Yoon JH, Song DE (2017) Is Male Gender a Prognostic Factor for Papillary Thyroid Microcarcinoma?? Ann Surg Oncol 24: 1958-1964.
Citation: Mohammad M, Ahmad MS, Mudalal M, Bakry A, Arzeqat T (2020) The Radioactive Iodine (I-131) Efficiency for the Treatment of Well-differentiated Thyroid Cancer. J Nucl Med Radiol Radiat Ther 5: 025.
Copyright: © 2020 Modallal Mohammad, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.